The cleft-lip nasal deformity presents a formidable challenge in rhinoplasty surgery. A wide variety of techniques have been proposed for the correction of this problem, which is proof of the difficulty of this reconstructive problem. The approach outlined in this article amalgamates many cleft-lip rhinoplasty concepts into a single unified technique. This technique is designed to address the deficiencies present on the cleft side of the nose.
The cleft-lip nasal deformity presents a formidable challenge in rhinoplasty. The 3 main factors contributing to this deformity are congenital anatomic deficiency or aberrancy, surgical scarring from previous reconstructive attempts, and changes related to growth.
Various techniques have been proposed for the correction of this problem. The sheer number of methods described in the literature serves as a testament to the intrinsically difficult nature of this deformity. All these techniques attempt to address some aspect of the problem. However, complete correction of all nasal deficiencies remains an elusive goal for many.
Unilateral cleft nasal deformity
The unilateral deformity results from tissue deficiency of the cleft lip, deficiency in the bony premaxilla, and abnormal muscle pull on the nasal structures. The unilateral secondary nasal deformity may comprise most, if not all, of the following features:
- 1.
The dome on the cleft side is retrodisplaced and less well-projected.
- 2.
The columella on the cleft side is foreshortened.
- 3.
The medial crus slumps laterally.
- 4.
The lower lateral cartilage (LLC) and the alar rim form a caudal hood.
- 5.
There is an alar-columellar web.
- 6.
There is insufficient vestibular skin in the region of the vestibular dome.
- 7.
The nostril orientation can vary due to lateralized alar-base position and deficient nasal floor.
- 8.
The alar-base displacement (lateral, inferior, and posterior) is universally present in the primary cleft deformity. This can be affected by primary lip repair, primary cleft rhinoplasty, and alveolar bone grafting.
- 9.
The caudal septum is deflected into the noncleft side, but the severity of the deflection is variable.
Primary Unilateral Cleft Rhinoplasty
Primary nasal repair at the time of primary cleft-lip repair can help improve the cleft-lip nasal deformity by achieving better symmetry and improved overall long-term appearance of the nose. The primary lip repair is typically performed by the time the patient is 3 months old. All efforts are made to minimize nasal tissue trauma and scarring, which may unfavorably affect subsequent growth. In this regard, an effective method for primary unilateral cleft rhinoplasty involves unilateral LLC suspension via limited dissection.
Adequate correction from the primary procedure may lessen or eliminate the need for secondary cleft rhinoplasty.
Secondary Unilateral Cleft Rhinoplasty
Secondary nasal surgery includes intermediate and definitive rhinoplasty. Intermediate rhinoplasty is performed before nasal growth is completed and is based on 2 separate timing strategies. Rhinoplasty is done between the ages of 4 and 6 years, sometimes concomitantly with lip revision, to minimize any peer psychological pressure. Waiting until 8 to 12 years of age and until after the completion of orthodontic alignment and alveolar bone grafting allows a better skeletal base for correction of severe nasal deformities. In general, the intermediate rhinoplasty techniques are more conservative than those of definitive rhinoplasty.
Definitive rhinoplasty is performed when maxillary and nasal growths are complete. This usually occurs between 16 and 18 years of age. Rhinoplasty performed in this time frame allows for more aggressive septoplasty, osteotomies, and cartilage grafting maneuvers. Each patient requires an individualized approach to timing of secondary rhinoplasty, based on the severity of soft tissue and skeletal deformities.
The author’s preferred technique for secondary rhinoplasty is the sliding cheilorhinoplasty. This technique is designed to address the deficiencies present on the cleft side of the nose, including lowered dome height, LLC malposition, lateralized alar base, alar-columellar web, and vestibular lining deficit. This is accomplished using a laterally based chondrocutaneous flap of LLC, vestibular skin, and lip scar tissue, which is advanced superiorly and laterally. This procedure is usually performed through an external rhinoplasty approach with structural cartilage grafting to maintain nasal tip support and contour.
Technique
The sliding cheilorhinoplasty technique uses the existing upper lip scar as part of the advancement flap for increasing the vestibular internal lining. The vermilion is marked with methylene-blue tattoo marks ( Fig. 1 ).
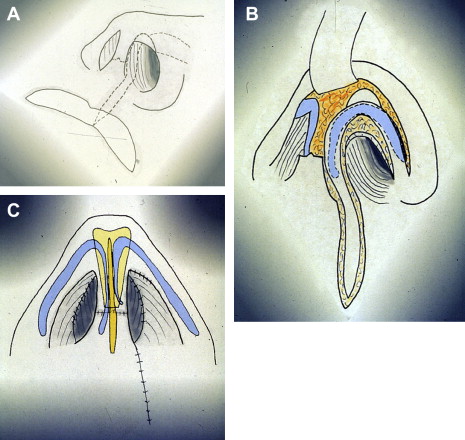
Two parallel incisions are then marked, which center on and encompass the unilateral upper lip scar that is to be revised. The width of this flap depends on the width of the original scar but should be at least 5 mm. The length of this flap is dictated by the amount of the lip scar that needs to be revised. The markings of these 2 parallel incisions are then extended into the nose. At the columella, the medial incision becomes continuous with the marginal incision. This incision is extended superiorly to encompass any alar webbing and is marked to create a rim margin that is symmetric to the contralateral normal rim. This incision is then merged with the continuation of the marginal incision laterally.
The lateral lip incision transitions into an intercartilaginous incision intranasally, and is carried superiorly and then laterally, outlining the entirety of the LLC. The lateral attachment of the flap is maintained to preserve flap vascularity.
Local anesthetic solution is infiltrated for hemostasis. The amount that is least necessary for vasoconstriction should be used to minimize tissue distortion.
Starting from the lip incision, the flap is elevated and extended superiorly and laterally, encompassing the lip scar and the LLC. Again, the lateral attachment of the flap is maintained for flap vascularity. The remainder of the nasal dorsum and the contralateral LLC is then exposed via the standard external rhinoplasty approach.
Any septal work may be accomplished at this time, including septoplasty and harvesting of grafting material. Care should be taken to leave sufficient dorsal caudal support for the nose.
A columellar pocket is next created. A columellar strut, which is used to anchor the cleft side LLC to the contralateral normal LLC, may be carved from either the septal or auricular cartilage. Symmetry of vestibular dome height is crucial in the positioning of the LLC. This symmetry typically requires advancement of the medial crus of the cleft LLC superiorly to match the vestibular dome heights bilaterally. This superior flap advancement in turn uses the residual lip scar as an internal nasal vestibular lining. Once the appropriate vestibular dome position has been established, the medial crura of the LLCs are secured to the strut with horizontal mattress sutures.
The upper lip is then repaired with tension-bearing sutures placed within the orbicularis musculature.
Once the base of the nose has been stabilized, attention is directed toward the nasal tip. Cephalic trim of the LLC may be performed as indicated. A shield-type tip cartilage graft can be sutured into position to maintain tip projection and to augment tip support. This graft also has the added advantage of allowing camouflage of minor tip asymmetries.
Closure of all incisions is then performed. Slight infolding of the alar-columellar web tissue on reapproximation of the marginal incision improves alar margin symmetry. The routine intranasal and external dressings and splint are then applied.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


