Scalp
OVERVIEW
Atopic dermatitis (AD) and infantile seborrheic dermatitis (referred to as cradle cap when it involves the scalp) are both eczematous eruptions. AD is the most common inflammatory skin condition in infants and children; it may be widespread or localized and might be the first sign of the “atopic march” that often precedes the development of another atopic disease such as asthma, hay fever, or other allergies. Infantile seborrheic dermatitis develops in areas of high sebaceous gland activity and tends to resolve at 6 to 8 months of age.
Birthmarks, such as nevus sebaceous and infantile hemangiomas (strawberry nevi), are visible skin lesions present at birth or shortly thereafter. They can be frightening to parents. Fortunately, the vast majority of congenital skin lesions or birthmarks are a benign, isolated finding, and parents can be reassured. A nevus can be either congenital (present at birth) or acquired. In children, benign nevi, also known as nevocytic nevi or common moles, tend to arise in the first 3 decades of life.
Head lice (pediculosis capitis) infestations caused by Pediculus humanus var.capitis are seen most often in children. In adults, chronic inflammatory scalp disorders such as dandruff, seborrheic dermatitis, atopic dermatitis, and psoriasis are frequent causes of discomfort and embarrassment, but do not generally result in permanent alopecia.
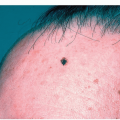
Benign neoplastic lesions such as seborrheic keratoses and cysts commonly appear on the scalp. Premalignant actinic keratoses, squamous cell carcinoma, and, less commonly, basal cell carcinoma arise on elderly patients with fair skin types who have had significant sun exposure in their lifetime.
INFANTS AND NEONATES
Infantile Seborrheic Dermatitis of the Scalp (“Cradle Cap”)
Infantile seborrheic dermatitis is a self-limited eruption that usually appears within the first 6 weeks of life. Most often, it presents on the scalp and is thus referred to as cradle cap; less commonly, it affects other areas of the body: behind the ears, in the creases of the neck, armpits, and diaper area (diaper rash).
The cause is unknown, but it possibly is due to overactive sebaceous glands in the skin of newborn infants from maternal hormones or by the skin yeast Pityrosporum ovale.
 Alert: It is important to note that infantile seborrheic dermatitis/cradle cap may ultimately prove to be an early manifestation of atopic dermatitis (see below), and rarely, psoriasis.
Alert: It is important to note that infantile seborrheic dermatitis/cradle cap may ultimately prove to be an early manifestation of atopic dermatitis (see below), and rarely, psoriasis.Distinguishing Features
Diagnosis
Clinical
Management
Cradle cap usually does not require medical treatment, as it usually resolves spontaneously
Mild antiseborrheic baby shampoos such as Sebulex and soft brushing may be used to remove the scales
If the scaling is heavy, mineral oil may be applied to the scalp for a couple of hours before shampooing
A medicated shampoo containing ketoconazole 1% (Nizoral) or a mild topical steroid such as 1% hydrocortisone cream or ointment (Cortaid, Cortisone 10) or fluocinolone 0.01% oil may be applied to any symptomatic (pruritic), inflamed, or reddened areas
Stronger keratolytic agents such as Salex cream or lotion, or Keralyt gel 6%, or salicylic acid in petrolatum can be used to remove thick, dense, adherent scale
 Figure 2-1 Infantile seborrheic dermatitis. Whitish scale stuck on or matted on the scalp. (Image courtesy of Robert I. Rudolph, MD.) |
 Figure 2-2 Infantile seborrheic dermatitis, cradle cap. Here the scale is thicker with yellowish greasy adherent scales. Thick greasy yellow scale that becomes stuck on the scalp is referred to as cradle cap. |
Infantile Atopic Dermatitis
Infantile atopic dermatitis is, by far, the most common cause of scalp rashes in infants. Atopic dermatitis is estimated to affect 15% to 20% of children worldwide. Symptoms begin during infancy (usually after 2 months) in more than half of the patients. It is a type of eczema that occurs in association with a family history of atopy (asthma, hay fever, allergic rhinitis).
The scalp and/or face is involved in almost all affected infants and the eruption can also become more generalized; however, it tends to improve with age.
 Figure 2-3 Infantile atopic dermatitis. Scale overlying erythema on the scalp, forehead, and temples in this infant. |
Distinguishing Features
Varying amounts of erythema and scale (Fig. 2-3)
Symptoms include pruritus, often indicated by the infants rubbing their scalp and head on crib bedding, or by pinching, scratching, or tapping affected areas. Clinical features are commonly indistinguishable from infantile seborrheic dermatitis.·Features of atopic dermatitis may become prominent after the cradle cap subsides
Diagnosis
Family history of atopy and physical examination
Management
Treatment can be initiated with a mid-strength (class 3 or 4) cream or ointment such as mometasone 0.1% ointment (Elocon) or fluticasone 0.05% cream or 0.005% ointment (Cutivate).
Low-potency, nonfluorinated topical steroids (class 6 or 7) or, if necessary, a higher-potency (class 5) steroid that is used for several days before it is changed to a lower-potency agent
Tacrolimus (Protopic) ointment 1% or pimecrolimus (Elidel) cream 1% is applied once or twice daily for longer-term use
Crisaborole 2% cream or ointment (Eucrisa) is a phosphodiesterase inhibitor. It is a nonsteroidal agent which can be applied without concern regarding steroid atrophy in intertriginous locations. Approved primarily for the treatment of eczema in children >3 months of age
 Figure 2-4 Infantile hemangioma. The most common tumor of infancy. The bright red color and firm rubbery appearance are typical of an IH in the growth phase. |
Infantile Hemangioma
An infantile hemangioma (IH), also called strawberry hemangioma, is the most common tumor of infancy, present in 5% to 10% of all infants. IH is more common in female infants and low-birth-weight newborns (see also Cheeks).
Distinguishing Features
IH is not present at birth
It arises in the first few weeks of life with a precursor lesion that can appear as a bluish or red bruise-like patch
Fully developed IH appears as a red lobulated nodule likened to a strawberry (Fig. 2-4)
IH has characteristic natural history consisting of three phases:
The rapid proliferation phase: 3 weeks until 6 to 7 months of age; an IH enlarges rapidly and appears red, firm and has a rubbery texture
The plateau (or late proliferative) phase: variable length, usually 7 to 12 months of age
The involution phase: usually starts at 1 year of age and is a gradual process that can last for years; the color continues to fade and some lesions involute completely while others leave a fibrofatty residua (Fig. 2-5)
Complications
Ulceration is the most common complication and is heralded by a gray-white color during the proliferative phase (Fig. 2-6).
IH in certain locations and of certain morphologies are at higher risk for development of complications and/or associated systemic involvement. For example, an IH in the perineum is at highest risk for early ulceration, an IH in the
central face can lead to permanent cosmetic disfigurement. IH can obstruct the oral cavity, respiratory tract, or may impair vision or breathing.
central face can lead to permanent cosmetic disfigurement. IH can obstruct the oral cavity, respiratory tract, or may impair vision or breathing.
 Figure 2-5 Infantile hemangioma, involution phase. Red color is breaking apart and texture is soft and spongy. The hemangioma is being replaced with fibrofatty tissue. |
 Figure 2-6 Infantile hemangioma, ulcerating. Ulceration is the most common complication of IH and occurs during the growth phase. |
Diagnosis
Diagnosis is clinically based on the typical morphology and characteristic growth pattern
Differential Diagnosis
Early IH (macular phase) may be difficult to distinguish from a port wine stain
Management
The vast majority of IHs will proliferate and involute with minimal consequence. In these cases, nonintervention is the treatment of choice and consists of education on the natural history of IH, close monitoring, and reassurance. If necessary:
Topical timolol 0.5% gel-forming solution is a nonselective beta-blocker that is highly effective for ulcerated and superficial hemangiomas. Other topical treatments include imiquimod, laser therapy, as well as mid to superpotent topical corticosteroids that can also halt growth and hasten involution
Systemic treatments include intralesional or systemic corticosteroids
The nonselective beta-blocker, propranolol, has become the first-line treatment for IH requiring systemic therapy, given its greater efficacy and better side effect profile compared to systemic corticosteroids
 Alert: High-risk hemangiomas should be treated early and patients should be referred to those with experience in treating complications of IH.
Alert: High-risk hemangiomas should be treated early and patients should be referred to those with experience in treating complications of IH.It is important to recognize those IHs that are at high risk for complications (i.e., ulceration, cosmetic disfigurement, and interference with vital functions) or associated anomalies.
Prior to propranolol initiation for IH, the patient’s medical and family history should be reviewed and a baseline cardiopulmonary evaluation should be performed if necessary.
Aplasia Cutis Congenita
Aplasia cutis congenita (ACC) is an uncommon congenital defect that results in a localized area of absent skin at birth. ACC is most often seen on the scalp. The exact cause of ACC is unknown and most cases are sporadic. Proposed theories include genetic factors, birth trauma, teratogens, and intrauterine infection.
ACC is an isolated defect in the majority of cases, but it can be associated with other developmental anomalies or syndromes. The so-called hair collar sign may indicate an underlying bony or neurologic abnormality.
Distinguishing Features
Most often an ACC presents on the scalp as a single, localized area of smooth alopecia in close proximity to the hair whorl. Lesions are usually sharply demarcated, oval, circular, or stellate, and measure 1 to 3 cm in diameter
A ring of long, dark hair around membranous aplasia cutis (hair collar sign) is thought to herald an underlying neural tube defect (Fig. 2-7)
Usually there is absence of the epidermis and dermis in the affected area, but occasionally subcutaneous tissues, bone, and dura can also be missing
Less commonly, ACC presents as multiple areas of alopecia on the scalp or can be found on the face, trunk, or extremities
ACC can have a variable appearance at birth including a well-formed hairless scar, ulceration with a granulating base, a superficial erosion, or a translucent, glistening membrane (membranous aplasia cutis), an uncommon variant
Lesions heal with scarring and alopecia (Fig. 2-8)
Diagnosis
Diagnosis is clinical
Differential Diagnosis
Birth-related skin injury from forceps or scalp electrodes (the birth history will reveal use of instruments)
Erosion from herpes simplex virus (HSV)
 Figure 2-7 Aplasia cutis congenita, hair collar sign. Two lesions of aplasia cutis congenita on the scalp, both with a surrounding “hair collar sign” which can signal an underlying neural tube defect. (Image courtesy of Seth J. Orlow, MD, PhD.) |
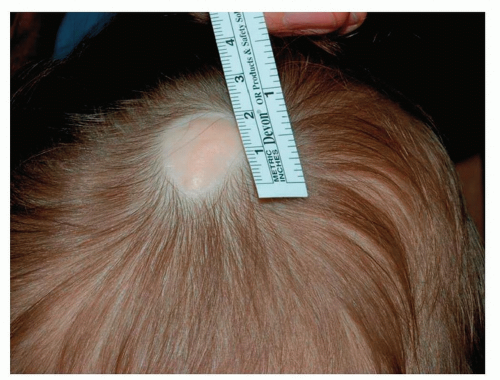 Figure 2-8 Aplasia cutis congenita, with scarring and alopecia. The lesion persists as a well-healed scar that lacks hair follicles. (Image courtesy of Seth J. Orlow, MD, PhD.) |
Management
Prognosis is excellent and most lesions heal completely in the first weeks to months of life
Conservative wound care with antibiotic ointments and nonstick dressings will help heal most small defects quickly
Most scars become relatively inconspicuous and require no correction but large and/or obvious scars can be treated with plastic surgical reconstruction in the future
If the lesion appears large, deep, or stellate or if located in the midline, a radiologic evaluation to assess for an underlying defect is necessary
Nevus Sebaceous
Nevus sebaceous (NS) is a common congenital hamartoma (benign tumor) composed of malformed sebaceous glands, apocrine glands, and follicular units. NS occurs sporadically and represents a defect in cutaneous embryologic development. It can occur anywhere on the body, but greater than 97% of lesions occur on the head or neck, but most often on the scalp.
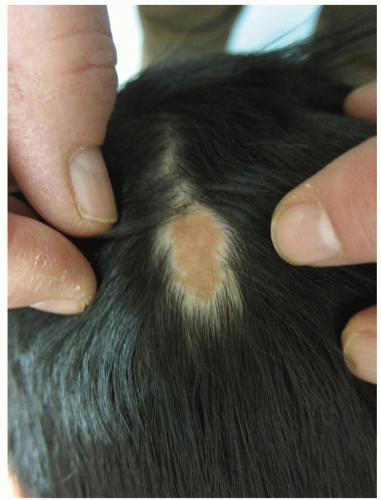 Figure 2-9 Nevus sebaceous. Typical tan color, oval shape of a nevus sebaceous. |
Distinguishing Features
NS initially presents as a solitary, well-circumscribed, oval or linear, hairless, pink or yellow-orange/tan, finely papulated plaque (Fig. 2-9)
Occasionally, NS can be thicker or have papillomatous projections, simulating a wart; or present as a large lesion at birth (Fig. 2-10)
After infancy, lesions flatten and grow proportionately as the child grows
At puberty, under the influence of androgens, NS thickens, becomes darker yellow or brown, more papular or verrucous
Warty growths, representing secondary adnexal neoplasms, may develop within an NS during adolescence or later
A possible complication that may occur later in life is the development of a secondary neoplasm, such as a basal cell carcinoma as well as other benign and malignant neoplasms within the lesionRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree