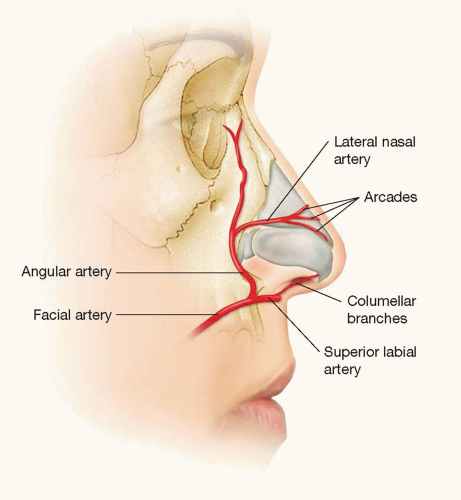
 FIGURE 48.1. Blood supply to the nose. |
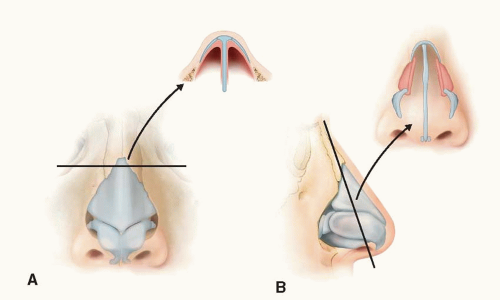 FIGURE 48.2. A. Upper cartilaginous framework. B. Note the “keystone area” where the nasal bones overlap the upper lateral cartilages and the “scroll area” where the lower lateral cartilages overlap the upper lateral cartilages. |
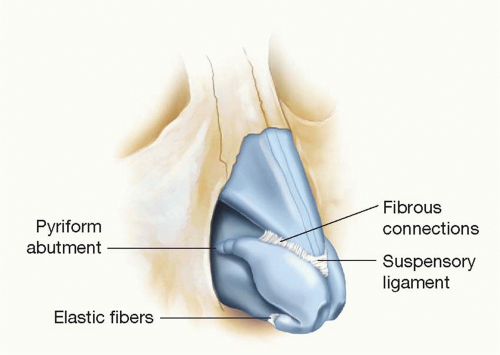 FIGURE 48.3. Ligamentous support of the cartilaginous framework. |
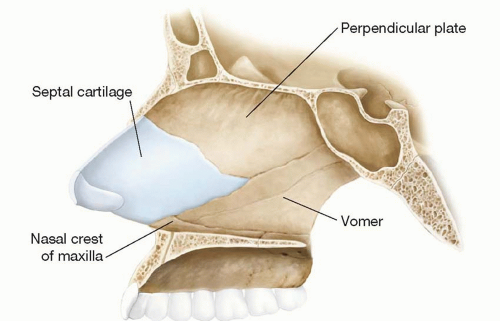 FIGURE 48.4. Anatomy of the nasal septum. |
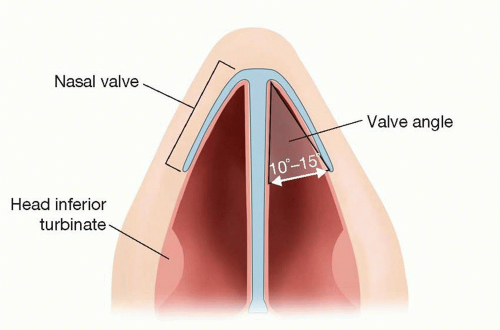 FIGURE 48.5. Internal nasal valve. |
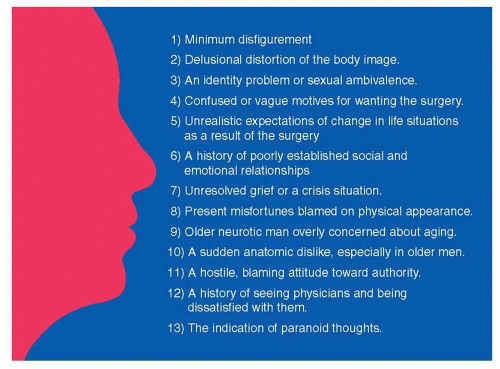 FIGURE 48.6. “Danger signs” that may indicate the patient has underlying psychological issues. |
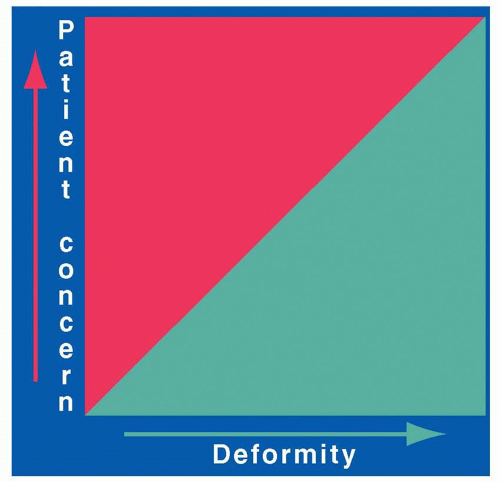 FIGURE 48.7. “GorneyGram” comparing patient concern with the actual degree of deformity. |
The face is divided into thirds using horizontal lines tangent to the hairline, brow (at the level of the supraorbital notch), nasal base, and chin (menton). The upper third (between the hairline and the brow) is the most variable, as it depends on the hairline and hairstyle, and therefore is the least important. The middle third lies between the brow and the nasal base. The lower third of the face can be subdivided into thirds by visualizing a horizontal line between the oral commissures (stomion). The upper third of this subdivision lies between the nasal base and the oral commissures and the lower two-thirds between the commissures and the menton (Figure 48.8). Deviation from these proportions may signal an underlying craniofacial anomaly, such as vertical maxillary excess or maxillary hypoplasia, that may need to be addressed prior to rhinoplasty (Chapter 25).
The nasal length (radix-to-tip, or R-T) should be equivalent to the stomion-to-menton distance (S-M) (Figure 48.9).
The lip-chin relationship is assessed by dropping a vertical line from a point one-half the ideal nasal length tangent to the vermillion of the upper lip. The lower lip should lie approximately 2 mm behind this line. The ideal chin position varies with gender, with the chin lying slightly posterior to the lower lip in women, but equal to the lower lip in men. Orthodontics, a chin implant, or orthognathic surgery may be necessary to improve overall facial harmony if there is a discrepancy in these relationships (Figure 48.10).
The nose itself is addressed from the anteroposterior view. A vertical line is drawn from the midglabellar
area to the menton, bisecting the nasal ridge, upper lip, Cupid’s bow, and central incisors (if the patient has normal occlusion). Any nasal deviation from this line is likely to require septal surgery (Figure 48.11).
TABLE 48.1 SYSTEMATIC NASAL ANALYSIS
Frontal view
Facial proportions
Skin type/quality—Fitzpatrick type, thin or thick, sebaceous
Symmetry and nasal deviation—midline, C-, reverse C-, S- or S-shaped deviation
Bony vault—narrow or wide, asymmetrical, short or long nasal bones
Midvault—narrow or wide, collapse, inverted V deformity
Dorsal aesthetic lines—straight, symmetrical or asymmetrical, well or ill defined, narrow or wide
Nasal tip—ideal/bulbous/boxy/pinched, supratip, tip-defining points, infratip lobule
Alar rims—gull shaped, facets, notching, retraction
Alar base—width
Upper lip—long or short, dynamic depressor septi muscles, upper lip crease
Lateral view
Nasofrontal angle—acute or obtuse, high or low radix
Nasal length—long or short
Dorsum—smooth, hump, scooped out
Supratip—break, fullness, pollybeak
Tip projection—over- or underprojected
Tip rotation—over- or underrotated
Alar-columellar relationship—hanging or retracted alae, hanging or retracted columella
Periapical hypoplasia—maxillary or soft-tissue deficiency
Lip-chin relationship—normal, deficient
Basal view
Nasal projection—over- or underprojected, columellar-lobular ratio
Nostril—symmetrical or asymmetrical, long or short
Columella—septal tilt, flaring of medial crura
Alar base—width
Alar flaring
From Rohrich RJ, Ahmad J. Rhinoplasty. Plast Reconstr Surg. 2011; 128:49e-73e.
The curvilinear dorsal aesthetic lines are traced from their origin at the supraorbital ridges toward their convergence at the level of the medial canthal ligaments. From here, they flare slightly at the keystone area and then track down to the tip-defining points, slightly diverging from each other along the dorsum during their course. The ideal width of the dorsal aesthetic lines should be approximately equivalent to the width between the tip-defining points or the interphiltral distance (Figure 48.12).
The normal alar base width is equivalent to the intercanthal distance, or the transverse dimension from the medial to lateral canthus. If the alar base width is greater than the intercanthal distance, the underlying etiology is examined. If the discrepancy is the result of a narrow intercanthal distance, it is better to maintain a slightly wider alar base. If there is true increased interalar width, a nostril sill resection may be indicated. If the increase in width is secondary to alar flaring (greater than 2 to 3 mm outside the alar base), an alar base resection should be considered. The bony base should equal approximately 80% of the alar base width (Figures 48.13 A and B). If the bony base is greater than 80% of the alar base width, osteotomies may be required. Over-narrowing the dorsum should be avoided in males as this can lead to an “over-feminized” look.
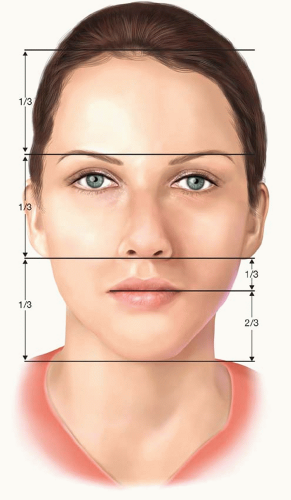
FIGURE 48.8. The face is divided into thirds, using horizontal lines tangent to the hairline, brow, nasal base, and chin.
The alar rims are examined for symmetry. They should normally flare slightly outward in an inferolateral direction (Figure 48.14).
The tip is assessed by drawing two equilateral triangles with their bases opposed (Figure 48.15). The supratip break, tip-defining points, and columellar-lobular angle serve as landmarks. If these triangles are asymmetric, the patient will likely require tip modification.
The final assessment on frontal view is of the outline of the alar rims and the columella. Normally, this outline should resemble a seagull in gentle flight. If the angles
are too steep, the patient likely has an increased infratip lobular height. Conversely, if the angle/curve is too flattened, it is likely the patient has decreased columellar show, which may require columellar and/or alar rim modification (Figure 48.16).
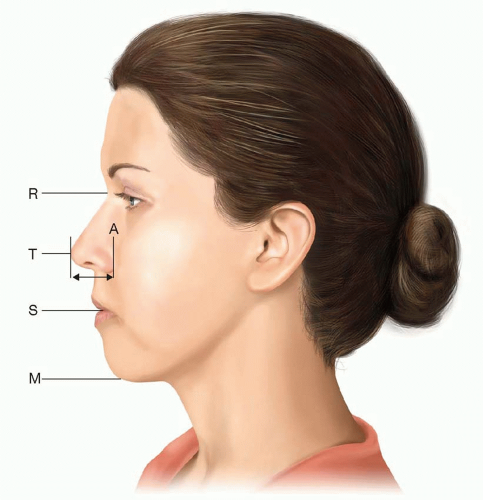
FIGURE 48.9. The ideal nasal length is equivalent to the stomion-to-menton distance. A, ala; M, menton; R, radix; S, stoma; T, tip.
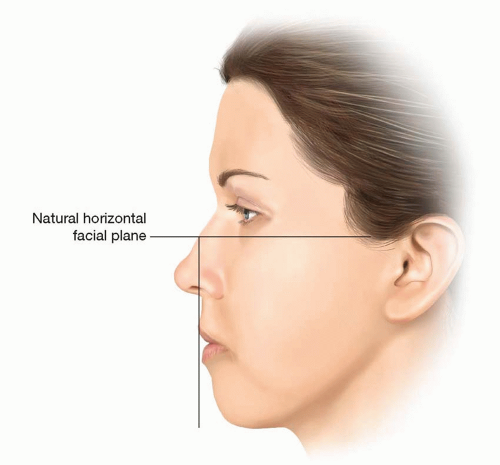
FIGURE 48.10. The ideal lower lip position is 2 mm behind a vertical line dropped from a point half the ideal nasal length along the natural horizontal facial plane.
The basal view of the nose is examined focusing on the outline of the nasal base and the nostrils themselves. The outline of the nasal base should describe an equilateral triangle with a lobule-to-nostril ratio of 1:2 (Figure 48.17). The nostril itself should have a teardrop geometry, with the long axis oriented in a slight medial direction (from base to apex).
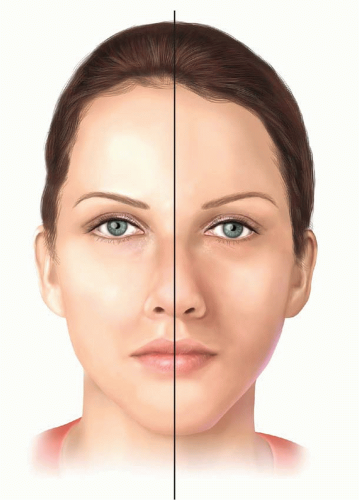
FIGURE 48.11. Symmetry is determined by drawing a vertical line from the midglabellar area to the menton.
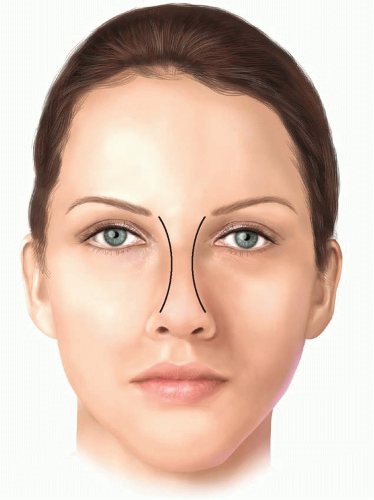
FIGURE 48.12. The curvilinear dorsal aesthetic lines extend from the supraorbital ridges to the tip-defining points.
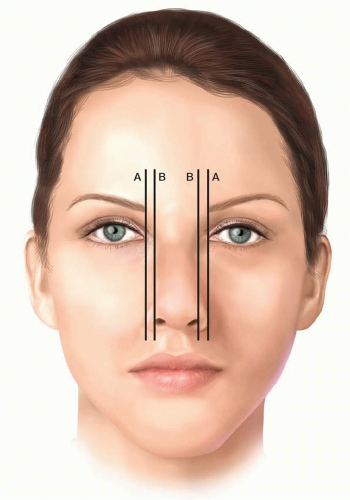
FIGURE 48.13. A. The normal alar base width equals the intercanthal distance, or the width of one eye. B. The bony base should be approximately 80% of the alar base width.
Attention is turned to the lateral view, beginning with analysis of the nasofrontal angle. This angle connects the brow and nasal dorsum through a soft concave curve. The apex of this angle (radix) should lie between the supratarsal fold and the upper lid lashes, with the eyes in primary gaze. The nasofrontal angle can vary between 128° and 140°, but is ideally approximately 134° in females and 130° in males.
It is important to note that the perceived nasal length and tip projection can be altered by the position of the nasofrontal angle. For instance, the nose appears longer if the nasofrontal angle is positioned more anteriorly and superiorly than normal. In this instance, the nasofacial angle (as defined by the junction of the nasal dorsum with the vertical facial plane) is decreased and the tip projection will appear diminished (yellow line). Conversely, the nose can appear shorter if the nasofrontal angle is positioned too posteriorly and/or inferiorly. In this case, the tip may also appear more projecting (red line; Figure 48.18). Ideally, the nasofacial angle should measure 32° to 37°.
While still analyzing the lateral view, tip projection is addressed. This can be done in two ways. The first is to draw a horizontal line from the alar-cheek junction to the tip of the nose. The distance between these points should equal two things: (1) the alar base width, and (2) 0.67 × R-T (radix-to-tip) (Figures 48.19A and B). The second way to assess tip projection is to examine how much of the tip lies anterior to a vertical line tangent to the most projecting part of the upper lip vermillion. If 50% to 60% of the tip lies anterior to this line, projection is considered normal. If the tip projection is outside of these proportions, it likely will require tip modification (Figure 48.20).
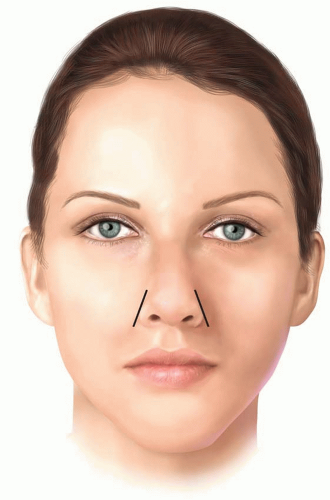
FIGURE 48.14. The alar rims should flare outward inferolaterally.
The dorsum is analyzed by drawing a line from the radix to the tip-defining points. In women, the ideal aesthetic nasal dorsum should lie approximately 2 mm behind and parallel to this line, but in men, it should approach this line to avoid feminizing the nose (Figure 48.21).
The degree of supratip break is also evaluated on the lateral view. This break helps to define the nose and separate the tip from the dorsum. A slight supratip break is preferred in women but not in men.
The degree of tip rotation is assessed by evaluating the nasolabial angle, which is the angle formed between a line coursing through the most anterior and posterior edges of the nostril and a plumb line dropped perpendicular to the natural horizontal facial plane (Figure 48.22). This angle is usually 95° to 100° in women and between 90° and 95° in men.
The nasolabial angle is often confused with the columellarlobular angle, which is formed at the junction of the columella with the infratip lobule (Figure 48.23). This angle is normally 30° to 45°. A prominent caudal septum can cause
increased fullness in this area, which can give the illusion of increased rotation, despite a normal nasolabial angle.
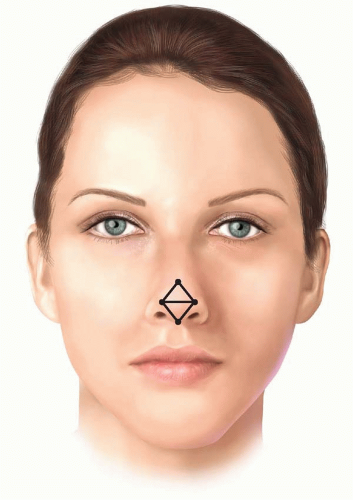
FIGURE 48.15. Tip assessment is performed by analyzing two equilateral triangles with opposing bases.
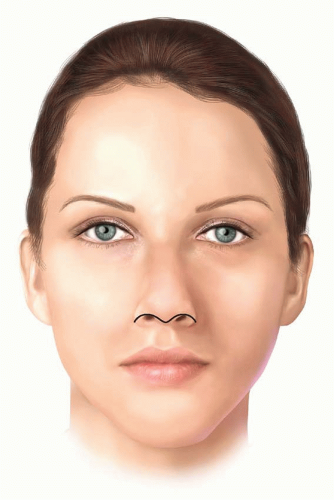
FIGURE 48.16. The outline of the alar rims and columella should resemble a “seagull in gentle flight.”
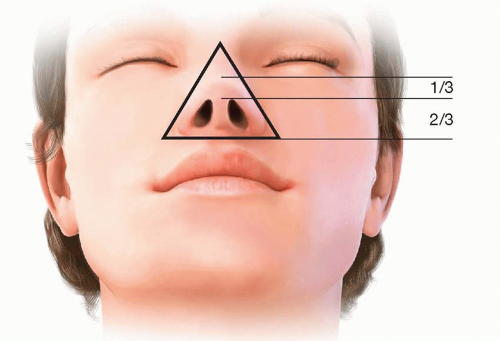
FIGURE 48.17. The outline of the nasal base should resemble an equilateral triangle with a lobule-to-nostril ratio of 1:2.
The alar-columellar relationship is assessed by drawing a line through the long axis of the nostril and a second, perpendicular line drawn from the alar rim to the columellar rim that bisects this axis. If the alarcolumellar relationship is normal, the distance from the alar rim (“point A”) to the long axis line (“point B”) should equal the distance between the long axis line and the columellar rim (“point C”) (AB = BC ≈ 2 mm) (Figure 48.24). If abnormal, the deformity can be stratified into six classes.29 Classes I to III describe increased columellar show, while classes IV to VI demonstrate decreased columellar show. The treatment of the discrepancy varies by class.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








