 For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
Introduction
The nose is a multifarious structure with critical mechanical and functional roles, which by virtue of its position, serves as the central and salient component of the face. Its relationship to surrounding structures is in part responsible for a harmonious, pleasing form as a whole. Functionally, the nose provides an airway and acts to warm, filter, and humidify air passing through it. Noses that deviate from ideal structural proportions – whether subtle variations of normal or more dramatic posttraumatic or neoplastic deformities – have motivated rhinoplasty surgeons since ancient India 800 BCE.
Anatomy
A thorough appreciation and understanding of relevant anatomy is crucial for all surgery. Obviously, recognition of the nuances and subtle variations of nasal anatomy is absolutely vital for execution of a successful rhinoplasty.
Skin
A thorough rhinoplasty evaluation must assess skin type and thickness. The surgeon must anticipate the advantages and limitations afforded by a particular skin type. In general, thin skin is unlikely to camouflage even minor irregularities in the underlying cartilaginous and osseous structures, particularly with grafting. In contrast, thick skin conceals imperfections in the nasal skeleton and may hide surgical flaws or reduce the desired definition intended from alteration of underlying cartilage and bone. Sebaceous skin can give the tip a bulbous appearance . The skin is thickest at the nasion. More caudally, the remaining upper half of nose tends to have skin that is thinner and more mobile than the lower half. In the tip area, there tend to be more sebaceous glands. However, in the infratip region, the columella and ala again are usually covered with thinner skin. 2,3.
Cartilaginous and Bony Support
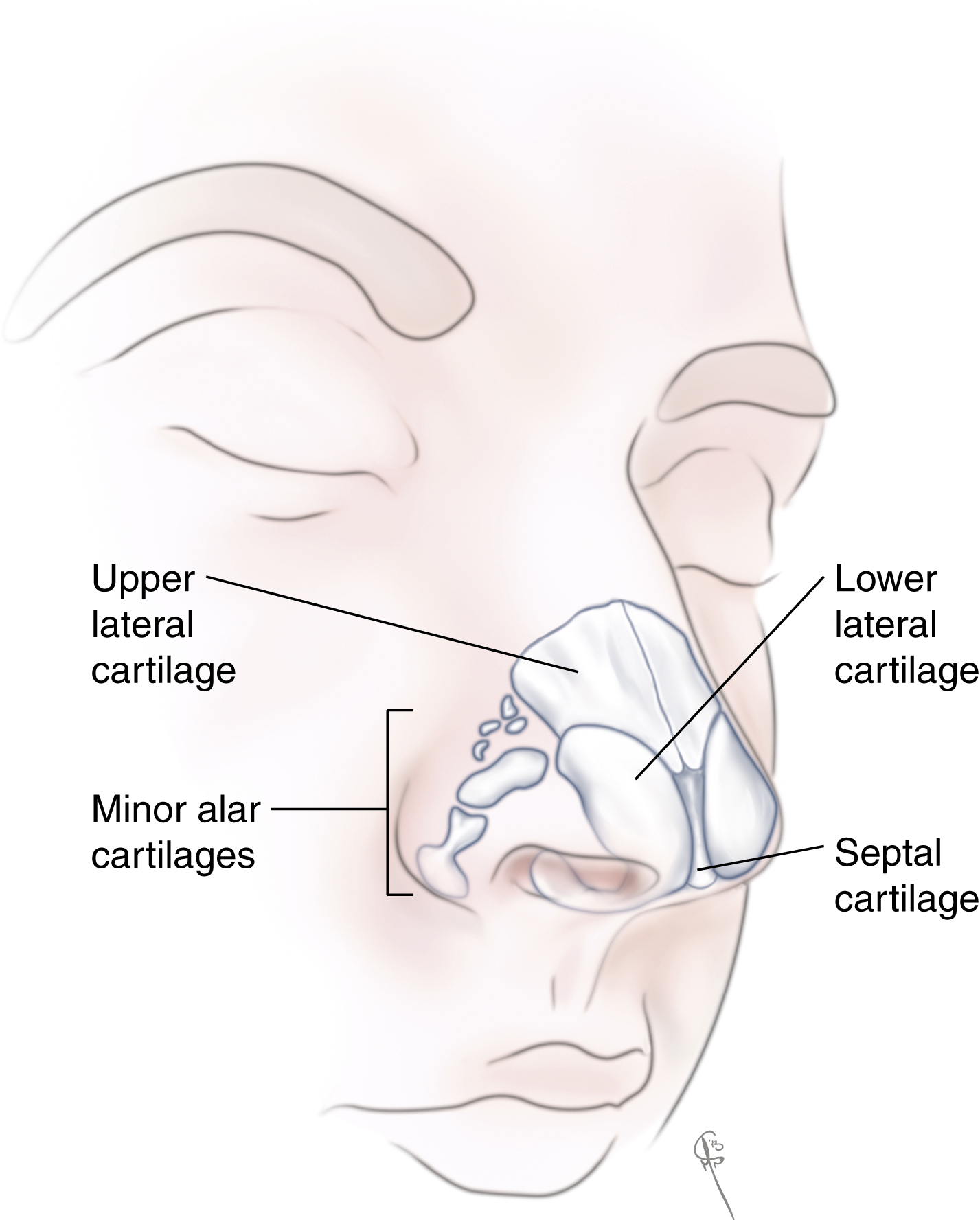
An understanding of the bony and cartilaginous structural components of the nose should be complemented by correlation with landmarks of the surface anatomy ( Fig. 68.1 ). Caudal to the glabellar protrusion, the deepest point of the surface of the nose is referred to as the radix. The root of the nose, just caudal to the nasofrontal suture line, is referred to as the nasion, minor adjustments of which can change the overall character of the nose. The rhinion describes the position along the dorsum where the nasal bones articulate with the upper lateral cartilages and the pronasale refers to the region extending from the supratip break, including the tip and infratip lobule, to the anterior-most aspect of the columella. The tip-defining points are the anterior-most points of the nose corresponding to the intermediate crura of the lower lateral cartilages.
Nasal Bones
The bony vault is pyramidal in shape and comprises the paired nasal bones that articulate with the frontal bone superiorly and the ascending maxillary processes laterally. The bony pyramid is narrowest at the level of the intercanthal line and widens inferiorly. The nasal bones are thickest cephalically and become thinner caudally. , The nasal bones are supported superiorly at the nasofrontal suture line, laterally at their articulation with the ascending process of the maxilla, and dorsally at their fusion with the perpendicular plate of the ethmoid. The junction between the upper third and lower two-thirds of the nose where the cartilaginous septum meets the nasal bones is referred to as the “keystone area,” as this area is essential for structural support, and stabilizing the nasal dorsum for height and projection.
Upper Lateral Cartilages
The upper lateral cartilages articulate with the septum and extend cephalically and laterally. The upper lateral cartilages are supported primarily by their connection with the nasal bones and frontal process of maxilla. On their deep surface, they are lined by perichondrium that is continuous with the septal perichondrium. Their articulation with the septum forms the internal nasal valve; the angle should be between 9 and 15 degrees.
Lower Lateral Cartilages
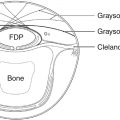
The lower lateral cartilages (LLC) are paired structures in the caudal third of the nose that can be subdivided into three segments: the lateral, intermediate/middle, and medial crura ( Fig. 68.2 ). The lateral crus supports the alar rim. The scroll area is the region where the superior edge of the lower lateral cartilage curls downward as it meets the inferior edge of the upper lateral cartilage. This area provides some support for the internal nasal valve. Superior and lateral to the scroll area, one can find several small sesamoid cartilages connected by fibrous tissue that wraps around the alae laterally. , The intermediate crus has the most variability in shape and may be convex, boxy, broad or concave; it forms the tip-defining point. It should be noted that skin over this region is particularly delicate as there is a deficiency of subcutaneous tissue: the skin directly abuts the perichondrium necessitating meticulous dissection. The medial crura sit next to each other in the columella. The footplate is the area closest to the nasal spine where variable degrees of divergence exist. The columellar segment, the middle portion of the columella, extends towards the intermediate crura where the cartilages may diverge again to reach the tip-defining points.
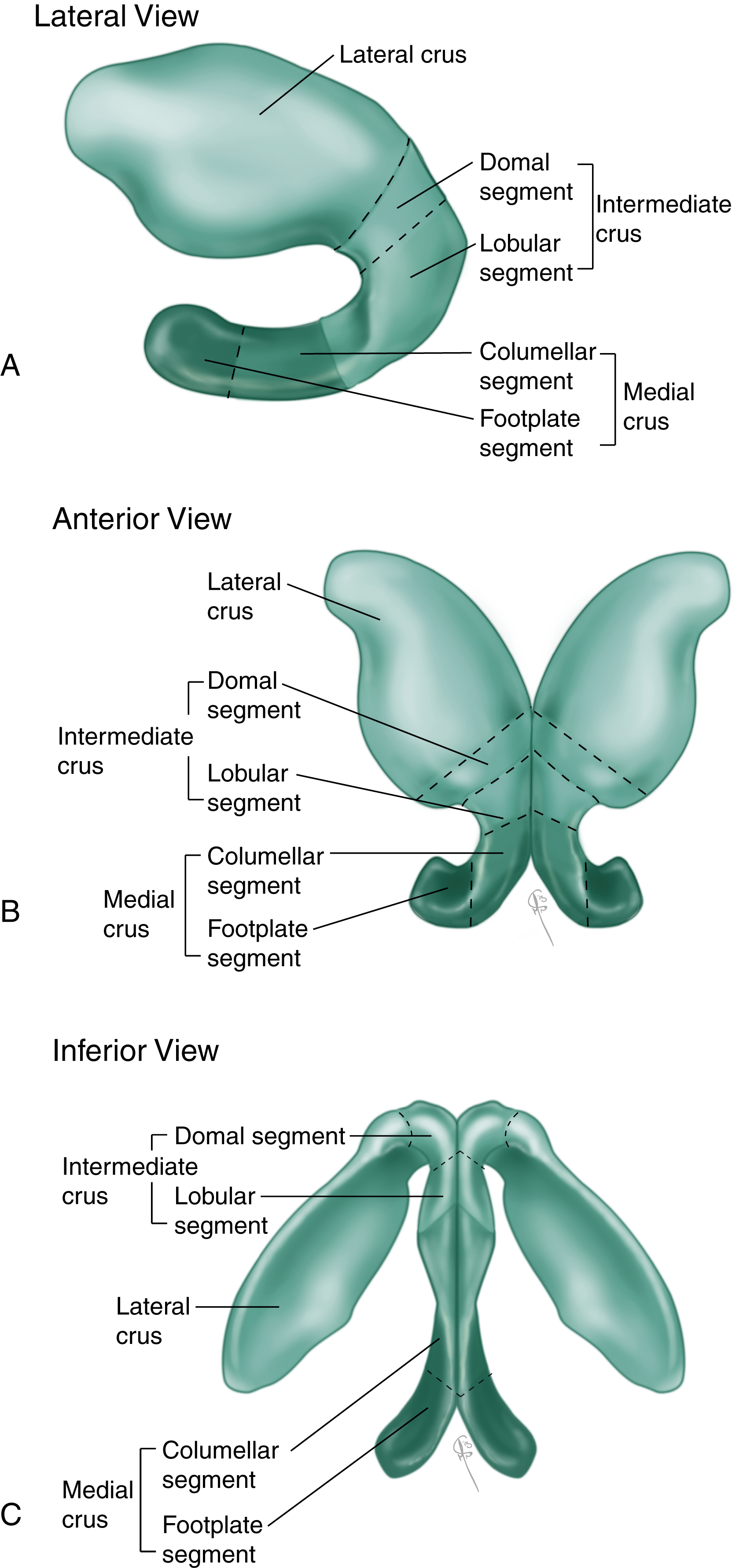
Several analogies have been proposed to describe the dynamics of tip rhinoplasty, relating the medial and lateral crura of the lower lateral cartilages and their attachment to the caudal septum to tip support, projection, and rotation. The “tripod concept” of the nasal base is the most popular analogy for understanding the interdependent relationships of the nasal base structures. This theory proposes that the nasal base structurally functions like a tripod with the paired medial crura acting as one leg of the tripod and each of the lateral crura acting as one of the other two tripod legs . Altering the length or strength of the legs will result in changes of the rotation and projection of the tip. While the tripod theory has ample utility in the understanding and planning of surgery, , it has limitations in that it may not be the most accurate predictor of the true forces on the nasal tip. Westreich et al. proposed an alternate model, which extrapolates on the tripod concept described as a “cantilevered spring tripod.” They measured stiffness and elastic modulus of the different cartilages and found that the septal cartilage had the greatest tensile strength. They also found that the strength and support of the nasal tip depended greatly on the thickness of the cartilage and perichondrial attachments more than the elastic modulus of the particular cartilage. With these findings, they proposed considering the nasal tip as a cantilever from the caudal septum. .
Septum
The septum is comprised of bony and cartilaginous portions. The bony septum is made up of the perpendicular plate of the ethmoid bone superiorly, the vomer inferiorly and posteriorly, and the maxillary crest, which forms the caudal-most projection of the premaxilla, anteriorly and inferiorly. The cartilaginous septum is composed of a single continuous quadrangular cartilage that articulates with the vomer and the perpendicular plate of the ethmoid posteriorly and superiorly and is supported inferiorly by the maxillary crest. The anterior aspect of the quadrangular cartilage supports the nasal dorsum and provides tip projection. The anterior septal angle supports the nasal tip with attachments to the medial crura of the lower lateral cartilages. The posterior septal angle articulates with the anterior-most portion of the maxillary crest. The amount of cartilage in the quadrangular cartilage varies among patients and is typically less robust in non-Caucasian patients.
SMAS
In the nose, the SMAS is a continuation of the subcutaneous musculoaponeurotic system, which is contiguous from the galea to platysma. Muscles associated with the nose within the SMAS can be categorized into elevators and depressors of the nasal tip. The elevator muscle group includes the procerus, levator labii superioris, alaque nasi, and the anomalous nasi. Depressors include the alar and transverse portions of the nasalis, the dilator naris posterior, depressor septi nasi, and compressor narium.
Blood Supply
Understanding the blood supply of the nose is important in order to avoid ischemic consequences if this rich blood supply is inadvertently and sufficiently disrupted. The dorsal nasal artery, a branch of the ophthalmic artery, penetrates the orbital septum above the medial palpebral ligament and courses along the side of the nose, providing robust blood supply to the dorsal nasal skin. It ultimately anastomoses with the lateral nasal artery, a branch of the angular artery (itself the terminal branch of the facial artery), with numerous branches that enter the subdermal plexus thereby supplying the lateral surface of the caudal nose. The tip of the nose is supplied both by the external nasal branch of the anterior ethmoid artery (a branch of the ophthalmic artery), the columellar artery (a branch of the superior labial artery), and branches of the lateral nasal artery. The external nasal branch of the anterior ethmoid artery passes between the nasal bone and the upper lateral cartilage to supply skin of the nasal tip. Branches of the superior labial artery supply the nostril sill and columellar base ( Fig. 68.3 ). Intranasal blood supply is from branches of the anterior and posterior ethmoid arteries, the superior labial and greater palatine arteries, and the maxillary artery.
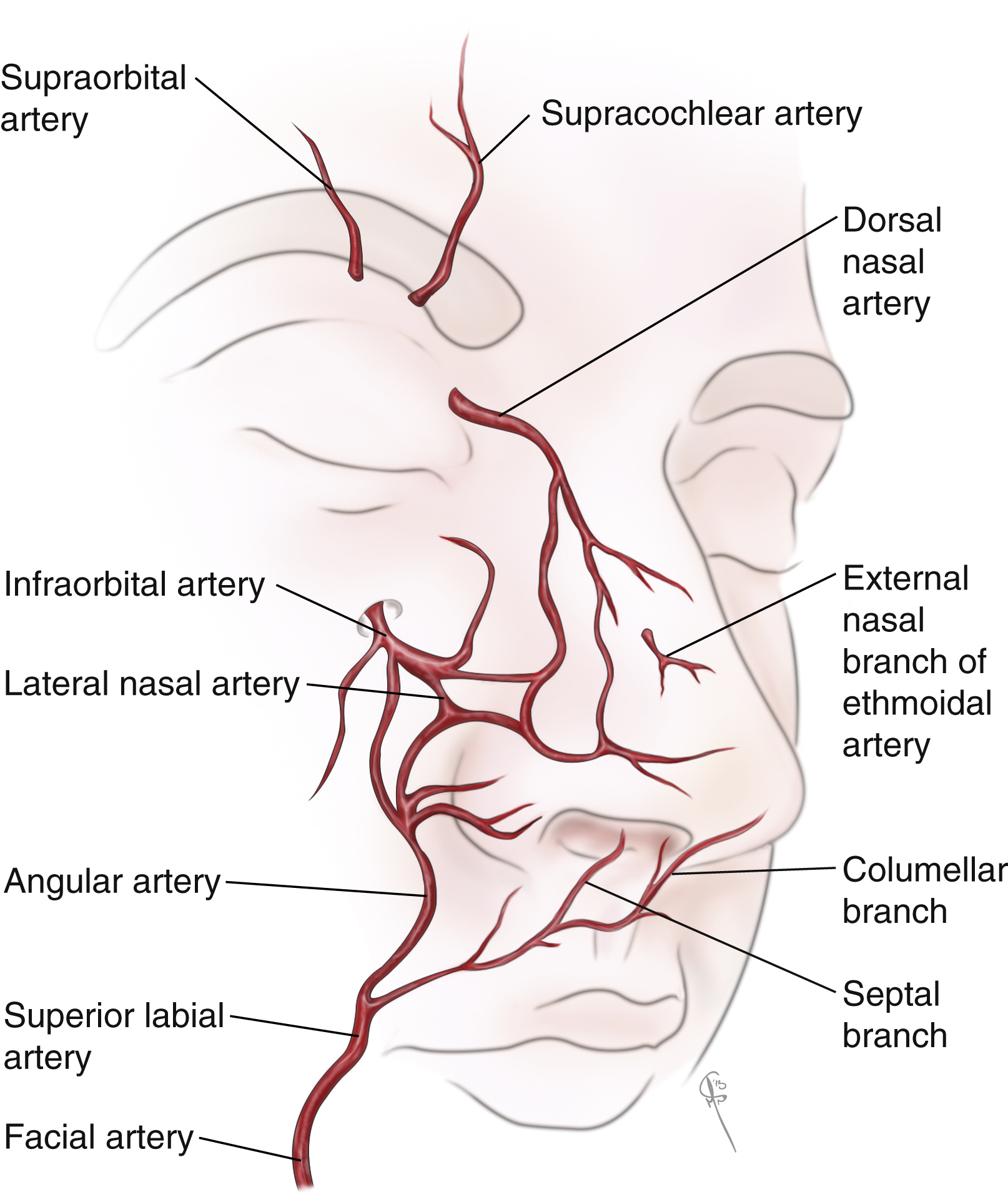
Venous drainage of the external nose generally consists of veins with names that correspond to the associated arteries, which veins drain through the facial vein, the pterygoid plexus, and ophthalmic veins, the pterygoid plexus and the facial vein. Lymphatic drainage of the nasal tip follows the same path and appears to be limited to the lateral walls, sparing the columella.
Nerve Supply
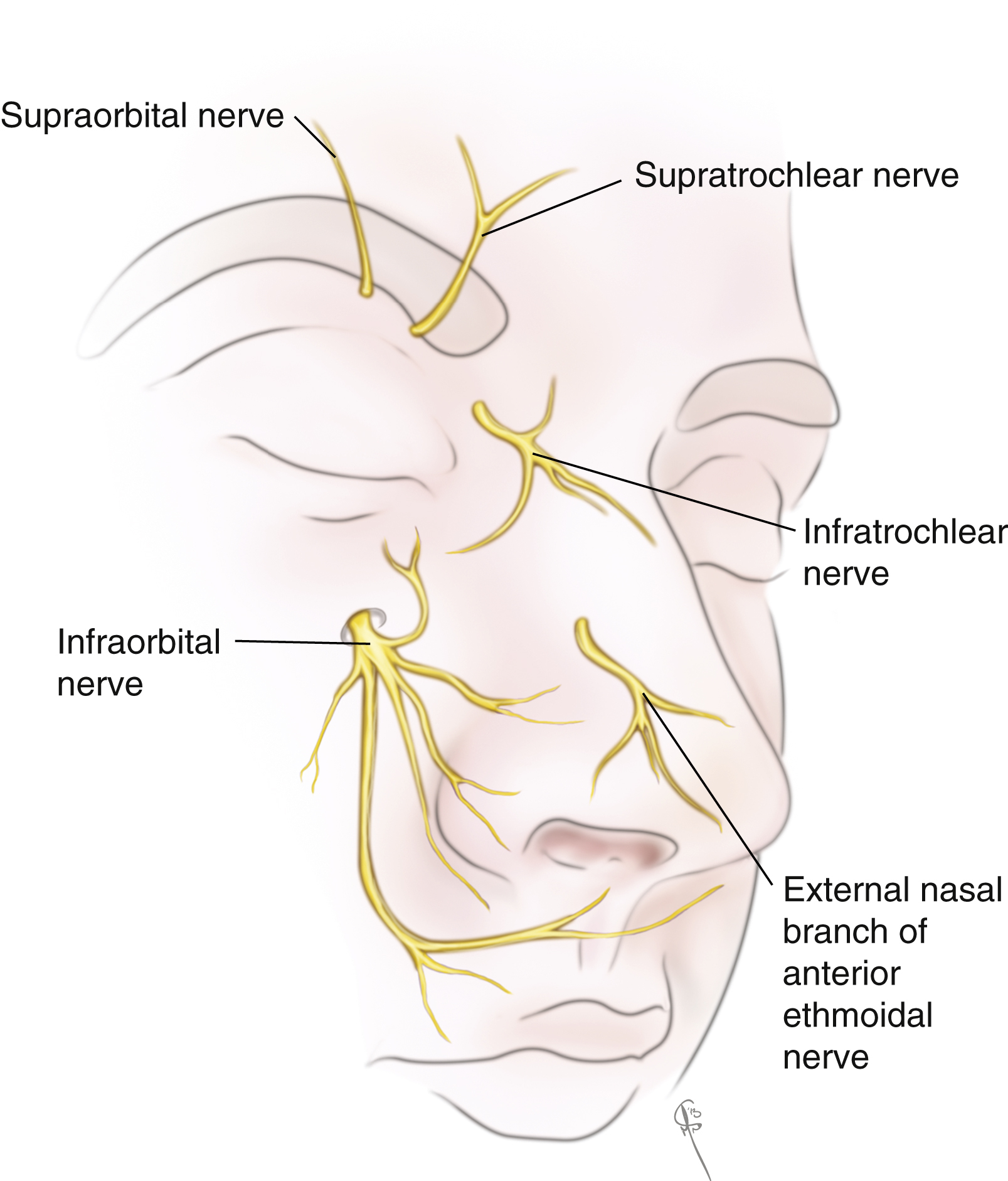
Branches of the second and third divisions of the trigeminal nerves provide sensory innervation of the nose while motor innervation is supplied by the zygomatic branch of the facial nerve. From V 2 , the ophthalmic nerve gives off the supratrochlear and infratrochlear nerves to supply sensation to the rhinion, radix sidewalls. The anterior ethmoid nerve gives off external branches that travel within the SMAS layer to supply sensation to the tip; therefore, careful dissection beneath the SMAS over the tip will preserve tip sensation. From V 3 , the maxillary nerve branches and supplies sensation to the lateral vestibule and columella ( Fig. 68.4 ).
Patient Assessment
The process of rhinoplasty begins with patient evaluation. Arguably, the foundation of a successful rhinoplasty is established at the initial patient visit including a thorough, accurate evaluation of the nose; its relation to the rest of the patient’s face; identification of appropriate and realistic goals given the patient’s anatomy; clear communication; and mutual understanding and agreement of surgical goals between the patient and the surgeon. A vital part of any successful rhinoplasty is the detection of the functional abnormalities. This begins with keen observation of mouth breathing, which often is unbeknown to the patients, and ends with circumspect examination of the internal and external nasal valves, septal deviation, and enlargement of the turbinates. Meticulous preoperative photodocumentation is crucial and life-size based planning or computer generated images of potential postoperative goals may be helpful in facilitating patient–surgeon discussion and establishing matching and achievable operative goals.
History
Important components of a complete history include medical, surgical, family, and social history as well as thorough review of all prescription and nonprescription medications. Of particular interest is whether there has been any previous nasal trauma or surgery. A history of diabetes, connective tissue disease, anticoagulation, or a bleeding or clotting disorder should be noted. Smoking significantly impedes healing and can lead to scarring, skin necrosis, and a poor outcome. A psychiatric history may help the surgeon understand a patient’s motivation for cosmetic surgery. If a patient’s motives are self-driven rather than driven by pressure from peers or a significant other, the patient is more likely to be satisfied with the ultimate surgical outcome. In addition to motivation, it is important to elicit a clear picture of the patient’s desires and expectations from rhinoplasty. This should be considered in the surgeon’s nasal analysis and proposal of surgical goals and limitations with thorough counselling and establishment of reasonable goals. History of sinus infections, sinus headaches or migraine headaches should be documented in depth.
Physical Examination
Physical exam should include a thorough facial analysis characterizing the nasal structures themselves and their relationship to the face as a whole. A careful intranasal exam should also be performed, including inspection of the septum, turbinates, nasal valves, and an assessment of nasal breathing. Finger palpation is an essential component of the exam.
Only in idealized drawings is the face completely symmetric, and strict symmetry of the nose and the face should not be anticipated. The nose should occupy the middle third of the face horizontally and the middle fifth of the face vertically. The nose itself may be divided into thirds vertically. Generally, the upper third is comprised of the nasal bones, the middle third is comprised of the upper lateral cartilages, and the lower third is comprised of the tip and the lower lateral cartilages. Deviations from the ideal should be accurately localized and surgical correction of these variations should address the appropriate structures.
An important feature is the smooth, unbroken, and symmetric brow-tip esthetic line, which is described as a “gentle sweeping line from the medial brow to the lateral nasal wall to the tip-defining point;” the ideal shape of this esthetic line in a female nose is that of an hourglass, narrowing in the middle and flaring at the top and bottom.
Numerous proportions and relationships have been described to characterize the ideal nose. In the frontal view, the ideal nasal length is two-thirds that of the midface, measured from the glabella to the alar base, and equal to the vertical length of the chin, measured from the stomion to the menton. The width of the alar base should approximate the intercanthal distance and may be up to but not more than 2 mm wider, so long as the intercanthal distance is normal. The radix should be at the level of the supratarsal crease.
In the lateral view, the nasofrontal angle should be approximately 115–130 degrees and the radix should be 4–6 mm deep. In females, the dorsum should extend as a straight line until reaching the supratip break, which esthetically separates the dorsum from the tip unit. Ideally, the nasolabial angle should be 93–98 degrees for men and 95–100 degrees for women, although this angle varies somewhat based on the height of the patient. In general, shorter individuals may have a more obtuse angle while taller individuals may have a more acute angle. In the lateral view, the alar base should be 2 mm above the line between the lower and middle third of the nose. The lateral tip projection can be measured from the alar–cheek junction to the tip-defining point.
The alar–columellar relationship should be carefully evaluated from the lateral view. When viewed from this aspect, the upper border of the nostril is formed by the alar rim and the lower border is formed by the columellar rim. Gunter described a method of analysing this relationship. A line is drawn which approximates the long axis of the nostril: the ala should be 1–2 mm above this line and the columella 1–2 mm below this line. If the columellar rim is less than 1–2 mm from this line, the columella is considered to be retracted; conversely, if the distance is greater than 1–2 mm, the columella is considered to be “hanging.” If the ala is less than 1–2 mm from this axis, it is considered to be a hanging ala; if it is greater than 1–2 mm from this axis it is considered a retracted ala. ,
The alar–columellar relationship and alar rim deformities should also include analysis from the alar base view. The ideal base view is an equilateral triangle with each ala forming the sides of the triangle and the alar base width forming the remaining side. A concave ala is present when the lateral border of the ala is medial to the line of the equilateral triangle whereas when it extends lateral to the line of the triangle, it should be considered convex.
The ideal nostril is oval-shaped, wider than the columella, and should be almost parallel to the vertical axis of the columella in the Caucasian nose. The length of the columella should be twice the height of the infratip lobule. The alae should insert at a soft angle to the cheek with a slight curve medially. Disharmonies of the alar base can be in either the vertical or horizontal plane, and careful analysis is critical, as surgical correction of these deformities differ depending on the nature of the deformity.
The relationship of the nose to surrounding facial structures affects the perception of nasal features. A sloping forehead may give the illusion of overprojection of the nasal tip whereas a flattened forehead may give the illusion of an underprojected nasal tip. Similarly, an underprojected chin may make the nose appear relatively overprojected and vice versa.
The esthetics of the nasal tip may be defined by a number of relationships, many of which are quite subtle. The angle at which the lateral and medial crura of the lower lateral cartilages meet should be about 30 degrees on either side. The ideal nasal tip should be well defined. Subtle variations in anatomy may make it appear boxy or bulbous. Wide lateral crura may blunt dome definition, resulting in a boxy tip. A greater than 30-degree angle between the lateral and medial crura or divergent domes can result in a bulbous-appearing tip.
Physical examination should include palpation of the bony and cartilaginous components of the nasal dorsum to understand the relationships between them. The tip recoil test is performed by placing gentle pressure on the tip to assess the strength of the lower lateral cartilages. An intranasal exam should be performed to identify deviations of the nasal septum, turbinate hypertrophy, and any internal causes of nasal obstruction. The Cottle or modified Cottle maneuver is performed to assess nasal valve collapse.
Although the most thoroughly studied and well-described ideal nasal esthetics pertain to the Caucasian nose, much individual variety exists and these ideals cannot be indiscriminately applied to all noses, particularly in different ethnicities such as the African, Asian, Middle Eastern or Hispanic noses.
The African nose has a wide base and low, flattened-appearing dorsum. The ascending maxillary process often lacks vertical projection, which contributes to the low dorsum. The nasal bones are short. Increased distance at alar insertion and alar flaring both contribute to the increased interalar distance. There also tends to be increased fibro-fatty tissue and thicker sebaceous skin at the tip, both of which contribute to lack of tip and soft tissue triangle definition.
The Asian nose has typical characteristics somewhere in between the Caucasian and African nose. There is typically a low dorsum that begins more caudally. Again, the skin at the tip and supratip region is thicker than the Caucasian nose but not quite to the extent of the African nose. The alar width is slightly wider than the Caucasian nose. Characteristically, in the Asian nose, there is paucity of septal cartilage leading to a less projected tip and occasionally retracted-appearing columella. This should be anticipated in Asian rhinoplasty and consideration of other sources of cartilage grafts should be explored and discussed. There also tends to be weaker lower lateral cartilage.
The Middle Eastern and Indian nose share some characteristics with the Caucasian nose,with similar height of the dorsum. However, they also frequently have overprojection of the dorsum resulting in a high dorsal hump. There is mild alar flaring, and thick skin around the tip region. There is variable skin thickness of tip and alar flaring. Dorsal height also varies between the norms of Caucasian and Asian nose.
Photography
The standard approach to photography for rhinoplasty is to obtain realistic preoperative photography using a digital single lens reflex (SLR) camera. Photos should be taken with a standard blue background with appropriate lighting. Many surgeons will have a dedicated space for photography in their office. Standardization of patient positioning, lighting, and angles should be maintained. This will facilitate the surgeon’s study of the patient’s nasal anatomy and facial harmony for surgical planning. Moreover, it permits accurate pre- and postoperative comparison thereby facilitating the surgeon’s self-assessment and critique allowing continual refinement of surgical technique ( Fig. 68.5 ).

An important aspect of successful photography is the lighting and positioning for rhinoplasty portraits. The simplest lighting setup is a single mounted flash on top of the camera itself; however, this can result in harsh and uneven shadows. There are several established, sophisticated lighting arrangements that have been described. The key light system, developed for portrait photography, positions the main light at a 45-degree angle from the patient, casting a shadow from the nasal tip to the oral commissure. A second fill light is placed at nearly the same angle on the opposite side in a position that it fills the shadow cast from the main light. Then, two backlights are placed behind the patient to separate him/her from the background. The quarter system places two lights equally at 45-degree angles from the patient.
The traditional six standard photographic views taken for rhinoplasty are the frontal anteroposterior (AP), right and left lateral, right and left oblique, and base view. , A top view is a useful addition that can be used to better characterize and understand deviations in the crooked nose, especially for patients with dorsal deviation. Some surgeons routinely obtain a smiling view. Proper positioning in both frontal and lateral views requires alignment along the Frankfort horizontal plane, defined by a line that connects the top of the tragus to the infraorbital rim; this line should be truly horizontal and parallel to the ground.
Rhinoplasty Dynamics
The nose is a 3-dimensional centerpiece on the face with critical structural and functional roles. There are many variables and dimensions that can be adjusted to alter the esthetic appearance, structural components, and functional role of the nose. There are many tools and maneuvers available to the rhinoplasty surgeon to adjust these numerous variables. While each adjustment may have a primary anticipated effect, such as increasing tip projection or reducing a dorsal hump, it will invariably have consequences, desirable or undesirable, to another variable nasal dimension.
Adjusting the height at the radix or the caudal aspect of the dorsum will have different effects on a number of facial dimensions. Lowering the radix will frequently result in the appearance of increased intercanthal distance and increased nasal length. Augmenting the dorsum at the radix will appear to reduce the intercanthal distance and shorten the nose. In contrast, reducing the height of the dorsum more caudally can have the opposite effect, giving the nose a shorter appearance and the illusion of greater cephalic rotation of the tip. Similarly, reduction of the caudal dorsum will cause the intercanthal distance to appear wider, while augmenting the dorsum will cause the intercanthal distance to appear more narrow. Reducing the caudal dorsum may also reduce the tip projection as the caudal septum has an important role in supporting tip projection. Osteotomies can result in a narrower-appearing nose and intercanthal distance.
Numerous procedures may be used to adjust tip projection and width; however, not every procedure is appropriate for every patient. For example, an overprojected tip can be reduced with a cephalic trim of the lower lateral cartilages only if the cephalic portions of the lower lateral cartilages are actually the highest projecting part of the caudal tip. If this is not the case, securing the footplate of the medial crura to the caudal septum can decrease or increase tip projection depending on the location on the septum to which they are secured. Reducing tip projection may result in the appearance of a relatively widened alar base and bowed columella. A number of maneuvers are frequently used to both increase tip projection and increase the angle of cephalic tip rotation. Placement of a columellar strut, anchoring the medial crura to the caudal septum, approximating the medial crura foot plates, and advancing the nasal spine can all result in the appearance of increased cephalic rotation and projection. Advancing the nasal spine may also shorten the upper lip. Care must be taken to choose the appropriate procedure for the anatomical constraints presented by each patient.
The astute nasal surgeon will be aware of these effects in planning for rhinoplasty to anticipate the most appropriate and effective maneuvers for a specific patient’s anatomy, during surgery to make adjustments when needed, and postoperatively to assess the results of their adjustments.
Operative Approach
For several decades, surgeons have debated the merits of “open” or the “external approach” versus endonasal rhinoplasty. In the USA, most rhinoplasty was performed endonasally in the latter decades of the 20th century, whereas today, open approach rhinoplasty is the technique of choice for most patients by the majority of rhinoplasty surgeons including the authors, who reserve the endonasal approach for certain patients needing only minor revisions One cannot definitively say that one approach is better than the other for all surgeons, as good results can be achieved by some surgeons using one method whereas equally good results can be achieved by others using the other technique. Some criticize external approach rhinoplasty with the assertion that by opening the skin–soft tissue envelope, some of the strength and support of the tip are lost when the soft tissue attachments are separated from the cartilaginous support. Proponents of the external approach feel there is better visualization and understanding of the anatomy, especially for the novice rhinoplasty surgeon and in the teaching setting. Cartilages are observed in their natural anatomical position and can thus be manipulated “in situ” as opposed to delivering them to make changes. Endonasal rhinoplasty may be more suitable for noses that may require a limited cephalic trim but otherwise have a well-defined tip and symmetric base requiring minimal if any intervention in these areas.
While the primary difference between the two approaches appears to be the midcolumellar incision which connects the bilateral marginal incisions also used in the endonasal approach, we believe that the more important difference is the ability to directly visualize the underlying structures and their relationships to one another in their resting position. Indeed, most of the trimming, suture, and grafting techniques performed are more easily performed with the exposure provided by the external approach.
Endonasal Rhinoplasty
A very brief discussion of endonasal rhinoplasty is warranted, although not our preferred approach. Endonasal rhinoplasty is performed using one of several incisions: a marginal incision (at the lower border of the lower lateral cartilage), an intercartilaginous incision (between the upper and lower lateral cartilages), a transcartilaginous incision, or a rim incision (largely abandoned because of predictable alar notching). To modify the nasal tip with the endonasal technique, the lower lateral cartilages are typically brought out of the nostrils, or “delivered.” The bilateral marginal and intercartilaginous incisions allow the development of bipedicled chondromucosal flaps consisting of the lower lateral cartilages and the underlying mucosa. The cartilages are delivered through the nostril from which they came or can be delivered through a single nostril and then modified as required. The main drawback of cartilage delivery with the endonasal approach is that it requires retraction of the lower lateral cartilages from their normal anatomic position; adjustments are then made with the cartilages out of their normal resting positions.
The plane of dissection is similar to that of the external approach: above the perichondrium and periosteum of the nasal cartilages and bones. Concurrent septoplasty is well described and routinely performed with good outcome, although it is performed through a hemitransfixion incision or a Killian incision as opposed to from above. Dorsal hump reduction can be achieved using an osteotome or rasps, albeit with less direct visual control to make fine adjustments compared to the external approach.
Many surgeons feel that a primary limitation of the endonasal technique when combined with septoplasty is if there is deviation of the L-strut requiring stabilization with spreader grafts, as this can be difficult to accomplish. Many surgeons also feel that the endonasal technique is more limited in its ability to allow adjustments of the alar rim, base and tip; however, the cartilage delivery technique of endonasal rhinoplasty can provide access to perform cephalic trim of the lower lateral crura as well as a variety of dome sutures.
External Approach (Open) Rhinoplasty
Although every rhinoplasty operation should be individualized to each patient’s particular anatomic indications, a systematic order and algorithm may be helpful in operative planning as well as establishing a logical progression of steps and maintaining stability. Local anesthesia using lidocaine with epinephrine should be carefully but judiciously infiltrated into all of the areas of the nose to be dissected, but not adding so much volume that the features and subtle nuances of anatomy are masked. We prefer the administration of 1 in 200,000 epinephrine solution in lidocaine to minimize the systemic effects of the epinephrine followed after 5 minutes with 1 in 100,000 epinephrine solution to maximize the local vasoconstriction. Between the injections we also place Oxymetazoline-soaked packings inside the nostrils and around the septum to boost the effects of epinephrine.
Numerous variations of the columellar incision exist. The authors use a midcolumellar stair-step incision while other surgeons might prefer an inverted-V or 5-cornered incision which is connected with bilateral marginal incisions placed at the caudal border of the lower lateral cartilages. Care is taken not to violate the soft tissue triangles. Dissection of the skin–soft tissue envelope is performed in the subperichondrial avascular plane directly over the cartilage of the lower lateral cartilages, then the upper lateral cartilages; keeping the dissection in this plane will allow the surgeon to avoid the neurovascular structures near the nasal tip. The dissection is then continued cephalically to the caudal aspect of the nasal bones at which point a periosteal elevator is used to elevate the periosteum of the nasal bones in the nasion region.
As previously noted, each operation should be individualized to address each patient’s anatomy. As required, the radix is addressed first, either by reducing it with a guarded bur if it is overprojected or by placing radix grafts if it is underprojected.
Next, the bony and cartilaginous dorsum is addressed. Preoperative evaluation of the dorsum should have identified whether there is an excess or deficiency of the dorsum. The skin is thinnest at the rhinion or bony-cartilaginous junction and becomes thicker cephalically towards the radix and caudally towards the nasal tip. Therefore, a slight prominence should exist at the upper portion of the upper lateral cartilage in order to compensate for the thinner skin to create a straight profile. Any cartilage or bony hump in excess of this should be removed.
The upper lateral cartilages are released from the septum, preserving the underlying mucoperichondrium thereby minimizing chances of postoperative internal valve narrowing. Any significant prominence of the cartilaginous and bony dorsum is addressed together using sharp dissection and an osteotome or a rasp. For a larger dorsal hump, a Rubin osteotome may be used to reduce the bony hump en bloc. , The bony dorsum can be further reduced or smoothed with rasping. Precise cartilage reduction can be achieved by removing consecutive thin slices with a 15 blade until reaching the desired profile. After dorsal hump reduction, the patient may be left with an “open roof deformity” where the lateral nasal bones and upper lateral cartilages are no longer touching the septum. This deformity is corrected later in the procedure with osteotomies and spreader grafts. When the dorsum is deficient, grafts can be placed to create a pleasing esthetic.
If there is significant septal deviation, the septum is addressed at this time either from the dorsal/open approach or intranasally through a hemitransfixion or Killian incision. Also at this time, if cartilage grafting is anticipated, septal cartilage can be harvested. As the old adage wisely professes: “Where the septum goes so goes the nose …”. Several indications exist for septoplasty in septorhinoplasty: obstructed nasal breathing associated with septal deviation, dorsal deviation associated with deviation of the anterior septum, and for harvest of graft material for other aspects of the rhinoplasty.
When septoplasty is performed from the dorsal approach, the anterior septal angle is identified: the lower lateral cartilages are retracted laterally and downward and the septum is identified caudal to its attachment to the upper lateral cartilage. The perichondrial envelope is dissected from the septal cartilage in the subperichondrial plane and if not already performed or as dissection proceeds, the upper lateral cartilages are released from the septum to provide adequate visualization of the more posterior septum. Preservation of the mucoperichondrium provides support and ultimately reduces internal valve collapse.
Once the septal cartilage and bone is exposed, it is assessed to determine which portion of the septal cartilage must be resected or weakened in order to relieve the deviation. One should also consider how much cartilage grafting material should be harvested. An important principle guiding septoplasty or septorhinoplasty is to maintain the structurally supportive “L-strut” comprised of dorsal and caudal septum. We recommend leaving at least a 1.5 cm, preferably 2–2.5 cm, dorsal strut to maximize the degree of support. If significant deviation exists in the L-strut, this may be corrected and stabilized with unilateral or bilateral spreader grafts or septal rotations suture (an effectively placed horizontal mattress suture (e.g., 4-0 PDS) may correct mild deviations of the L-strut). Gruber et al demonstrated that a 10-mm wide, 0.5-mm thick piece of cartilage with a curvature may be adequately straightened with a horizontal mattress suture placed with an 8-mm longitudinal spacing with the knot on the convex side.
If there is a spur or deviation involving the bony septum either superiorly in the perpendicular plate of the ethmoid or posteriorly in the vomer, these may be addressed by resecting the deviated portions. Caution should be exercised during resection of the perpendicular plate, avoiding rocking motions, as cerebrospinal fluid (CSF) leak may occur as a rare complication of septorhinoplasty.
If the inferior edge of the caudal L-strut has been released from the maxillary crest, it can be repositioned in the midline and sutured to the maxillary crest periosteum to secure it. Alternatively a piece of cartilage may be secured with a permanent suture as bridge between the caudal septum and the nasal spine if there is not enough length for adequate projection.
If the septorhinoplasty is being performed to improve nasal airway obstruction, inferior turbinate hypertrophy should be addressed with submucosal resection, inferior turbinate outfracture, and/or conservative resection of the hypertrophic portions of the turbinate, being careful not to be overzealous, possibly causing atrophic rhinitis or empty nose syndrome.
Once satisfactory dorsal projection is achieved, osteotomies are planned and executed as necessary. Osteotomies are performed to narrow the bony dorsum, to close an open roof deformity created by dorsal hump reduction, or to straighten a crooked bony dorsum. Recalling anatomic considerations, the ideal width of the bony dorsum is about two-thirds that of the alar base width. The nasal bones and ascending maxilla tend to be thicker cephalically; therefore, planning osteotomies higher may help to minimize the narrowing effect on the internal nasal valve and nasal breathing. However, if the osteotomy is carried too high or if the medial and lateral osteotomies do not meet, a rocker deformity may result. Another anatomical consideration in osteotomy is the patient age: younger patients tend to have more flexible bone while older patients have more brittle and easily fractured bone. Interrupted “postage stamp style” osteotomies in younger patients may be less effective if they result in greenstick fracture and their nasal bones spring back into place.
It is important to perform effective injection of local anesthetic containing epinephrine prior to the osteotomies in order to minimize bleeding and postoperative swelling. The periosteum of the nasal bones is elevated medially while the lateral periosteum is left attached to bone in order to provide stability to the segment of bone after lateral osteotomy during the healing period. If significant hump reduction has been performed, a formal medial osteotomy may be unnecessary.
In general, medial osteotomies should be performed first, followed by vertical osteotomies, then the lateral osteotomies, in order to maintain stability of the remaining lateral portions of the nasal bones for each succeeding osteotomy. Medial osteotomies are usually performed intranasally by seating the osteotome between the septum and the upper lateral cartilage at the caudal edge of the nasal bone. Since the upper lateral cartilages obtain their structural support from their connection to the underside of the nasal bones, this relationship must not be interrupted if narrowing of the bony dorsum is part of the preoperative plan, a second medial osteotomy is performed to remove the excess bone as a wedge. Medial osteotomy is followed with vertical (anteroposterior) osteotomy at the level of the medial canthal ligament (the deepest part of frontonasal suture laterally) to connect the lateral osteotomy with medial osteotomy and mobilize the bony segment. Vertical osteotomies should be performed below the level of the canthus to minimize risk of lacrimal system injury, and if performed correctly can provide more precise control of nasal bone positioning.
The lateral osteotomy is performed in a continuous fashion in a caudal to cephalic direction through nostril incisions and using a guarded osteotome. With this approach, the inferior limit of the lateral osteotomy should be just above the level of the inferior turbinate insertion in the ascending process of the maxilla and care must be taken to preserve the bony triangle at the level of the piriform aperture at the caudal aspect of the maxillary bone. Staying above the inferior turbinate, as in a high-to-low osteotomy will minimize risk of nasal airway compromise and address a wide bony base at the same time, the alternative way is to infracture the inferior turbinate to minimize the chance of airway compromise.
Tip and Lower Lateral Cartilages
The ideal nasal tip should be well projected, supported, not over- or underrotated, and well defined without being bulbous or have skin that is so tightly pulled over the cartilage that the tip appears bifid. Appropriate tip projection may vary in different ethnicities. This should be considered in ethnic rhinoplasty as overprojection may result in racial incongruity , and disharmony with the rest of the patient’s face.
Various cartilaginous trimming, grafting, and suture techniques may achieve nasal tip definition and correct mild tip deviations. Conservative trimming of the lateral crus may be performed to even out asymmetries. It is imperative to leave a minimum of 6 mm strip of the lateral crus to preserve enough strength to prevent buckling.
The domes should about 4.5 mm wide and the width of overall tip should be around 8–11 mm, with the average being 9 mm. The thicker the soft tissues of the tip, the narrower the tip should be. A lateral crural mattress suture may be used to strengthen the lateral crus or to straighten convexities of the ala, either after overresection or in the setting of weak cartilage. For the lower lateral cartilage, typically about 6 mm wide and 0.5 mm thick, a mattress suture may be placed with 6 mm spacing between the two loops of the stitch. Multiple stitches may be placed along the length of the lower lateral cartilage for added strength. The same concept may be used to provide a subtle increase in strength for the columella. A columellar–septal suture strengthens the columella when only a mild weakness is present that does not require grafting.
Dome stitches may be used to not only create more definition of the nasal tip but also to correct mild deviations or asymmetries by bringing together divergent intermediate crura. If there is any chance of knots protruding into the skin, absorbable monofilament PDS is preferred. If sutures are placed deep in a location with no risk of extrusion or visibility, nylon is also a viable option. A hemitransdomal stitch is placed through the vestibular skin and traverses the most cephalic end of the dome and attempts to evert the lateral crus. A transdomal suture is a horizontal mattress suture that brings together the medial and lateral crura of one of the lower lateral cartilage. When placing this stitch, care must be taken to avoid causing the lateral crus to invert as it may result in concavity of the ala. Also, if the lateral bite of the stitch is not placed laterally enough, it may result in counterrotation and decrease in projection. A transdomal stitch placed appropriately laterally should increase tip rotation, projection, and definition. An interdomal stitch approximates the medial crura together and is set back from the tip several millimeters.
In profile the domes should rise about 6 mm beyond the dorsum. This projection should be increased to 8 mm or even more on noses with thick skin. As previously described, in the ideal profile view of the nose, the ala sits 1–2 mm above the long axis of the nostril and the columella 1–2 mm below it. It is vital to identify the correct anatomical problem: when a hanging ala is present, this should be correctly distinguished from retracted columella so that the appropriate problem is addressed. If a mild alar retraction exists (<2 mm from the long axis of the nostril), an alar rim graft will not only correct this deformity, it will also correct the concavity commonly associated with the retraction. On noses with wide bases and mild alar retraction, a small wedge of alar skin may be resected and the remaining ala repositioned inferiorly. If greater than 2 mm of retraction exists, a V–Y advancement, a composite graft, or an intercartilagenous graft may be required between the upper and lower lateral cartilages on that side. These maneuvers can lower the ala 4–8 mm. A hanging ala may be corrected by excising a small wedge of vestibular skin intranasally or by resecting a strip of cartilage at the caudal edge of the lateral crus of the lower lateral cartilage. A hanging columella can be corrected by resecting a thin strip of the caudal cartilaginous septum or by securing the medial crura to the caudal septum in a tongue-in-groove configuration. . Columellar retraction can be addressed by columellar strut or septal extension grafting.
The base view of the nose should approximate an equilateral triangle. If there is convex ala protruding from the triangle, debulking of soft tissue, trimming lateral crura, or placing dome-spanning sutures may correct this. Concave ala may be corrected by alar rim or strut grafting with cartilaginous grafts on top of or deep to the lateral crus respectively, depending on the severity of the concavity.
Grafts
Autologous graft material is preferable to alloplastic implants, as the latter is significantly more prone to infection and extrusion. Common choices of graft material include septal cartilage, conchal cartilage, rib cartilage, and temporalis fascia. Cadaveric irradiated cartilage and alloplastic materials such as Medpore, silicone, and Gortex are used by some surgeons. For most primary rhinoplasties, septal cartilage is preferred and has several advantages: it is readily accessible and in the same operative field, abundant (in patients who have not undergone septoplasty), and strong, which is ideal for supportive grafts. Auricular conchal cartilage can be harvested without additional prep if its use is anticipated and the ear is prepped into the operative field. Some surgeons prefer a preauricular incision whereas others prefer a postauricular incision for graft harvest. A significant amount of cartilage may be harvested without compromising the structural or esthetic appearance of the ear as long as a few millimeters of rim is left in place along the conchal wall. Conchal cartilage is curved and significantly weaker than septal cartilage thus making it less suited for supportive strut grafts and better for alar reconstruction. Potential donor site morbidity includes auricular hematoma or perichondritis, although their risk can be minimized by the use of antibiotics and a bolster dressing.
Rib cartilage may be necessary for significant nasal reconstructive procedures. The rib provides an abundant source of graft material but it carries the minor disadvantage of requiring a second harvest site and potentially causing a pneumothorax. The most common source of costal cartilage for grafting in females is the sixth and seventh rib cartilages, as the incision can be hidden in the inframammary crease. Costal cartilage carries the risk of warping once it is in place. The effect of warping can be minimized by keeping the cartilage in saline for 30–60 minutes after harvest, determining in which direction twist will occur, and anticipating warp when carving the cartilage. A warping prevention suture described by us could be used to minimize the potential for a revision surgery. After deciphering the direction of the warping following placing the cartilage in saline solution, a 4-0 or 5-0 PDS suture is passed back and forth on the convex side of the cartilage from one end to the other end and tied tight enough to straighten the warped cartilage. This suture negates the need for the use of Kirschner-wire (K-wire). Perichondrium, native fascia or temporal–parietal fascia harvested from the patient can be laid over cartilage grafts to camouflage irregularities. Multiple layers of fascia can be laid on top of each other with each layer of fascia resulting in 0.5 mm of augmentation although additional layers of fascia may prolong postoperative swelling. For bulk, any of the above cartilages can be diced and wrapped in fascia. These fascia-wrapped cartilage grafts can add volume in areas such as the dorsum but have little utility as supportive grafts. We prefer placement of diced cartilage using a 1-mL insulin syringe in an ideally prepared pocket without fascia. Alloplastic material such as Medpore, a high-density polyethylene, is theoretically biocompatible and intentionally placed pores allow fibrovascular ingrowth which serves to prevent graft migration. However, the risks of extrusion and infection and the fact that it is often difficult to remove because of the fibrovascular ingrowth make it less ideal than autologous graft materials.
Spreader Grafts
Spreader grafts may be indicated when there is midvault nasal obstruction to widen the internal nasal valve, to augment an overly narrow dorsum, to support a deviated L-strut, to fill a defect from dorsal hump reduction, or when there is an inverted-V deformity. We believe that any time a large enough hump is removed to create an open roof the use of spreader grafts becomes mandatory, otherwise an inverted-V deformity will ensue months or years later. The ideal material for a spreader graft is septal cartilage. Costal cartilage, layered or folded conchal cartilage, or the medial edge of the upper lateral cartilages (spreader flap) may also be used. Typically the cartilage is cut into strips approximately 5 mm high and 30 mm long, spanning the cartilaginous dorsum. If there is a curve in the graft cartilage, it can be scored and oriented so that the two pieces counteract the other’s curve. The graft is secured with at least two mattress sutures. The mattress sutures each traverse five layers securing both pieces to the septum medially and the upper lateral cartilages laterally.
Supportive Grafts
The columellar strut graft is the most commonly used graft. The ideal material for a columellar strut is septal cartilage. It can be placed to help support the tip and overcome ptosis and overrotation of the tip. The medial crura of the LLC can be secured to the graft to prevent hanging columella.
For dorsal augmentation and increased tip projection with adequate support, onlay grafting may be performed. Adequate healthy skin must be present at the tip, as this graft may stretch the skin increasing the risk of skin necrosis. The ideal graft material is either septal cartilage or a straight segment of rib.
A lateral crural strut graft can be placed to correct a prior concavity of the base view of the ala or to counteract the effect of dome sutures that may lead to concavity. A pocket is dissected on the deep surface of the lateral crus of the LLC beneath the vestibular skin intranasally. The graft cartilage is placed in the pocket and secured to the lateral crura using mattress sutures.
Alar rim grafts, fashioned from septal or costal cartilage, may be used to support the nasal valve or cosmetic purpose, it is ideally placed in a pocket at the lowest part of the alar rim. Cephalic placement on the lower lateral cartilage will stent open the internal nasal valve while caudal placement on the lower lateral cartilage will stent open the external nasal valve. Once the appropriate placement is done, the graft is secured with a suture that will be used to repair the rim incision.
The ideal alar rim smoothly transitions from the tip-defining point to the nasofacial insertion, the contour and strength of which are determined by the lateral crus of the LLC. The LLC is in a position close to the rim more medially but laterally is in a more cephalic position as it moves away from the alar margin: this lack of rigid support can lead to scarring, retraction, and/or unpredictable asymmetry. The alar rim graft, placed along the alar margin, is a powerful graft capable of directly altering the contour and strength of the alar margin. Indications include correction of alar flare, cephalic malposition and inadequate alar support, and correction of dynamic margin collapse. On patients with cephalically oriented LLC, the lateral crura are dissected and transposed caudally.
Several types of tip grafts can be used to create a more defined-appearing tip and/or to achieve slight increase in projection of the nasal tip. A shield or onlay graft is cut or prepared using the tip punch device designed by our group and placed as an onlay graft on top of the LLC or as a shield graft. A tip graft is created from a horizontal piece of cartilage that crosses both domes with beveled edges laterally. The tip graft can be used to correct minor tip asymmetries. An infralobular graft can be attached to the septal cartilage in order to increase columellar show in noses with a retracted columella. After placement of a columellar strut, an onlay to the nasal tip is supported by the columellar strut and overlies both domes. A subdomal graft can be used to correct a pinched dome appearance or set the distance between the domes. The subdomal graft is placed after dissecting a tunnel under the domes and secured with 6-0 Vicryl suture; septum is the ideal location for donor site and graft is around 1×1×8 mm.
Alar Base Adjustments
Alar adjustments should be reserved for the last step after all the tip refinement and supportive grafts have been completed. An overprojected nasal tip or hypoplastic maxilla may give the illusion of narrowed alar width. Similarly an underprojected tip or protruding maxilla may give the illusion of widened alar width. These issues must be ruled out before considering adjusting the alar base positions. Ala that are displaced cephalically can be repositioned by resecting an ellipse of skin around the alar base and repositioning the ala medially; this will bring it to a more medial and caudal position. Wedge excisions according to the appropriate abnormality can remove part of nasal sill, ala, or both. V–Y advancement and inverted-T excision for wide and thick alae are other maneuvers that can be useful in certain patients.
Final Steps
Typically, if septoplasty has been performed and there is a mucosal incision, it is closed with interrupted 5-0 chromic sutures and intranasal Silastic or Doyle splints are placed. Some surgeons prefer quilting sutures to reapproximate the apposing mucoperichondrial flaps in the absence of the removed septal cartilage. The columellar incision is closed with interrupted 6-0 fast-absorbing catgut sutures. Marginal incisions are closed with interrupted 6-0 fast-absorbing catgut sutures.
The dorsum is taped with Steri-Strips (3M). If osteotomies were performed, the dorsum is splinted with a Denver Splint or a thermoplastic splint. If a rib graft has been used for dorsal grafts, it may have been secured in place with K-wires: these are pulled through the splint and secured in place until they are removed 2–3 weeks postoperatively.
Postoperative Care
Postoperative care varies among surgeons. Patients are counseled about the potential for postoperative bleeding, which can be self-limited and treated with oxymetazoline spray. In the immediate postoperative period (24–48 hours), patients should to keep their head elevated to minimize swelling. Patients should avoid exercise or strenuous activity for 2–4 weeks postoperatively. Postoperative antibiotic prophylaxis may be considered if intranasal splints have been placed or an ear bolster is used after conchal cartilage harvest. Sutures and splints are removed 1 week postoperatively. Although it is not always necessary or indicated, postoperative steroids have been observed to be effective in decreasing swelling. Perioperative steroids have been shown to decrease periorbital edema in the immediate postoperative period.
Complications
After rhinoplasty, the normal postoperative course has some expected inconveniences that the patient should be made aware of preoperatively and should not be considered as complications. Pain, bruising, and postoperative swelling are to be expected. If the swelling is excessive or prolonged, postoperative oral steroids may help to speed resolution. Taping the nose may be helpful in decreasing swelling and may be continued by the patient on a nightly basis even weeks after surgery. Gryskiewicz et al feel that after 14 days, Kenalog injections may be considered every 2–4 weeks for up to six injections.
Intraoperative complications should be identified and addressed prior to completion of surgery. These include excessive bleeding, iatrogenic injury to the nasal skin or underlying cartilages, lack of dorsal support as a result of fracture of the L-strut, septal fracture; inward displacement or collapse of the nasal bones; “rocker deformity;” and cribriform plate fracture. The risk of bleeding can be minimized by counseling the patient to avoid not only anticoagulants and nonsteroidal anti-inflammatory drugs (NSAIDs), but also supplements that may have anticoagulative effects. Bleeding can also be minimized with control of hypertension, topical intranasal vasoconstrictors, adequate preoperative injection of a local anesthetic combined with epinephrine, dissection in the proper plane, and careful but judicious use of bipolar cautery. Hypertension is the most common reason for intraoperative bleeding and should be appropriately controlled by the anesthesiologist. Von Willebrand disease is more common than many realize and patients are treated with desmopressin (DDAVP) or tranexamic acid, also useful in patients who have taken NSAIDs. Obviously, iatrogenic injury to the nasal cartilages or nasal skin should be avoided, but careful repair should be performed if such an injury occurs. The septum can be fractured in about 1% of septorhinoplasty cases. This is more likely to occur if there has been previous septal cartilage harvest or significant dorsal hump reduction, deficient nasal bones or a severely deviated septum. A fractured L-strut can be addressed with suture fixation to spreader grafts and/or by fixation of the strut to the nasal bones. Intraoperative complications associated with osteotomies can be identified immediately after the osteotomies are completed. A collapsed or unstable displaced nasal bone can be suspended from the septum if still attached to the upper lateral cartilages. Sutures, or infrequently, K-wires can be used to stabilize the bones or, one can place a Merocel pack intranasally for 1 week to hold the bone(s) in position. A rocker deformity may occur if the lateral osteotomy is carried too far upward and laterally beyond the radix. With a rocker deformity, inward displacement of the nasal bone will result in outward and lateral displacement of the frontal bone segment. This is corrected by an additional osteotomy in the appropriate position. If a CSF leak is observed, it should be managed immediately. Nasal packing and lumbar drainage may be necessary.
In the immediate postoperative period, complications may include bleeding, erythema related to vascular congestion, infection, skin loss or necrosis, and early patient dissatisfaction. While mild bleeding may be expected after rhinoplasty, excessive postoperative bleeding is rare (0.9%). In cases of troublesome or excessive bleeding, hypertension should be controlled, topical vasoconstrictors should be used, and DDAVP may be infused without the need for additional intervention. Packing should be avoided. Early postoperative erythema may be a sign of vascular congestion (more common in revision cases), contact dermatitis, or early infection. When erythema appears to be of infectious etiology, early initiation of aggressive oral antibiotic treatment is indicated. The skin over the nasal tip is delicate and at risk for necrosis, especially if the patient is a smoker. Its vascular supply can be compromised by excessive soft tissue trimming or cauterization over the ala, which may disrupt the lateral nasal artery, or with grafts that exert too much stretch or tension on the skin.
In the intermediate postoperative period (2 weeks to 2 months), additional complications may be noted such as prolonged edema, delayed healing, patient concern/dissatisfaction, synechiae, osseous overgrowth, septal perforation, anosmia or “late” presentation of a CSF leak. As the initial postoperative swelling subsides, subtle defects or irregularities may be noticed; more obvious abnormalities such as graft migration may be recognized and will likely need to be addressed surgically. Patients may voice concern about the appearance of the nose because they cannot anticipate its final shape. Osseous overgrowths may occur at the site of bony resections or torn perichondrium and can be addressed with conservative rasping in a revision procedure. Septal perforations may occur, more commonly if bilateral septal tears were created and not repaired. Anosmia that continues after splints are removed and expected postoperative swelling has diminished may be the result of cribriform plate injury. Clear rhinorrhea that begins in the later postoperative period can be a late presentation of CSF leakage. CSF leaks are rare after rhinoplasty (1.17%) and usually seal on their own; however, patients with suspected leaks should be counselled to be vigilant in watching for signs of meningitis.
Late complications from rhinoplasty include nasal airway obstruction; various irregularities and deformities; implant exposure, extrusion, or migration; scarring, silent sinus syndrome; enophthalmos; and mucocele formation. Nasal obstruction may result from nasal valve collapse due to overexcision of the lateral crura of the LLC, mid-vault collapse, aggressive medialization of the bony pyramid, or intranasal scarring in the form of synechiae. Saddle nose deformity may result from overresection of the septum or bony dorsum. Open roof deformity results from failure to fill the midline defect created from dorsal hump resection with osteotomies and spreader grafts. Unsightly scarring may occur at the columellar incision with notching. Scarring may also occur at the site of percutaneous osteotomies with hyperpigmentation or tethering of the skin. Ethnic incongruity may occur by inappropriate planning in ethnic rhinoplasty. Autologous implants may become infected, migrate, extrude, or be associated with skin contracture which must be addressed by removal and replacement with an autologous graft, if appropriate.
Secondary and Tertiary Rhinoplasty
It is not uncommon for the rhinoplasty surgeon to be presented with a patient who has had a prior rhinoplasty. It is estimated that between 2% and 30% of rhinoplasties result in secondary rhinoplasty. The preoperative assessment described above for primary rhinoplasty, for the most part, applies in revision rhinoplasty. Of particular importance is the patient’s previous surgical history, the nature of their concerns or dissatisfaction, the patient’s social history and psychiatric history, and of course, a thorough objective evaluation of the patient’s anatomy.
Evaluation
Operative History
It is important to attempt to obtain the operative record of any and all previous nasal surgeries as part of the preoperative evaluation of a patient presenting for revision rhinoplasty. The most common reasons for revision rhinoplasty are underresection or overresection of the structural cartilages. Consequently, eliciting information from the operative record and comparing it with the patient’s physical examination may help the surgeon clarify whether the remaining cartilages need to be trimmed further or reinforced with grafts. Also, the extent of previous septoplasty or septal cartilage removed may help the revision rhinoplasty surgeon anticipate the need for various alternative cartilage grafting sources such as conchal or costal cartilage and whether these sources have previously been used.
Patient Reported Issues
The surgeon needs to have a very clear and specific understanding of the source of the patient’s dissatisfaction. Perhaps even more than with primary rhinoplasty, realistic expectations must be established. If the patient’s expectations are judged to be unrealistic, it should be made clear and documented whether the surgeon believes that their desired results are attainable. A number of patient-reported issues may be unique in the setting of prior surgery. Most of these relate to postoperative complications such as an inappropriately placed graft, graft migration, pain, infection or extrusion of implants, or nasal airflow obstruction secondary to nasal valve collapse from excessive cartilage resection.
Objective Issues
A full examination and facial analysis should be performed. The height, width, and symmetry of the nose should be assessed. The nasofrontal angle location and angulation should be noted. The dorsum should be visually examined and palpated for irregularity. The bony pyramid should be examined noting its width, any asymmetries, and whether there is an inverted-V deformity. The supratip area should be assessed for pollybeak deformity. Adequacy of tip projection and rotation should be assessed. Assessment of the LLC should include evaluation for symmetry, bossae, alar rim collapse, the tip-defining points, width, position, and columellar angle. Intranasal examination can identify valve narrowing or weakness, synechiae, or septal perforation from prior surgery and give the revision surgeon clues as to how much septal cartilage may be available for grafting.
Skin
Skin examination in the patient who has had a previous rhinoplasty is important as it can be thinned or scarred from previous surgery, perhaps more often with external approach or with extensive dissection. Also, previously placed alloplastic graft material may have resulted in scarring. The presence of scarring may increase the risk of skin necrosis and poor outcome. When the skin is extremely thin and scarring seems highly likely, it may be prudent to stage the revision procedure by placing a dermal graft and allowing it to heal prior to performing revision rhinoplasty so that a healthy skin flap can be elevated and redraped with a good chance of healing at the time of surgery.
Structural Support
The full nasal examination and analysis as described above will provide insight about the structural support remaining in the previously operated nose. Often due to prior cartilage removal, there may be a lack of support to the tip and alae that may require grafting.
Operative Principles and Approach
One can argue that for revision rhinoplasty cases, the external approach is particularly advantageous, allowing full examination of the anatomy and assessment of what has been done in the previous surgery unless the revision surgery is minor, which can be done through a closed technique. In revision cases, it is wise to err on the side of minimal resection, as the structural support has already been compromised by prior dissection and resection. Sources of cartilage for grafting should be considered and planned out prior to surgery. When autologous septal cartilage is not available, the authors prefer to utilize other autogenous materials like rib or conchal cartilage.
When possible, the nose should be entered through the previous incision unless it has been poorly designed. This can avoid leaving the patient with an additional scar and allow the surgeon to resect and revise an unsightly scar. Dissection on the cartilage should proceed with caution, anticipating scarring from previous dissection. If a dorsal onlay graft is deemed necessary, the recipient surface should be flattened with a rasp to minimize irregularity. If costal cartilage is used, securing it with K-wire can limit warping and migration. The septum is addressed as described previously. If the L-strut is significantly weakened, it can be reinforced with spreader grafts.
Tip reconstruction is performed, as described for primary rhinoplasty. If supportive grafts are necessary, one should begin by supporting the columella. Grafts can be secured in various ways including by drilling a K-wire into the maxilla just lateral to the maxillary crest and securing the graft to the wire. Occasionally, when there has been excessive resection of the lateral crura, supportive grafts may not be enough and alar replacement is required. Conchal cartilage has a natural curve that mimics the curve of the lower lateral cartilages and is a good choice for this indication. The soft tissue is dissected creating a tissue pocket at the pyriform aperture and the graft is placed in this pocket. An anchor graft may be used in revision cases for alar retraction: conchal cartilage is shaped to look like an upside-down anchor with the sides at each lower lateral cartilage and the middle secured to the septum or a columellar graft. Previous rhinoplasty may create a pinched dome appearance. A dome spreader graft may address this by securing a small piece of cartilage between the medial crura.
Complications
The spectrum of complications that may occur after revision rhinoplasty is essentially the same as that for primary rhinoplasty, although postoperative edema may take longer to resolve and there may be a higher risk of skin necrosis in previously dissected tissue.
References
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


