Key Term
Two feet–one hand syndrome
Scaly disorders are a heterogeneous presentation of skin diseases that primarily manifest with scale. This group includes inherited disorders (e.g., ichthyosis vulgaris), acquired disorders (e.g., xerosis), and infections (e.g., tinea pedis).
Important History Questions
How long has the lesion(s) been present?
This is an important question to distinguish between a genodermatosis, such as ichthyosis vulgaris, from an acquired disorder, such as xerosis.
Have you had a similar lesion(s) in the past?
Some disorders, such as tinea pedis, tend to be one-time events, whereas tinea versicolor and xerosis are often characterized by episodic disease.
Do any of your immediate relatives have a similar disorder?
A “yes” answer indicates a possible genodermatosis; however, the answer has to be weighed against the possibility that the disorder is acquired as an infection from an immediate family member. For example, it is not uncommon for multiple family members to have tinea versicolor or tinea pedis.
How are you treating your skin condition?
Many patients use home-based, over-the-counter (OTC), or prescription remedies that can alter the appearance of the condition. Some home remedies may actually make the condition worse.
Has the skin condition ever been biopsied?
This of course could be helpful in regard to any of the conditions in this chapter; however, not all of the disorders have specific histologic findings. If there is a history of previous biopsies, consider having the biopsy reviewed by a dermatopathologist or a pathologist with expertise in this area because subtle clues to the diagnosis may be missed in scaly disorders.
Are you taking any medications?
This is an important question because some disorders, such as palmoplantar keratodermas, xerosis, and ichthyoses, may be produced by medications.
Important Physical Findings
What is the distribution of the lesions?
Some of the cutaneous disorders demonstrate a characteristic location. For example, ichthyosis vulgaris involves the extensor surfaces of the extremities and spares the intertriginous areas. Tinea pedis and palmoplantar keratodermas are most commonly restricted to palmoplantar areas. Tinea versicolor tends to affect the trunk and usually but not always spares the face.
Are the nails normal or abnormal?
Nail findings may suggest a diagnosis. For example, in tinea pedis there is often accompanying fungal nail disease, whereas in palmoplantar keratodermas, the nails are often unaffected.
What is the color of the scale?
The majority of the scaly disorders demonstrate white scale; however, there are important exceptions, notably tinea versicolor, which has a fine brownish scale, and ichthyosis vulgaris, which has a yellowish-brown scale. Thickened keratin on the palms and soles may have a yellow-brown hue, which may be a clue to an inherited palmoplantar keratoderma.
What are the size and shape of the scale?
Not all scale has the same appearance. For example, tinea versicolor has a fine branlike scale, whereas ichthyosis vulgaris often has a larger rhomboidal scale. Xerosis demonstrates small white scale, which may crack.
Tinea (Pityriasis) Versicolor
ICD10 code B36.0
SUPERFICIAL FUNGAL INFECTION
Pathogenesis
Tinea versicolor is a common superficial fungal infection produced by the yeast Malassezia furfur and other species in this genus. This yeast is a normal part of the cutaneous microflora; however, under certain conditions, it will convert to the mixed hyphal and yeast form, which produces clinical disease. Malassezia spp. require lipids for growth and are not dermatophytes. Tinea versicolor is more common in warm humid climates, where it may affect up to 50% of adults.
Clinical Features
- •
It typically affects adolescents and young adults.
- •
Tinea versicolor is usually asymptomatic, although occasional patients may complain of a burning sensation or mild pruritus.
- •
Primary lesions are tan or fawn-colored macules that may coalesce into large patches ( Figs. 9.1 and 9.2 ).

Fig. 9.1
Patient with sharply defined, asymptomatic, fawn-colored patches on the trunk. Note involvement of the navel, an area that is frequently affected.

Fig. 9.2
Patient with large confluent plaques of tinea versicolor presenting on the trunk. Once again, note involvement of the naval area.
- •
Close inspection reveals a fine branlike scale that covers the entire macule or patch.
- •
The affected areas usually display a truncal distribution, although extension to acral areas may occur.
- •
Hypopigmented macules ( Fig. 9.3 ), due to the production of biochemical products by the yeast that interfere with melanin synthesis and packaging, is a less common presentation. This decrease in pigmentation is more noticeable when the patient has darker skin or is well tanned.

Fig. 9.3
Patient with hypopigmented tinea versicolor presenting as sharply hypopigmented plaques with fine scale on a patient with a darker skin type.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
Diagnosis
- •
A clinical presentation of a predominantly truncal eruption with fine scale that is fawn-colored or hypopigmented is usually diagnostic.
- •
A potassium hydroxide (KOH) examination can be done by scraping or using clear tape. The finding of an admixture of yeast and short hyphae (so-called spaghetti and meatballs) is diagnostic ( Figs. 2.8 and 9.4 ).
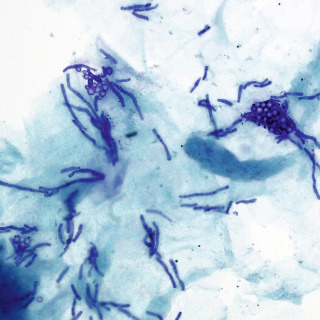
Fig. 9.4
Tape preparation of a sample stained with methylene blue demonstrating diagnostic short hyphae and clusters of yeast (400×).
- •
Rare or atypical cases may require a shave or punch biopsy. The yeast and short hyphae can be seen in the stratum corneum on routine H&E stain; however, special stains make it easier for the pathologist or dermatopathologist to identify the organisms.
- •
Culture can be done on scrapings but is not recommended because most laboratories have little or no experience preparing special lipid-augmented (usually olive oil) media.
Treatment
- •
Limited tinea versicolor is best and most easily treated with any of the topical imidazole antifungal creams, including bifonazole, clotrimazole, econazole, ketoconazole, oxiconazole, and tioconazole. There are no differences in efficacy among these agents; price and availability are the driving factors behind the choice. These are typically applied twice per day for 2 to 4 weeks.
- •
Larger areas of tinea versicolor are better treated with liquid preparations, such as flutrimazole shampoo and ketoconazole shampoo; these are typically applied for 5 minutes before rinsing. Treatment typically lasts 2 to 4 weeks. Topical 2.5% selenium sulfide can also be used in a similar fashion; however, it can be a significant irritant and is not preferred.
- •
Itraconazole, 200 mg/day for 7 days, or a single dose of 400 mg, has been used effectively and has an expected cure rate of over 80%. Another oral alternative is fluconazole, which is generally used in a dose of 300 mg once weekly for 2 weeks.
Clinical Course
In humid climates, in patients prone to tinea versicolor, the recurrence rate is almost 50% at 6 months after therapy. In one double-blind, placebo-controlled study, itraconazole prophylaxis, using a regimen of 200 mg taken orally each month for 6 months, reduced the relapse rate to 12%.
Acquired Ichthyosis Vulgaris (Ichthyosis Acquisita)
ICD10 code L85.0
ACQUIRED DISORDER OF KERATINIZATION
- •
Acitretin
- •
Cholesterol-lowering drugs (e.g., pravastatin)
- •
Clofazimine
- •
Hydroxyurea
- •
Kava
- •
Lithium
- •
Nicotinic acid
Pathogenesis
Acquired ichthyosis is associated with a number of underlying conditions, including malignancies (particularly Hodgkin lymphoma), sarcoidosis, graft-versus-host disease, lupus erythematosus, and some medications (see box). This disorder of keratinization usually parallels the course of the underlying disease process. In some cases, the ichthyosiform changes are the presenting complaint.
Clinical Features
- •
As the name implies, acquired ichthyosis is not present at birth; most cases occur in adults, including the elderly.
- •
In contrast to ichthyosis vulgaris, acquired ichthyosis is not associated with atopic dermatitis, and increased palmar and plantar skin markings are usually not present.
- •
The primary lesion is a bran-like, fine, lightly scaling lesion in areas other than the extensor limbs; lesions typically spare the flexures and face.
- •
The legs and arms typically demonstrate larger brownish or brownish-yellow rhomboidal scales, which may demonstrate a subtle tendency to turn out at the edges ( Figs. 9.5 and 9.6 ).

Fig. 9.5
Acquired ichthyosis vulgaris. This patient had sarcoidosis and large, brownish, rhomboidal scale on the anterior legs, indistinguishable from the genetic form of ichthyosis vulgaris. In some cases, a biopsy taken from this area will demonstrate underlying sarcoidal granulomas.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








