Techniques for abdominal contouring have proliferated and evolved over the past 2 decades. Now more than ever, aesthetic operations are tailored to fit the anatomic features and aesthetic goals of each individual patient, stressing the absolute importance of patient selection. This short scar procedure relies on a combination of liposuction and modified skin resection and muscle tightening in the lower abdomen. It has been the author’s experience that this results in a more rapid recovery in most patients. It is almost always performed in conjunction with liposuction of the posterior trunk to achieve a harmonious recontouring of the aesthetic unit of the trunk. The techniques employed are familiar to all plastic surgeons performing body contouring procedures. Patient selection is the absolute key to achieving successful outcomes. Short scar abdominoplasty results in significant contour improvement in the properly selected patient. The procedure relies on a combination of liposuction and modified excisional surgery to produce the desired outcome.
Techniques for abdominal contouring have proliferated and evolved over the past 2 decades because of the integration of liposuction into the procedures of full and limited abdominoplasty as influenced by the contributions of surgeons such as Ted Lockwood and Osvaldo Saldahna. Furthermore, there is universal recognition among aesthetic plastic surgeons that abdominal contour improvement is really one component of a 3-dimensional contouring of the trunk and that all abdominoplasty procedures must be viewed from this prospective. Now more than ever, aesthetic operations are tailored to fit the anatomic features and aesthetic goals of each individual patient, stressing the absolute importance of patient selection.
From my (the author of this article) perspective, one of the hallmarks of the exceptional aesthetic surgeon is someone who has an “aesthetic vision” for goals that be achieved and can select the most minimal operation to deliver the desired result in a given situation. This hallmark holds true in aesthetic surgery of the face (an area where Daniel Baker’s teaching has had a dramatic influence), the breast, and trunk region.
At present the majority (approximately 85%) of my abdominal contouring practice involves a full abdominoplasty, a procedure with selective undermining, musculofascial plication, and the application of liposuction to the abdominal flap (and adjacent contours) done through a long incision incorporating the high lateral tension abdominoplasty procedure introduced by Lockwood, because in my experience most patients presenting for contour enhancement surgery of the trunk are best served by it.
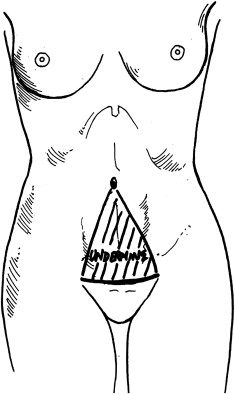
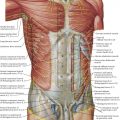
However, there continues to be a small segment of patients (15%) who present with concerns related to the lower abdomen and deformities primarily marked by adipose tissue excess on the abdominal wall, and muscle laxity and skin excess limited to the lower abdomen. These patients tend to be young (in their third and fourth decade of life), nulliparous, and generally in good physical shape, with an active lifestyle marked by regular exercise. Such patients can often achieve excellent improvement with aggressive liposculpture of the abdominal wall coupled with infraumbilical musculofascial plication and excision of lower abdominal skin excess ( Fig. 1 ) done through a relatively short suprapubic incision—a procedure I have previously described as a “marriage abdominoplasty.” This term was coined to denote the power that can be derived from combining or “marrying” aggressive abdominal liposculpture with modified surgical techniques in patients who are candidates for it. The procedure was derived from the contributions of previous surgeons with the incorporation of liposuction as an increasingly important component.
Patient selection and classification of deformity
The procedure of short scar abdominoplasty, lower abdominoplasty, or marriage abdominoplasty does not treat upper abdominal skin excess or patients with significant upper abdominal musculofascial laxity, therefore patients presenting with these features on physical examination are not candidates for it. This selection will exclude the majority of patients presenting for abdominal contouring in most plastic surgeons’ practices.
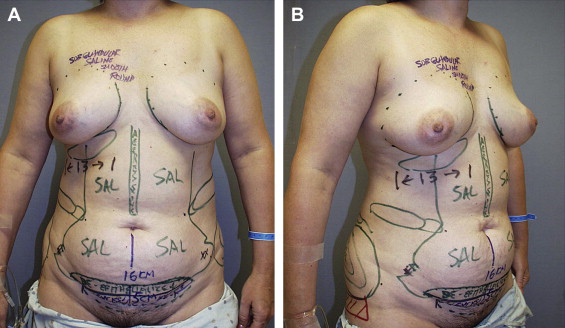
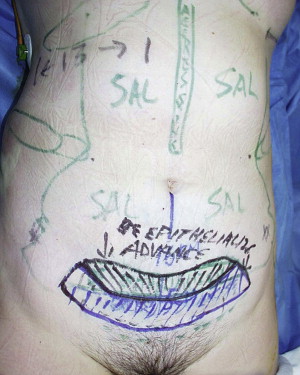
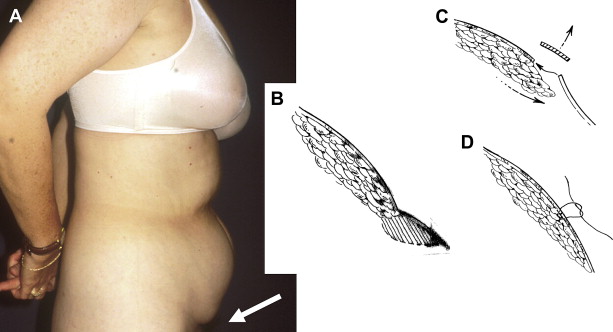
Favorable candidates are those who are nonsmoking and in good health, with stable weight over several months, and whose contour abnormality is predominantly adipose excess. The adipose excess is usually located between the linea semi-lunaris lines on the abdominal wall, but frequently there is excess adipose tissue accumulation on the posterior trunk including the hips, flanks, and back region. These areas are routinely treated by liposuction during most abdominoplasty procedures. Patients frequently have existing suprapubic incisions following a cesarean section or other gynecologic procedure resulting in a “step-off” in contour between the abdomen and suprapubic region ( Fig. 2 ). This step-off is readily addressed by a short scar abdominoplasty by excising the scar, elevating the mons pubis area slightly, and advancing the “de-epithelialized” lead edge of the abdominal flap (that would otherwise be discarded) beneath the tissues of the pubic region ( Figs. 3 and 4 ).
A careful history is obtained to clarify the patient’s goals and expectations. Patients presenting with striae as their main concern are not likely to be improved with this procedure, which entails a relatively small (rarely >7 cm) excision of vertical skin excess. Patients with even the smallest amount of supraumbilical skin excess will generally not notice any improvement in this skin excess with the standard version of the procedure in which there is no incision around the umbilicus. For this reason a careful examination of the abdomen from an aesthetic standpoint is an essential first step in allowing the surgeon to classify the patient’s deformity preoperatively. Several abdominoplasty classifications have been proposed but the most straightforward is that put forth by Matarasso ( Table 1 ). Addressing supraumbilical skin excess may be possible with transection of the umbilical stalk (floating the umbilicus) advancing, and fixing it at a slightly lower level. Probably the biggest source of disappointment in patients undergoing lower abdominoplasty or “marriage abdominoplasty” is upper abdominal skin excess in the form of transverse folds of periumbilical skin wrinkling. This appearance is not addressed by the surgery even with procedures that “float” the umbilicus.
Related posts:
 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


