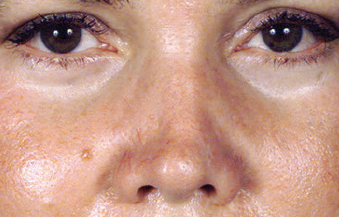
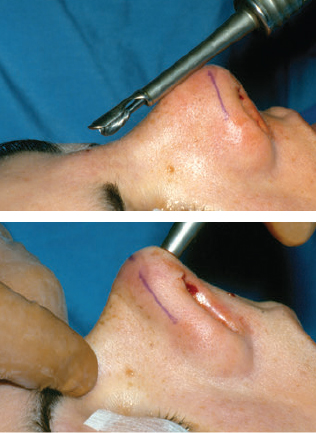
CHAPTER Secondary surgery may be performed for minor imperfections (revision rhinoplasty) or correction of major flaws, largely using primary rhinoplasty maneuvers. Some of the common flaws encountered in secondary rhinoplasty are listed in this chapter. Managing a patient who requires secondary rhinoplasty is vastly different from the management of a primary rhinoplasty patient in many aspects, presenting a technical challenge and requiring even greater precision in the planning and execution of surgical techniques. A surgeon’s interpersonal skills are also important in providing the patient with requisite emotional support throughout the process.1–5 The surgeon must have a clear understanding of the patient’s concerns, define the imperfections precisely, and identify corresponding solutions while setting realistic goals and expectations. Comprehensive knowledge of potential problems and pitfalls and finesse during surgery is crucial to achieving these goals. In this chapter, the main differences between primary and secondary rhinoplasty in terms of patient evaluation, surgical planning, technical details, and postoperative care are discussed. Secondary rhinoplasty patients have spent significant time analyzing the form and function of their nose. Many patients spend time researching revision rhinoplasty on the internet, often exploring medical literature in addition to navigating through the nonscientific sources of information before consultation. Often, they have also sought the opinions of other plastic surgeons, and as a result, patients pre sent with clear ideas and define the deformity using plastic surgery terminology. Some even have opinions regarding the techniques they wish used to fix the abnormalities. Summary Box Common Deformities Encountered in Secondary Rhinoplasty • Skin thickness issues • Radix depth imperfections • Nasal bone flaws • Tip disharmonies • Nostril imbalance • Nasolabial angle abnormalities • Alar rim retraction • Airway issues Listening to patients while they explain their dissatisfaction and noting the manner in which these concerns are expressed may provide valuable insight regarding their level of perfectionism and nature of their expectations. This will help the surgeon better determine whether the patient would be likely to be pleased with the surgical outcome. For example, if a patient avers that his or her previous surgeon “butchered the nose,” but the examination reveals only some minor flaws, it is very unlikely that the patient will be pleased with the results of any secondary surgery. Conversely, a patient whose nose has major flaws but who makes mitigating remarks about the previous surgery has the highest probability of being satisfied with the outcomes of a subsequent procedure. Many patients seeking primary rhinoplasty are not aware of their breathing problems, and thus they do not volunteer any information regarding breathing concerns or may even deny having airway concerns. Careful observation may reveal that many of these patients are mouth breathers, and internal examination may reveal airway obstruction. The main reason for this unawareness or denial is that they have grown up with this problem and lack a base for comparison. Conversely, secondary rhinoplasty patients are aware of their breathing difficulties and commonly associate it with previous surgery. These patients have a clear base for comparison, and if their airway is adversely affected for different reasons, they can sense it. Common conditions leading to airway problems are alteration in internal or external valves, scar tissue formation, medialization of inferior turbinates and upper lateral cartilages or, often, a combination of these adverse changes.6–8 Secondary rhinoplasty patients have a great deal of apprehension before the upcoming surgery compared with primary surgery patients. They also exhibit more frustration and impatience. They may have a more negative attitude toward the surgical team because of their perceived undesirable experience with primary surgery. Thus restoring their trust may pose a challenge. To overcome these adversities, the surgeon must demonstrate more compassion and restore confidence by identifying and describing the disharmonies and providing a thorough explanation regarding how to correct the flaws. A longer consultation time is needed for secondary rhinoplasty patients compared with primary surgery patients, because some of them spend a significant portion of their visit trying to explore what went wrong during the initial surgery. It is crucial to redirect the patient’s focus to the current problems and avoid any negative statements about the previous surgery and the surgeon. Any unfounded adverse statements made by the second surgeon may evoke or intensify the patient’s rage toward the primary team. When appropriate, potential legal actions can be averted by explaining how complicated rhinoplasties can be and how rare it is to attain perfect outcomes under most circumstances. Voicing a negative opinion or making any disapproving statements about the primary surgery and the surgeon solely based on the patient’s emotional statements is utterly unfair and inappropriate. It is important to be especially cognizant of the potential effects of nonverbal cues while listening to the patient. Any intentional or unintentional facial expressions, eye rolling, grimacing, or gesture of disdain should be prevented. This unethical, unprofessional conduct may further escalate a patient’s negative emotions toward his or her primary surgeon and place additional strain on the already disturbed relationship. Any professional judgments should either be deferred until all of the facts pertaining to the previous surgery have been scrutinized or be avoided altogether. Every attempt should be made to persuade the patient to return to the previous surgeon. This is a professional courtesy and often offers an economic advantage to the patient. However, the patient’s interest is the main priority. Therefore if the patient is reluctant to return to her previous surgeon and if the previous surgeon’s skills are unknown or questionable, a more experienced or seasoned surgeon should undertake the patient care. In doing so, operative notes from the previous surgery should be obtained and confirmed by physical examination. The magnitude of previous septal cartilage resection and turbinectomy must be assessed before surgery. A secondary rhinoplasty consult should also include an entire facial analysis, like the primary rhinoplasty, because other facial disharmonies like forehead prominence or retrusion, chin deformities, malar bone hypoplasia, or a dysmorphic maxilla or mandible may be contributing factors to the patient’s dissatisfaction.9,10 Any disharmony in these features, if detrimental to rhinoplasty outcomes, should be brought to the patient’s attention and documented. However, insistence on correcting these deformities before or at the time of rhinoplasty should be discouraged. It is crucial to ensure that the patient has realistic expectations and is not suffering from any underlying psychological conditions that would contribute to patient dissatisfaction regardless of the surgical outcome. A significantly disproportionate concern about the deformity is prodigiously alarming, and these patients require careful evaluation to rule out body dysmorphic disorder. Asking the patient to rate the nasal deformity on a scale of 1 to 10 (with 10 being a perfect nose) and comparing this to the number assigned by the surgeon can be enormously helpful in recognizing those patients who may not be pleased after the surgery, regardless of triumphant surgical results. Proceeding with another rhinoplasty when there is more than a 3- to 4- point disparity between the patient’s and the surgeon’s scores may not be advisable without further analysis. Observation of the skin thickness is the first important step in evaluating a patient for a rhinoplasty, because thick and sebaceous skin could be a reason for a failed primary rhinoplasty procedure, and these patients may not be optimal candidates for any external skin incision. For patients with sebaceous and thick skin, referral to a dermatologist may be appropriate to reduce sebaceous overactivity before secondary rhinoplasty. Tretinoin or isotretinoin are often used to treat this condition. However, surgery should be delayed for 6 months or more after this treatment has been completed to reduce treatment-induced hypertrophic scarring or increased bleeding. Achieving pleasing tip definition is often difficult in patients with thick skin. Appropriate measures should be incorporated into the surgery to attain better tip delineation in these patients. Any dead space, in particular, should be avoided, because it can be replaced with blood, followed by scar or fibrofatty tissue, all of which can adversely affect tip definition and result in a polly beak or supratip deformity. Patients presenting for a secondary rhinoplasty may have thin skin over the dorsum of the nose because of a subcutaneous dissection instead of subperiosteal dissection during the primary surgery. In these patients, some of the valuable soft tissue is eliminated while removing the dorsal hump. On patients with thin skin even the smallest dorsal irregularities are easily discernable. A layer of perichondrium, fascia, or dermis graft may be required to augment the soft tissue and overcome this deficiency. Dorsal augmentation with alloplastic material is another reason for thinning of the skin. These patients may have purplish discoloration of the skin directly over the implanted material, which is often more noticeable in cold weather. This discoloration can be improved by replacement of the implant with the autogenous materials and addition of soft tissue in the subcutaneous plane of the dorsum. Some secondary rhinoplasty patients have telangiectasia on the nasal skin, which may become more intense after surgery. These patients need to be informed of this matter and the fact that it might be necessary to treat this undesirable skin appearance with laser. Suboptimal scars from primary surgery might be a predictor of poor healing after secondary surgery. A systemic examination of the external nose from the radix to the subnasale is necessary to detect all of the imperfections. A shallow radix is a fairly common finding that results in an undesirable transition from the forehead to the dorsum of the nose (Fig. 24.1). The radix may be too shallow because of undercorrection or not correcting the abnormality during primary surgery. Overresection of the radix is uncommon, because inexperienced surgeons have difficulty deepening the radix. Nasal bone asymmetry or irregularity is one of the most common reasons for patient dissatisfaction (Fig. 24.2). In an optimal rhinoplasty outcome, there is a graceful transition of the shadows from the eyebrows to the tip of the nose. Dorsal aesthetic lines may be distorted or another line posterior to the excising line may be seen in patients with suboptimal rhinoplasty results. This extra dorsal line is usually a result of the lateral osteotomy being too anterior (Fig. 24.3). Upper lateral cartilages may also appear asymmetrical as a result of unilateral overresection or, more commonly, be caused by anterior deviation of the septum (Fig. 24.4). Overresection of the middle vault might cause an inverted-V deformity because of medial shift or collapse of the upper lateral cartilages (Fig. 24.5). Increased awareness of this problem and the use of spreader grafts has reduced the incidence of inverted-V deformities. This collapse is usually not seen intraoperatively or in the early postoperative period. Depending on skin thickness, the problem may reveal itself several months to several years after the surgery. Fig. 24.1 A patient with an underresected radix. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Fig. 24.2 A patient with an asymmetrical nasal bone after primary rhinoplasty. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Fig. 24.3 An anterior lateral osteotomy during initial surgery caused this step deformity. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Fig. 24.4 Deviation of the anterior septum resulting in the appearance of asymmetrical upper lateral cartilages. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Fig. 24.5 An inverted-V deformity. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Fig. 24.6 A supratip deformity. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) Tip deformities may range from minor imperfections, such as asymmetry of the domes, to gross disharmony and complete distortion.11 An underprojected tip is a common problem requiring secondary rhinoplasty. Disproportionate nasal tip width is also a common issue. A hanging or retracted tip is a common component of the imbalances necessitating secondary rhinoplasty. Disproportionate width of the alar base is also common and may be the reason for dissatisfaction. A supratip deformity (Fig. 24.6) may be caused by an underresected or overresected caudal dorsum, underprojected tip (pseudodeformity), or a combination of these factors.12 As stated previously, overresection of the caudal septum may result in a dead space, facilitating accumulation of blood and fluid and promoting scar formation and fibrosis, which ultimately create fullness in the supratip area. An obtuse nasolabial angle (overshortened nose) was the hallmark of rhinoplasties performed in 1970s and early 1980s, whereas suboptimal tip rotation is more common today. The latter is the consequence of an effort to be conservative and prevent an obtuse nasolabial angle. A hanging columella (Fig. 24.7) may result from the placement of the columella strut or protrusion of the caudal septum. Ideally, about 4 mm of columella is visible on the profile view. Excessive columellar show is displeasing and needs correction. In contrast, a retracted columella can result from overresection of the caudal septum or a short caudal septum. Rarely, this disharmony is the cause of a hanging ala, creating an ostensible retracted columella. Fig. 24.7 A hanging columella. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) On the basilar view, asymmetry of the domes, nostril shape, and infratip lobule volume and length would be evaluated. Excessive soft triangle lining and overall nasal tip and columella deviation can be assessed in this view as well. Nasal valves should be evaluated during deep breathing. Collapse of the internal nasal valves was very common in rhinoplasties done in 1980s because of aggressive resection of the middle vault. Although this is less common today, it is still seen occasionally. Intranasal examination to identify nasal septal deviation, septal perforation, enlarged turbinates, synechiae, and polyps is crucial in every rhinoplasty patient evaluation. Because of the level of precision required to correct the deformities seen in secondary rhinoplasty, patient assessment using digital life-sized photographs is even more important than in primary rhinoplasty.13 This tool also ensures synchronicity between the surgeon’s and the patient’s goals. Generally, secondary rhinoplasty should not be performed until at least 1 year has passed after the original surgery. However, in rare cases, the amount of deformity and anxiety of the patient may mandate earlier intervention. In these cases, scar tissue and swelling may sacrifice the final results; even with a perfect initial surgical outcome, subsidence of swelling that is hiding flaws may reveal the necessity for further revisions in the future. Multiple visits and discussions are advisable to ensure a clear mutual understanding between the surgeon and patient before the secondary surgery. This will also provide more time for healing before a revision surgery. Routine steps for informed consent should be taken by going over procedure-specific, general anesthetic, and surgical complications. Unpredictability and possible failure to reach the goal should be discussed with the patient and documented. Limitations resulting from the presence of scar tissue, finite supply of available and suitable cartilage grafts, shrinkage of the skin, and telangiectasis must be explained to the patient. The potential need for cartilage graft from costal or conchal sources should also be reviewed and the potential cartilage graft source and backup source determined before surgery based on the surgeon’s and patient’s preference. Other complications like airway problems and scarring should be reviewed. The ideal candidate for surgery is a patient with a clear understanding of the surgery and its limitations. A patient with unrealistic expectations or one who demands perfection, makes disparaging remarks about the previous surgeon, or makes the surgeon uncomfortable is not a good candidate for secondary rhinoplasty. Correction of nasal deformities resulting from a primary surgery might require minor, intermediate, or major rhinoplasty. Minor revision, such as placement of a tip or dorsal graft, can be done under local anesthesia with or without sedation. It is preferable that major surgeries are performed with general anesthesia for three reasons: 1. Scar tissue might make the diffusion of the local anesthetic more difficult and unpredictable. 2. Dissection of the nose and septum often is very difficult because scar tissue requires more intense surgeon concentration and patient relaxation. 3. Airway protection and blood aspiration are better controlled with endotracheal anesthesia than with deep sedation. A minor revision can be achieved with an endonasal incision for the placement of tip or dorsal grafts. However, for a major revision, a columellar stair-step incision or a V incision is preferred.14,15 An open approach provides a better view of the deformity and offers an opportunity for analyzing the reasons for the failed previous surgery and more successful correction. If the original surgery was performed with an open technique, another open incision is safer because of the “delayed” phenomenon. Regardless, an open technique can be used even if the original surgery was performed with a closed technique. The key to a successful surgery is the ability to identify the imperfections and facilitate adequate exposure, regardless of the surgical technique used. Most deformities can be readily detected during external examination. However, it is not always possible to fully delineate structural flaws, especially in the tip area, during physical examination; thus the surgeon might experience some unexpected findings during surgery and must be prepared to manage them. After induction of anesthesia, the nose is packed with gauze saturated in 4% cocaine or phenylephrine. Lidocaine containing 1:200,000 epinephrine is infiltrated in an organized manner circumferentially, and if a turbinectomy is planned as part of the procedure, the turbinates are injected before nasal injection. After allowing a few minutes for the initial vasoconstriction, a second injection is administered with a mixture of lidocaine and ropivacaine including 1:100,000 epinephrine for additional vasoconstriction. Vasoconstriction after the first injection will minimize the systemic effects of the secondary injection and produce more protracted anesthesia and more comfortable recovery. A step or inverted-V incision is made in the columella, and meticulous dissection is carried to the nasal tip and dorsum, separating soft tissue from the nasal frame. A guarded burr can be used to remove additional bone from an undercorrected or shallow radix.16 This tool is safe and very effective if used properly. After adequate dissection of the soft tissue in the dorsum and radix, the guarded burr is introduced into the radix area (Fig. 24.8). After activation of the device, the radix is lowered using a side-to-side motion of the device for short duration to avoid thermal damage. If the dorsal hump is large, it can be removed first to facilitate the insertion of the device between the skin pocket and radix bone. Occasional soft tissue interference with the movement of the burr should not discourage its use. Repeated, judicious use of this tool will achieve its intended results. However, caution should be exercised because this tool is very powerful and may cause excessive bone removal if used too aggressively. Fig. 24.8 Guarded burr for reduction of a bony radix. (Reproduced from Totonchi A and Guyron B. Common secondary nose flaws and their logical correction. In: Rohrich RJ, Ahmad J, eds. Secondary Rhinoplasty by the Global Masters. St. Louis: CRC Press; 2016.) A rasp can be used to remove the residual dorsal hump. It is crucial to dissect the soft tissue completely off the bone before using the rasp to prevent thinning of soft tissue, as mentioned previously. Rasping of the bone might create a wide appearance to the dorsum, or even an open roof deformity, which would require a corrective osteotomy. If septoplasty is indicated, it should be done at this time using a dorsal open technique. If the area is devoid of a dorsal hump to be removed or the dorsal hump removal does not create an open roof, septoplasty can be done using an L-shaped mucoperichondrial incision. Although some authors recommend the removal of dorsal humps using an osteotome, this is not usually advisable on secondary rhinoplasty patients, because the remaining dorsal hump is irregular. Lateral low-to-low osteotomies can be performed percutaneously or through a small incision in the vestibular lining. If the latter is selected, subperiosteal dissection may not be as easy as in the primary rhinoplasty because of the extent of the adhesions. On the other hand, secondary osteotomy is often easier if it is performed at the same site as primary osteotomy, because bone deposition at the osteotomy site is never as strong as the original bone. The secondary osteotomy is sometimes done further posteriorly, because the osteotomies leading to the secondary procedures are performed too anterior and require correction by another more posteriorly placed osteotomy. This is done mainly to make the lateral wall smoother. In patients who have a wide bony dorsum or who have very thick bone in this area, which may prevent the medialization of the nasal bone, a double medial osteotomy will be necessary to remove a bony wedge. The first osteotomy is on the medial aspect of the nasal bone, slightly lateral to the midline, aiming superiorly and medial. The second is immediately lateral to the septum, aiming laterally and superiorly. These two osteotomies are joined at the nasion, and then the bony wedge is removed. After completing the low-to-low and medial osteotomies, a percutaneous anteroposterior osteotomy at the nasion area (at the location of nasal divergence) is performed to reposition the nasal bone as a unit. A small lateral depression over the nasal bone can be camouflaged using a cartilage graft, or even a fat graft, as long as the airway has not been significantly narrowed by the medial displacement of the nasal bone and the upper lateral cartilage and the internal valve remains competent. If the patient experiences difficulty breathing, it may be necessary to correct the nasal valve by outfracturing the nasal bones and placing spreader grafts, which will reposition the upper lateral cartilages and improve the airway. A cartilage graft can be used to correct the deficiencies on the dorsum of the nose caused by overresection or asymmetrical resection of the hump. The septal cartilage is an optimal source of cartilage for dorsal augmentation. A history of septoplasty should not necessarily change the plan by either precluding the exploration or use of the septum. If available, the septal cartilage is prepared and gently crushed and the margins are beveled to prevent harsh dorsal lines or step-off (Fig. 24.9). Adequate soft tissue dissection is necessary to avoid forcing and subsequently fracturing or malpositioning the graft. After proper positioning, the cartilage is secured to the dorsum to prevent shifting using 5–0 PDS sutures. The conchal cartilage is a second choice only for minor deformities. For major deficiencies, a costochondral graft is a better choice. To harvest a conchal cartilage graft, the ear is infiltrated on its medial and lateral surfaces with lidocaine containing 1:100,000 epinephrine, using a 27-gauge needle. The site of the cartilage incision is marked from the anterior surface using a 25-gauge needle dipped in methylene blue. An incision is made on the posterior surface of the ear. The dissection is carried toward the cartilage, leaving the perichondrium on the medial surface of the cartilage graft. The lateral surface is dissected in the subperichondrial plane and the cartilage is incised, guided by the methylene blue marks. The wound is irrigated and a 5–0 plain catgut suture is passed through the upper portion of the conchal fossa on the lateral side, taken through the mastoid fascia and brought out through the lower part of the fossa and clamped, leaving a sufficient loop. Then the posterior skin is closed using a 5–0 running locking catgut. At the end, a cotton ball is moistened and placed in the conchal fossa and the 5–0 catgut loop is closed over it to secure the cotton ball in place and to eliminate the dead space.
24
Secondary Rhinoplasty
Avoiding Unfavorable Results and Complications in Secondary Rhinoplasty
Patient Evaluation
Physical Examinations and Common Flaws






Preoperative Planning
Surgical Technique
Incision
Alteration of the Radix
Removing the Residual Dorsal Hump
Nasal Bone Osteotomy
Correcting the Dorsal Deficiency
Harvesting a Conchal Cartilage Graft
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine










