Key Words
HPV, HIV, herpes, viral infections, STIs, molluscum contagiosum, Bowenoid papulosis, papillomavirus, neonatal herpes, suppressive therapy
Genital Warts
Virus Types
Human papillomavirus (HPV) causes warts and anogenital malignancy. HPV can reside in epithelial basal cells and lead to subclinical or latent infection. Numerous types of HPV viruses have been identified. These HPV types also are categorized into low-, intermediate-, and high-risk groups. Detection of high-risk genotypes ( n = 13) from genital specimens is considered a major determinant associated with the development of cervical cancer. HPV-16 and HPV-18 are regarded as high-risk cancer-associated HPVs; HPV types 6 and 11 are considered low-risk; and HPV types 31, 33, and 35 have an intermediate association with cancer. These seven HPV types are found in about 70% of cervical neoplasms. Additional HPVs including types 42, 43, 44, 45, 51, 52, 56, 58, 59, and 68 have been identified as the principal HPVs detected in the remaining lesions. Bowenoid papulosis is most commonly caused by HPV-16. The rare verrucous carcinoma (Buschke–Löwenstein tumor) that resembles a large wart is locally aggressive but rarely metastatic. It is associated with HPV-6 and HPV-11.
Incidence
HPV is the most common sexually transmitted disease (STD) with a prevalence of 42.5% among adults 18 to 59 years old in the United States. Most infected individuals are asymptomatic and clear the infection spontaneously within a few years. Persistent infections with HPV (HPV-16 and -18 account for 66% of cervical cancer in the United States) cause cancer and genital warts (HPV-6 and -11 account for 90% of genital warts). l
Regression and Persistence
HPV infections are usually transient and tend to undergo spontaneous regression. Approximately 70% of women are HPV DNA undetectable at 12 months after HPV infection detection, and more than 80% are clear at 18 months.
Cell-mediated immunity controls latent HPV infection and mediates the regression of HPV-induced lesions. Patients who are immunocompromised because of a decrease in cell-mediated immunity are at increased risk of developing and failing to eradicate HPV-related disease. This includes organ transplant patients receiving immunosuppressive treatment and patients with human immunodeficiency virus (HIV) infection. After wart eradication, patients may continue to have latent virus in their anogenital epithelium, and it is not known whether HPV is sufficiently infectious to allow transmission in this stage of development.
Risk
The immune status has an impact on the disease course and response to treatment. Cigarette smoking is linked to the risk of anogenital warts. Men who smoke more than 10 cigarettes per day are twice as likely to have anogenital warts as men who do not smoke cigarettes. There is a 3-fold increase in the incidence of anogenital warts in women who are smokers. The increased rate of progression of anogenital warts in smokers may reflect immune modulation effects induced by cigarettes. HIV patients have increased rates of HPV infection (prevalence 31% to 57%), with increased duration. The incidence of anogenital HPV infection is increased 17-fold in renal transplant patients.
Transmission
Risk factors for acquisition of condyloma in women have been identified as the number of sexual partners, frequency of sexual intercourse, and presence of warts on the sexual partner. Transmission of HPV during infant delivery may rarely occur. Between 60% and 85% of sexual partners of patients with warts will develop anogenital warts within 6 weeks to 8 months. Visible warts appear after an average of 2.9 months after contact. Transmission may then occur to new partners during this latency period.
Among newly sexually active women, consistent condom use by their partners appears to reduce the risk of cervical and vulvovaginal HPV infection. Subclinical HPV infections may occur at epithelial sites outside of the area covered by a latex condom (i.e., the scrotum and vulva and the suprapubic and perianal areas).
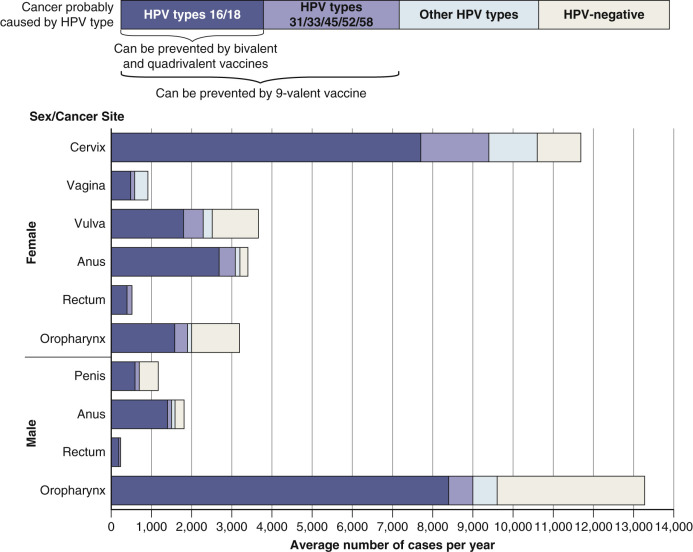
Development of Intraepithelial Neoplasia and Cervical, Penile, Vulvar, Anogenital, and Oropharyngeal Cancers.
According to the CDC, HPV causes more than 90% of anal and cervical cancer and greater than 50% of vaginal, vulvar and penile cancers ( Fig. 11.1 ). Approximately 15% to 28% of HPV DNA-positive women developed cervical squamous intraepithelial neoplasia within 2 years. The risk of progression for HPV types 16 and 18 is greater (approximately 40%) than that for other HPV types. Male circumcision is associated with a reduced risk of penile HPV infection and, in the case of men with a history of multiple sexual partners, a reduced risk of cervical cancer in their current female partners.
Genital warts in rare cases degenerate into squamous cell carcinoma (SCC). Nearly 30% of vulvar carcinomas are associated with or preceded by condylomata. Men having sex with men who have anal condylomata have a 50-fold relative risk for developing anal cancer. HPV can lead to malignant anogenital lesions of the cervix, vulva, anus, and penis. HPV-induced oropharyngeal cancer incidence is increasing at alarming rates and is now the primary cause of oropharyngeal cancer. Individuals are affected at younger ages, especially men between ages 40 and 70.
Clinical Presentation
Genital warts (condylomata acuminata or venereal warts) are pale pink with numerous, discrete, narrow-to-wide projections on a broad base ( Figs. 11.2 to 11.17 ![]() ). The surface is smooth or velvety and moist, and lacks the hyperkeratosis of warts found elsewhere. The warts may coalesce in the rectal or perineal area to form a large, cauliflower-like mass. Perianal warts may be present in persons who do not practice anal sex.
). The surface is smooth or velvety and moist, and lacks the hyperkeratosis of warts found elsewhere. The warts may coalesce in the rectal or perineal area to form a large, cauliflower-like mass. Perianal warts may be present in persons who do not practice anal sex.


















Another type is seen most often in young, sexually active patients. Multifocal, often bilateral, red- or brown-pigmented, slightly raised, smooth papules have the same virus types seen in exophytic condylomata, but in some instances these papules have histologic features of Bowen disease. (See discussion of bowenoid papulosis later in this chapter.)
Warts spread rapidly over moist areas and may therefore be symmetric on apposing surfaces of the labia or rectum (see Fig. 11.16 ). Common warts can possibly be the source of genital warts, although they are usually caused by different subtypes of virus. Warts may extend into the vaginal tract, urethra, and anal canal or the bladder, in which case a speculum or sigmoidoscope is required for visualization and treatment. Condylomata may spontaneously regress, enlarge, or remain unchanged. Genital warts frequently recur after treatment. There are two possible reasons: (1) latent virus exists beyond the treatment areas in clinically normal skin; and (2) warts that are flat and inconspicuous, especially on the penile shaft and urethral meatus, escape treatment.
Oral Condylomata in Patients With Genital Human Papillomavirus Infection
One study showed that 50% of patients with multiple and widespread genital HPV infection who practiced orogenital sex have oral condyloma. All lesions were asymptomatic. Magnification was necessary to detect oral lesions. The diagnosis was confirmed by biopsy. The tongue was the site most frequently affected. Oral condylomata appeared as multiple, small, white or pink papules, sessile or pedunculate, and as papillary growths with filiform characteristics ( Figs. 11.18 and 11.19 ). The size of oral lesions was greater than 2 mm in more than 50% of lesions, and in 61% of cases more than five lesions were present. HPV-16, HPV-18, HPV-6, and HPV-11 were found. HPV-16 is the principle cause of oropharyngeal cancer (see above).


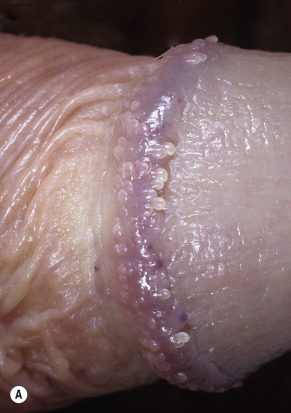
Pearly Penile Papules
Dome-shaped or hair-like projections, called pearly penile papules, appear on the corona of the penis and sometimes on the shaft just proximal to the corona in up to 10% of male patients. These small angiofibromas are normal variants but are sometimes mistaken for warts. No treatment is required ( Fig. 11.20 ).

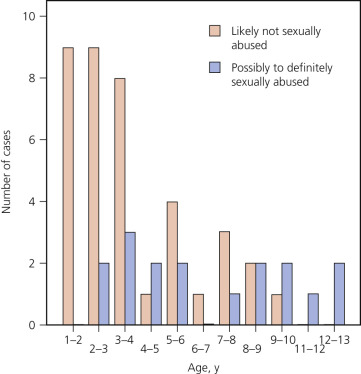
Genital Warts in Children
The prevalence of anogenital condyloma in childhood is not known. HPV infection can be transmitted via sexual and nonsexual means. Nonsexual transmission can occur before birth, during birth or after birth. Vertical transmission from the mother may result in anogenital condylomata and laryngeal papillomas. The incubation of HPV is thought to be three weeks to several months. Older children with anogenital condylomata are more likely to have been sexually abused ( Fig. 11.21 ). Many factors including statements by children, parents, and providers need to be taken into consideration when deciding to file a report of sexual abuse. Providers specializing in child abuse must be consulted if there is any doubt. The presence of a first episode of anogenital warts over the age of 4 and especially over the age of 8 years, with no known source of infection, warrants further investigation.
Diagnosis
A clinical diagnosis can be made in most cases. The differential diagnosis includes seborrheic keratoses, nevi, molluscum contagiosum, and pearly penile papules. Biopsy suspicious lesions.
Viral Typing Using Standard Cervical Screening Specimens.
For patients with “atypical squamous cells of unknown significance” (ASCUS) on Papanicolaou (Pap) smear, HPV typing may be used to determine the need for colposcopy. Cervical swab specimens are submitted. A positive result indicates the presence of HPV DNA attributable to one or more of the following genotypes of the virus: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. Patients who are positive for these high-risk HPV type are referred for colposcopy.
Vaccination.
Boys and girls aged 9 to 14 should receive 2 shots 6 to 12 months apart; if children are older than age 14, three shots are given over 6 months, and individuals with immunocompromising conditions aged 9 through 26 should receive a 3-shot regimen. The Gardasil vaccine is recommended for women through age 26 and men through age 21 for the prevention of cervical cancer, precancerous or dysplastic lesions, and genital warts caused by HPV types 6, 11, 16, and 18. Gardasil 9 protects against cancers caused by HPV types 16, 18, 31, 33, 45, and 58, and is used for prevention of genital warts caused by HPV types 6 and 11.
Treatment
A detailed overview of treatment is provided in Table 11.1 and Box 11.1 .
| Coverage | Recommended Regimen | Alternative Regimen | Special Considerations |
|---|---|---|---|
| Human papillomavirus anogenital warts | Patient-applied:
| Provider-administered for external genital warts:
|
|
| Human papillomavirus urethral meatus warts |
| ||
| Human papillomavirus vaginal, cervical, and intra-anal warts |
|
| |
| Hepatitis A |
| ||
| Hepatitis B |
|
|
Venereal Warts
Chemical (Self-Applied by Patient)
- •
Podophyllotoxin 0.5% solution or gel, twice daily for 3 days, followed by 4 days of no treatment; the cycle can be repeated up to four times (total volume of podophyllotoxin should not exceed 0.5 mL/day). OR
- •
Imiquimod 5% cream applied with a finger at bedtime, left on overnight, three times a week for as long as 16 weeks. The treatment area should be washed with soap and water 6 to 10 hours after application. Hands must be washed with soap and water immediately after application.
- •
The safety of both podophyllotoxin and imiquimod during pregnancy has not been established.
Chemical (Provider Administered)
- •
Podophyllin, 10% to 25% in compound tincture of benzoin, is applied carefully to the warts, avoiding normal tissue. External genital and perianal warts should be washed thoroughly 1 to 4 hours after the application of podophyllin. Podophyllin applied to warts on vaginal or anal epithelial surfaces should be allowed to dry before the speculum or anoscope is removed. Treatment should be repeated at weekly intervals.
- •
Where available, podophyllotoxin 0.5%, one of the active constituents of podophyllin resin, is recommended. Its efficacy is equal to that of podophyllin, but it is less toxic and appears to cause less erosion.
- •
Some experts advise against the use of podophyllin for anal warts. Large amounts of podophyllin should not be used because it is toxic and easily absorbed. Its use during pregnancy and lactation is contraindicated. OR
- •
Trichloroacetic acid (TCA) 80% to 90%, applied carefully to the warts, avoiding normal tissue, followed by powdering of the treated area with talc or sodium bicarbonate (baking soda) to remove unreacted acid. Repeat application at weekly intervals.
Physical
- •
Cryotherapy with liquid nitrogen, solid carbon dioxide, or a cryoprobe. Repeat applications every 1 to 2 weeks. OR
- •
Electrosurgery OR
- •
Surgical removal
Vaginal Warts
- •
Cryotherapy with liquid nitrogen OR
- •
Podophyllin 10% to 25%. Allow to dry before removing speculum. OR
- •
TCA 80% to 90%
Cervical Warts
Treatment of cervical warts should not be started until the results from a cervical smear test are known. Most experts advise against the use of podophyllin or TCA for cervical warts.
- •
Management should include consultation with an expert.
- •
Pap smear
- •
No TCA or podophyllin
Meatal and Urethral Warts
Accessible meatal warts may be treated with podophyllin 10% to 25%, in compound tincture of benzoin, or podophyllotoxin 0.5%, where available. Great care should be taken to ensure that the treated area is dry before contact with normal, apposing epithelial surfaces is allowed. Low success rates with podophyllin are reported. Urethroscopy is necessary to diagnose intraurethral warts, but they should be suspected in men with recurrent meatal warts. Some experts prefer electrosurgical removal. Intraurethral instillation of a 5% cream of fluorouracil or thiotepa may be effective, but neither has been adequately evaluated. Podophyllin should not be used. Recommended treatments:
- •
Cryotherapy OR
- •
Podophyllin 10% to 25%






HPV cannot be completely eliminated because of the surrounding subclinical HPV infection. Removal of visible lesions decreases viral transmission. All treatment methods are associated with a high rate of recurrence that is likely related to surrounding subclinical infection. Therapies with antiviral/immunomodulatory activity (e.g., imiquimod cream) may be associated with lower recurrence rates.
Management of Sexual Partners
Examination of sexual partners is not necessary for the management of genital warts because the role of reinfection is probably minimal. Many sexual partners have obvious warts and may desire treatment. The majority of partners are probably already subclinically infected with HPV, even if they do not have visible warts. The use of condoms may reduce transmission to partners likely to be uninfected, such as new partners. HPV infection may persist throughout a patient’s lifetime in a dormant state and become infectious intermittently. Whether patients with subclinical HPV infection are as contagious as patients with exophytic warts is unknown. One study showed that the failure rate of treating women with condylomata acuminata did not decrease if their male sexual partners were also treated.
Pregnancy
The use of podophyllin and podofilox is contraindicated during pregnancy. Genital papillary lesions have a tendency to proliferate and to become friable during pregnancy. Many experts advocate the removal of visible warts during pregnancy. HPV-6 and HPV-11 can cause laryngeal papillomatosis in infants. The route of transmission is unknown, and laryngeal papillomatosis has occurred in infants delivered by cesarean section. Cesarean delivery should not be performed solely to prevent transmission of HPV infection to the newborn. In rare instances, cesarean delivery may be indicated for women with genital warts if the pelvic outlet is obstructed or if vaginal delivery would result in excessive bleeding.
Children
Spontaneous resolution of pediatric condylomata occurs in more than half of cases in 5 years. Nonintervention is a reasonable initial approach to managing venereal warts in children.
Patient-Applied Therapies
Carefully explain how to use the medication. Be sure that patients can identify the lesions and understand the extent of the disease.
Imiquimod.
Imiquimod is available as a 5% and a 3.75% cream (see the Formulary) in conveniently packaged small dose packs. Clearance rates are 40% to 70%, and there are lower recurrence rates. Improved efficacy and lower recurrence rates occur with imiquimod by inducing the body’s own immunologic defenses. Imiquimod has an immunomodulatory effect and does not rely on physical destruction of the lesion. It has antiviral properties by induction of cytokines. Imiquimod enhances cell-mediated cytolytic activity against HPV. The cream is applied at bedtime every other day and up to five times per week if tolerated, for a maximum of 16 weeks. Patients use a finger to apply the medication into the anal canal for anal warts. On the morning after application, the treated area should be cleansed. Side effects are erythema, swelling, erosions, weeping, crusting, scaling, itching, and burning. Imiquimod may induce local hyper- or hypopigmentation. Wart clearance occurs by 8 to 10 weeks, or earlier. Systemic reactions have not been reported. Imiquimod has not been studied for use during pregnancy. Imiquimod cream is safe to use in organ transplant patients. It is effective in HIV patients even with low CD4 counts.
Podofilox.
Podofilox, also known as podophyllotoxin, is the main cytotoxic ingredient of podophyllin. Podophyllotoxin arrests mitosis and causes destruction of wart tissue within a few days, but can cause damage to surrounding skin. Podofilox gel and solution is available for self-application and is useful for responsible, compliant patients. Patients are instructed to apply the medication to their external genital warts twice each day for 3 consecutive days, followed by 4 days without treatment. Minimize application to normal surrounding skin. No wash off is required between applications. The solution is not used for vulvar, introital, and anal warts. It is recommended that no more than 10 cm 2 of wart tissue should be treated in a day and the total volume of podofilox should be limited to 0.5 mL/day. This cycle is repeated at weekly intervals for a maximum of 4 to 6 weeks. Approximately 15% of patients report severe local reactions to the treatment area after the first treatment cycle; this is reduced to 5% by the last treatment cycle. Local adverse effects of the drug, such as pain, burning, inflammation, and erosions, have occurred in more than 50% of patients. Podofilox is not recommended for perianal, vaginal, or urethral warts and is contraindicated in pregnancy.
Green Tea Sinecatechins (Veregen Ointment).
The topical ointment sinecatechin (Veregen) is used for treatment of external genital and perianal warts. This ointment is approved for use in immunocompetent patients 18 years of age and older. Clearance rates range from 54% to 65% with recurrence occurring in approximately 5.9% to 12% of cases. Side effects are mild and include erythema, pruritus or burning, pain, superficial ulceration, and edema. Erosion, erythema, and ulceration correlate with higher clearance rates. Local reactions occur with highest intensity between weeks 2 and 4. Polyphenon E ointment should be applied three times daily and it is not necessary to wash off the ointment.
Provider-Administered Therapies
Cryosurgery.
Liquid nitrogen delivered with a probe, as a spray, or with a cotton applicator is very effective for treating smaller, flatter genital warts. It is too painful for patients with extensive disease. Exophytic lesions are best treated with excision, imiquimod, or podofilox. Warts on the shaft of the penis and vulva respond very well, with little or no scarring. Cryosurgery of the rectal area is painful. A conservative technique is best. Freeze the lesion until the white border extends approximately 1 mm beyond the wart. Overaggressive therapy causes pain, massive swelling, and scarring.
A blister appears and erodes to form an ulcer in 1 to 3 days, and the lesion heals in 1 to 2 weeks. Repeat treatment every 2 to 4 weeks as necessary. Two to three sessions may be required.
Use EMLA cream and/or 1% lidocaine injection for patients who do not tolerate the pain of cryotherapy.
Cryotherapy is effective and safe for both mother and fetus when applied in the second and third trimesters of pregnancy. An intermittent spray technique, using a small spray tip, is used to achieve a small region of cryonecrosis, limiting the runoff and scattering of liquid nitrogen. Cervical involvement that requires cervical cryotherapy does not increase the risk to mother or fetus.
Surgical Removal and Electrosurgery.
Excision with scissors, curettage, or electrosurgery produces immediate results. These methods are useful for both extensive condylomata and a limited number of warts. Small isolated warts on the shaft of the penis are best treated with conservative electrosurgery or scissor excision rather than subjecting the patient to repeated sessions with podophyllin. Large, unresponsive masses of warts around the rectum or vulva may be treated by scissor excision of the bulk of the mass, followed by electrocautery of the remaining tissue down to the skin surface. Removal of a very large mass of warts is a painful procedure and is best performed with the patient receiving a general or spinal anesthetic in the operating room. There is an increased risk for iatrogenic HPV infection with electrocautery and laser. The procedure should be performed in a room with adequate ventilation, providers should protect themselves with a mask, goggles and a gown, and the high flow suction should remove the plume.
Trichloroacetic Acid.
Application of trichloroacetic acid (TCA) 50% to 90% is effective and less destructive than laser surgery, electrocauterization, or liquid nitrogen application. It is most effective on small, moist warts.
This is an ideal treatment for isolated lesions in pregnant women. A very small amount is applied to the wart, which whitens immediately. The acid is then neutralized with water or bicarbonate of soda. The tissue slough heals in 7 to 10 days. Repeat each week or every other week as needed. Excessive application causes scars. Take great care not to treat normal surrounding skin.
Podophyllum Resin.
Podophyllin is a plant compound that causes cells to arrest in mitosis, leading to tissue necrosis. Podophyllum resin 10% to 25% in compound tincture of benzoin used to be the standard provider-administered therapy. It is prepared by a compounding pharmacist. Patient-applied medications are now commonly used. The medication can be very effective, especially for moist warts with a large surface area and lesions with many surface projections. Podophyllin is relatively ineffective in dry areas, such as the scrotum, penile shaft, and labia majora. It is not recommended for cervical, vaginal, or intraurethral warts. The compound is applied with a cotton-tipped applicator ( Fig. 11.22 ). The entire surface of the wart is covered with the solution, and the patient remains still until the solution dries in approximately 2 minutes. When lesions covered by the prepuce are treated, the applied solution must be allowed to dry for several minutes before the prepuce is returned to its usual position. Powdering the warts after treatment or applying petrolatum to the surrounding skin may help to avoid contamination of normal skin with the irritating resin. The medicine is removed by washing 1 hour later. The patient is treated again in 1 week. The podophyllin may then remain on the wart for 8 to 12 hours if there was little or no inflammation after the first treatment.

Overenthusiastic initial treatment can result in intense inflammation and discomfort that lasts for days. The procedure is simple and it is tempting to allow home treatment, but in most cases this should be avoided. Very frequently patients overtreat and cause excessive inflammation by applying podophyllin on normal skin. To avoid extreme discomfort, treat only part of a large warty mass in the perineal and rectal area. Warts on the shaft of the penis do not respond as successfully to podophyllin as do warts on the glans or under the foreskin; consequently, electrosurgery or cryosurgery should be used if two or three treatment sessions with podophyllin fail. Many warts disappear after a single treatment. Alternate forms of therapy should be attempted if there is no improvement after five treatment sessions.
Warning.
Systemic toxicity occurs from absorption of podophyllin. Paresthesia, polyneuritis, paralytic ileus, leukopenia, thrombocytopenia, coma, and death have occurred when large quantities of podophyllin were applied to wide areas or allowed to remain in contact with the skin for an extended period. Only limited areas should be treated during each session. Very small quantities should be used in the mouth, vaginal tract, or rectosigmoid area. Do not use podophyllin on pregnant women.
Alteration of Histopathology.
Podophyllin can produce bizarre forms of squamous cells, which can be mistaken for SCC. The pathologist must be informed of the patient’s exposure to podophyllin when a biopsy of a previously treated wart is submitted.
5-Fluorouracil Cream.
Application of a 5-fluorouracil cream may be considered in cases of genital warts that are resistant to all other treatments. A thin layer of cream is applied one to three times per week and washed off after 3 to 10 hours, depending on the sensitivity of the location. Treat for several weeks, as necessary. Irritation makes it intolerable for some patients.
Carbon Dioxide Laser.
The CO 2 laser is an ideal method for treating both primary and recurrent condylomata acuminata in men and women because of its precision and the wound’s rapid healing without scarring. The laser can be used with an operating microscope to find and destroy the smallest warts. For pregnant women, this is the treatment of choice for large or extensive lesions and for cases that do not respond to repeated applications of TCA (see provider precautions above).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


