Key Words
layers of the “scalp”, parietal laxity, galeal scoring, wide undermining, rotation-advancement flap, skin grafting, latissimus dorsi free flap
Synopsis
Scalp defects arise from a variety of etiologies and often have complex presentations. The reconstructive process begins with a thorough defect analysis, including size, location, wound conditions, and possible exposure of underlying structures. Reconstructive options follow the tenets of the reconstructive elevator, though the hair-bearing nature and inelasticity of the galea pose unique challenges for scalp reconstruction. Small defects may be amenable to primary closure or healing by secondary intention. Skin grafting may be an appropriate option for patients who cannot tolerate a more involved procedure, or may be used for coverage of a secondary defect. In less acute settings, tissue expansion may be used to generate additional hair-bearing skin for wound coverage or scalp resurfacing. Larger defects often require local flaps, commonly rotation flaps that recruit tissue from the surrounding regions. For the largest, most complex defects, the latissimus dorsi flap should be considered, because it is the workhorse free flap for reconstruction of extensive scalp wounds. In general, complications of scalp reconstruction include wound breakdown, infection, implant exposure, and graft or flap failure, which may be minimized with close post-operative monitoring and timely management.
Clinical Problem
Presentation and Etiologies
The clinical presentation of scalp defects is broad and varies by causative factor. Etiologies may be congenital or acquired, both of which have been previously enumerated in the literature. Congenital etiologies include aplasia cutis; congenital nevi, vascular malformations, and congenital tumors. Acquired etiologies broadly involve traumatic, oncologic, and infectious causes. Traumatic injuries may be blunt or penetrating, or the result of avulsion or burns. Oncologic defects may be secondary to tumor invasion, resection, and/or therapeutic radiation. Wound healing problems and scarring may also lead to scalp defects.
Associated Conditions
Patients with scalp defects may similarly present with a spectrum of associated conditions. Deformity or absence of a segment of calvarium may accompany soft tissue defects. In these patients, it is critical to consider the necessity and timing of calvarial reconstruction. Scalp soft tissue wounds may demonstrate active infection with or without osteomyelitis of the underlying calvarium, the latter of which is particularly at risk in instances of chronic infection or exposure. Tumors involving the scalp pose several challenges due to a potential need for wide resection, pre- and/or post-operative chemotherapy and radiation, and timely reconstruction to avoid delays with cancer therapy. Margin status is a major consideration in patients for whom resection is intended to be curative, and must be verified as clear before final reconstruction. Cancer patients may also have shortened life expectancy and poor nutrition status that predisposes to impaired wound healing, both of which should factor into reconstructive decision making.
Pre-Operative Management
Physical Examination
In performing the pre-operative history and physical examination, it is necessary to assess the general health of the patient with special attention to medical factors that may affect ability to undergo anesthesia and/or wound healing. Such medical issues include cardiopulmonary health, peripheral vascular disease, diabetes mellitus, immunosuppression, and history of smoking or radiation. Goals of surgery should also be clarified, including cure versus palliation in cases of malignancy, and wound closure versus aesthetics. The physical examination must include a detailed defect analysis, including the location, depth, and size of the anticipated defect; exposure of underlying structures such as bone, prosthetic material, or dura; and the health of the surrounding tissues, which may show evidence of prior radiation, burns, or scar.
Key Anatomy
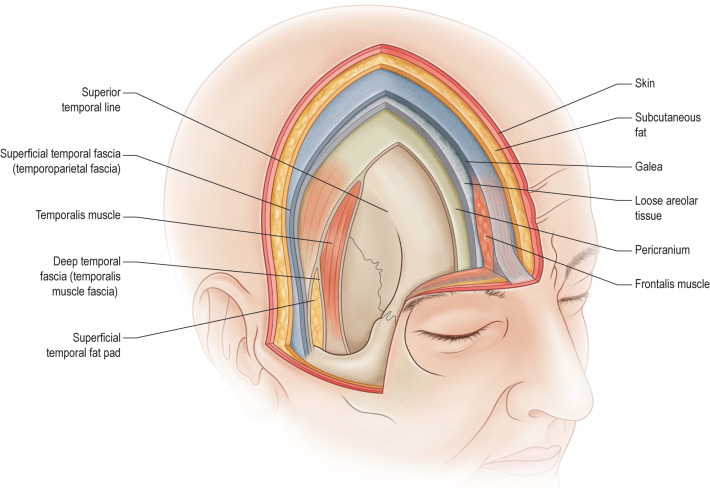
The surgical anatomy of the scalp has been extensively described. The scalp consists of five layers represented with the mnemonic “SCALP”: Skin, subCutaneous tissue, galea Aponeurosis, Loose areolar tissue, and Pericranium ( Fig. 3.6.1 ). The skin of the scalp is the thickest in the body, measuring 3 to 8 millimeters, and contains numerous sebaceous glands. The subcutaneous tissue consists of pilosebaceous appendages in addition to arteries, veins, and lymphatics. The galea is an inelastic musculoaponeurotic layer that is contiguous with the frontalis muscle anteriorly, the occipitalis muscles posteriorly, and the auricular muscles laterally. It continues inferiorly as the superficial musculoaponeurotic system (SMAS) and laterally as the superficial temporal fascia. Vertical septa extend from the skin to the galea, connecting these three layers such that they can be mobilized as one unit over underlying tissue planes. The loose areolar tissue, also known as subgaleal fascia in the temporal fossa, is an avascular plane that is safe for dissection. It is thinnest at the vertex and becomes thicker in the temporoparietal areas. Lastly, the pericranium is the periosteum of the calvarium and is anchored to the skull at suture lines.
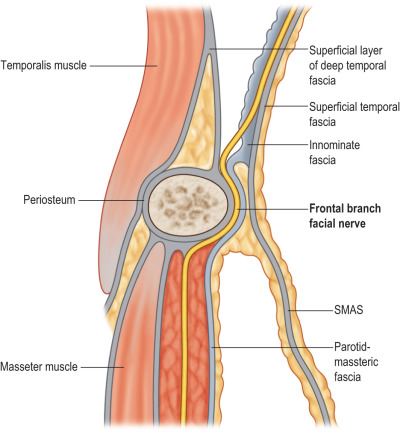
In the temporoparietal region, four subcutaneous layers can be defined ( Fig. 3.6.2 ). The superficial temporal fascia, which is also known as the temporoparietal fascia and the aforementioned lateral extension of the galea, is the most superficial layer that overlies the loose areolar tissue and is where the superficial temporal artery is located. Within the loose areolar tissue courses fibers from the frontal branch of the facial nerve. Beneath the loose areolar tissue is the deep temporal fascia that overlies the temporalis muscle and divides into superficial and deep layers that envelop the temporal fat pad above the zygomatic arch. Connections between the deep temporal fascia and the pericranium at the superior temporal line may need to be released to gain mobility during reconstruction. In general, the greatest mobility is achieved in the parietal area, with the least amount of mobility at the scalp vertex.
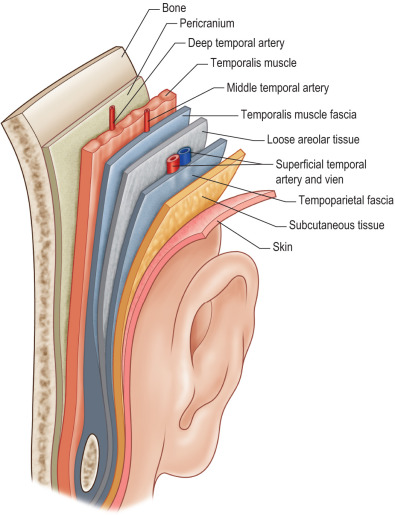
The scalp is highly vascular and is supplied by terminal branches of the internal and external carotid artery systems ( Fig. 3.6.3 ). The supraorbital and supratrochlear arteries arise from the ophthalmic artery and the first branch of the internal carotid artery, and pierce the frontalis muscle above the brow to supply the anterior scalp and forehead. The posterior scalp is supplied by branches of the external carotid artery, which mainly involve the occipital arteries that course along the vertebral muscles and can be located within 2 centimeters of midline at the nuchal line. The posterior auricular artery supplies the posterolateral areas. The superficial temporal artery, one of the terminal branches of the external carotid artery, supplies the lateral scalp. Traveling on the undersurface of the superficial temporal fascia, this artery bifurcates into frontal and parietal branches at the level of the superior helix to supply the anterior and posterior scalp, respectively, via interconnections with other angiosomes. In fact, due to the broad collateralization of the scalp blood supply, it is possible to replant the whole scalp based on only one vessel. The venous system parallels the arterial supply to drain externally into jugular veins, and also internally via emissary veins that connect to dural sinuses. Lymphatics drain into preauricular, postauricular, parotid, upper cervical, and/or occipital nodal basins.
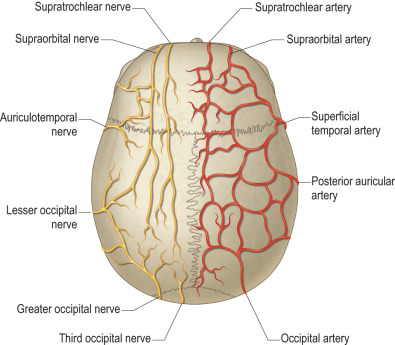
Motor and sensory innervation to the scalp is provided by frontal nerve branches, and nerves of spinal and trigeminal origin. The frontal branch of the facial nerve passes through the parotid approximately 2.5 centimeters anterior to the tragus and continues to course superiorly within the loose areolar tissue over the zygomatic arch; it can be encountered 1 to 2 centimeters lateral to the orbital rim ( Fig. 3.6.4 ). Injury to this nerve notably results in an inability to raise the ipsilateral brow. The posterior auricular branch of the facial nerve innervates the occipitalis muscles. Sensory innervation of the anterior scalp and forehead is from the supratrochlear and supraorbital branches of the ophthalmic division of the trigeminal nerve ( Fig. 3.6.5 ). The supratrochlear nerve enters through the superior orbital fissure and courses beneath the corrugator muscle to innervate the central forehead, in addition to the upper eyelid and conjunctiva. The supraorbital nerve also enters through the superior orbital fissure, then divides into a superficial branch that pierces the frontalis to innervate the central forehead, and into a deep branch that pierces the galea just medial to the superior temporal line to innervate the frontoparietal scalp. The posterior scalp is innervated by the greater and lesser occipital nerves, which have spinal nerve and plexus origins, respectively. The lateral scalp is supplied by branches of the trigeminal nerve, with the temporal region innervated by the zygomaticotemporal nerve from the maxillary division, and the preauricular area innervated by the auriculotemporal nerve from the mandibular division.