Secondary Correction of Enophthalmos
David Matthews
Samer Abouzeid
Edward W. Kubek
DEFINITION
Enophthalmos refers to the posterior position of one eye relative to the contralateral eye.1
Secondary post-traumatic enophthalmos refers to the persistence of enophthalmos after attempted correction during the primary operation and is a common sequela to orbital trauma.
Hypoglobus describes a vertical discrepancy in globe position.
Secondary post-traumatic enophthalmos is the most common secondary facial deformity following primary surgery for facial trauma.2
Until the 1970s, enophthalmos was not considered correctable.
Tessier’s work demonstrated that both acute and late enophthalmos were correctable.
In 1982, Kawamoto first reported his technique to correct long-standing post-traumatic enophthalmos with osteotomies and bone grafting.3
These techniques were then repeated by Manson, Wolfe, and Gruss.4
ANATOMY
The bony architecture of the orbit forms two basic components, the orbital frame (comprising the rim) and the orbital pyramid with its apex pointed posteriorly (comprising the floor, roof, lateral wall, and medial orbital wall.
The optic nerve enters the orbit at the apex of an asymmetric pyramid where the apex is oriented posteromedially and superiorly.
General dimensions of the bony orbit are 50 mm deep, 35 mm wide, and 40 mm high.1
Each of the pyramid’s four walls has a unique shape that contributes to globe position.1
Four structures of surgical importance1:
The Hammer’s “key area,” or posterior part of the medial orbital wall (FIG 1).
S-Curvature of the posterior one-third of the orbital floor—any graft, synthetic or autologous, must sit atop the ledge created by the palatine bone posteriorly.
Greater wing of the sphenoid—anatomic reduction indicates proper alignment of the lateral wall and rim with the zygoma.
Orbital rim position—failure to anatomically reduce a displaced orbital rim (ie, the frame) prevents restoration of normal orbital shape and volume.
Four measurements of surgical importance denote safe distances of dissection beyond key structures. Note that dissecting posteriorly to these distances will still be insufficient for secondary correction of enophthalmos, if the posterior margin of the defect is not defined.
Dissection should be limited to:
Medial wall—36 mm of the anterior lacrimal crest
Orbital floor—35 mm of the infraorbital foramen
Orbital roof—30 mm of the supraorbital notch
Lateral wall—25 mm of the frontozygomatic suture
PATHOGENESIS (OPTIONAL)
Post-traumatic, secondary enophthalmos occurs when the fracture pattern expands the volume of the bony orbit and is either uncorrected (FIG 2A) or reduced in the wrong position (FIG 2B):
As a result, the globe occupies a smaller percentage of the total space and assumes a more posterior position.
The most common cause of secondary enophthalmos during the primary operation is inadequate posterior dissection for fear of injuring the optic nerve or globe,2 followed by inadequate reduction of medial wall fractures (FIG 3).5
Failure to re-establish the anatomic form of Hammer’s key area and/or the S-curve of the posterior orbital floor can also lead to secondary enophthalmos, even in cases where the orbital floor is intact.1
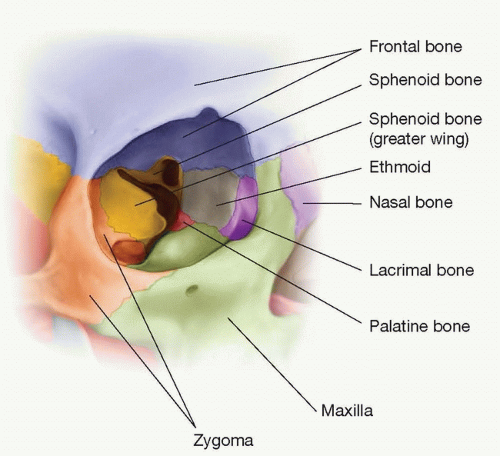
FIG 1 • Key areas of the orbit include the junction between the zygomatic bone and greater wing of the sphenoid. The palatine bone should be used as a support shelf for the bone graft.
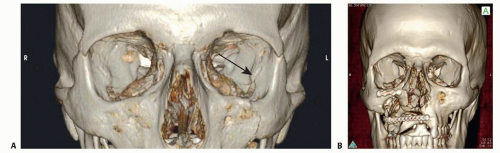
FIG 2 • A. Absent reduction of the orbital floor (see black arrow) results in increased orbital volume leading to enophthalmos. B. Inadequate reduction after remote zygoma fracture demonstrates the ledge between the zygomatic bone and the greater wing of the sphenoid.
Late atrophy of orbital fat is rarely demonstrated and is not a cause of secondary enophthalmos5; furthermore, it should be the goal of the surgeon to reduce all malpositioned orbital fat noted during the workup for secondary correction.
NATURAL HISTORY
In the early postinjury period, clinical enophthalmos is usually masked by swelling.
As edema subsides, postsurgical patients, or those who did not seek acute care, may present with enophthalmos, in the presence or absence of diplopia.
Globe position and healing after the primary operation or injury is considered stable at 6 months.2
PATIENT HISTORY AND PHYSICAL FINDINGS
Normal physiologic anteroposterior variance between eyes is ≤2 mm.1Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree