Discoid lupus erythematosus (DLE) is twice as common in women and is more common in African Americans. Conversion to systemic lupus erythematosus (SLE) is uncommon (5%), but in some cases discoid lupus-like lesions are the initial cutaneous sign of SLE.1 Approximately 25% of patients with SLE will have discoid lupus lesions at some point in their disease.
The primary lesion is an angular, plaque with “follicular plugging,” central atrophy and peripheral hyperpigmentation, and erythema (Figures 24-1 and 24-2).1 Pruritus or burning are common symptoms. The lesions are primarily located on sun-exposed areas, generally the face, arms, scalp, upper chest, and back. Conchal fossa (bowl) scarring of the ear is almost pathognomonic (Figure 24-3). The scarring lesions of DLE may be disfiguring in patients with darker skin pigmentation, leaving permanent hypo- or hyperpigmentation. Scalp lesions may result in permanent hair loss due to scarring alopecia. Variants of DLE include hypertrophic, diffuse, and tumid, the latter two being less common.



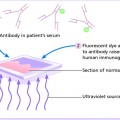
Antinuclear antibody (ANA), if present, is most often low titer. A skin biopsy of a lesion for direct immunofluorescence shows a positive lupus band (IgG, IgM, and C3 in a band-like pattern along the dermal-epidermal junction) in most patients.1
✓ Seborrheic dermatitis, psoriasis, other photosensitive dermatoses, and tinea faciei.
Mild to moderate limited disease can be treated with topical steroids or calcineurin inhibitors. Oral antimalarials such as hydroxychloroquine can be added for more widespread disease or disease that is disfiguring.2 Methotrexate, prednisone, and other systemic immunomodulators are other options for systemic therapy. Sunscreens, hats, and sun protective clothing should be regularly used.
Subacute cutaneous lupus erythematosus (SCLE) like all connective tissue diseases is somewhat more common in women than in men.
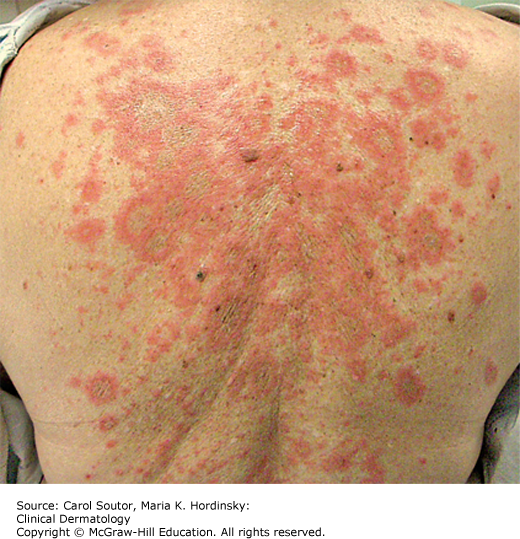
SCLE presents with a sudden onset of figurate, annular, arcuate, or psoriasiform lesions that are typically nonscarring and nonatrophic in a photodistribution (face, neck, extensor arms); however, the upper trunk is also commonly affected (Figure 24-4). Systemic symptoms are frequently absent or of minimal intensity. SCLE is often drug induced and can persist long after the causative drug has been withdrawn.1
ANA usually is positive (>60%).1 Antibodies to Ro/SS-A are positive in more than 80% of patients. A skin biopsy for direct immunofluorescence will demonstrate a positive lupus band test in more than 60% of patients.
✓ Tinea corporis, psoriasis, and dermatomyositis.
Any potentially inciting drug should be discontinued if possible. Many patients will require medications similar to those used in DLE.2 Sun protection is also very important.
Systemic lupus erythematosus is the multisystem (systemic) extension of DLE and SCLE, not a part of a seamless continuum of those diseases. Women constitute 85% of those affected.
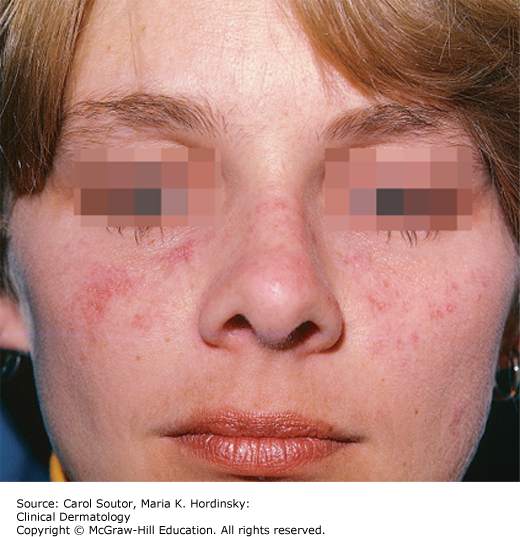
Skin symptoms are minimal and usually consist of pruritus or increased sun sensitivity. Systemic symptoms are common and include arthralgias, myalgias, fatigue, malaise, fevers, chills, night sweats, weight loss, headaches, visual changes, and diffuse hair loss. Raynaud’s symptoms are common. Cutaneous lesions though sometimes “discoid lupus” like, are generally diffuse, nonscarring and often nondescript. The “butterfly rash” (erythema with fine scale over the malar area) is one of the criteria for the diagnoses of SLE (Figure 24-5).1
A positive, high titer ANA is present in more than 95% of patients. The presence of anti-Sm and rRNP antibodies is characteristic of SLE. The white blood cell count is often low (4000/mm3) with anemia frequent. Drug-induced disease may be detected by antihistone antibody testing. A positive lupus band is present in 90% of skin biopsies from involved skin.
✓ Dermatomyositis, contact dermatitis, and other photosensitizing diseases.
Treatment is generally systemic. Hydroxychloroquine,2 prednisone, methotrexate, biologic agents, plasmapheresis, and immunomodulators are frequently indicated. Sun protection is important.
Patients with skin lesions of discoid, subacute cutaneous, or systemic lupus are often co-managed by rheumatology and dermatology recognizing the distinct skills of each specialist.
Lupus foundation of America, Inc.: www.Lupus.org
National Institute of Arthritis and Musculoskeletal and Skin Diseases: www.niams.nih.gov/Health_Info/Lupus/
Dermatomyositis is a rare chronic immune-mediated disorder that affects the skin and/or proximal skeletal muscles. The diagnosis of cutaneous dermatomyositis is often missed or delayed, because the pruritus and rash associated with it are very similar to other forms of dermatitis. Patients with dermatomyositis have an increased risk of malignancy.3
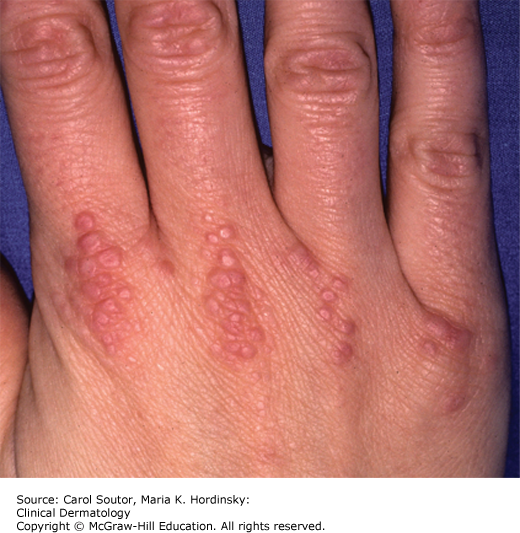
Intensely pruritic, diffuse, scaly erythematous patches in the scalp with postauricular erythema are characteristic findings.3 Similar patches are often found on the upper back shoulders, upper chest (shawl sign), and deltoid regions. Pathognomonic findings include periorbital erythema (heliotrope) and violaceous papules over the joints of the dorsal hands (Gottron’s papules) (Figure 24-6). Periungual erythema may be present. Patients may complain of photosensitivity and proximal muscle weakness (eg, difficultly in climbing stairs or raising arms above the head).
Most patients have an elevated ANA and myositis-specific antibodies, including Jo-1 and Ro/SSA.3 Patients with muscle disease usually have an elevated creatine phosphokinase (CK) and aldolase.
Pruritic erythematous scaly patches on scalp and upper chest and shoulders with or without proximal muscle weakness. Pathognomonic findings of Gottron’s papules and heliotrope may be present.
✓ Lupus erythematosus (especially subacute cutaneous), seborrheic dermatitis, and contact dermatitis.
Antihistaminics (H1 and H2) and doxepin can be used for symptomatic relief of pruritus. Topical steroids and topical pimecrolimus and tacrolimus may partially control the skin disease. Most patients with moderate to severe disease require systemic steroids or other systemic immunomodulating agents.3 Management also includes an age and gender appropriate workup for malignancy (eg, ovarian, cervical, prostate, lung, colon, and breast) and evaluation for muscle involvement including electromyography (EMG) and muscle biopsy.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


