Chapter 57 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Introduction
Due to the high incidence of anterior cruciate ligament (ACL) ruptures and the tremendous socioeconomic importance of this injury, there continues to be intensive research into basic science, pathology, and reconstruction techniques of the ACL. Thus a wide range of techniques for ACL reconstruction and numerous different fixation devices are available. Nevertheless, the perfect technique for ACL reconstruction still seems to be elusive, demonstrated by the fact that primary ACL reconstruction is not successful in restoring normal knee kinematics in all cases. According to the current literature, revision surgery after primary ACL reconstruction is performed in 3% to 25% of cases due to long-term graft failure as well as unsatisfactory outcome (loss of range of motion, locking, effusion, pain, etc.).1–3
It is generally believed that revision ACL reconstruction is a challenging procedure requiring experience in a variety of different surgical techniques and graft fixation techniques. Revision ACL reconstruction might be even more demanding if surgical mistakes have been made during primary reconstruction, if a double-bundle reconstruction was performed, or if a severe tunnel enlargement has developed. Whether revision ACL reconstruction can be performed as a single- or two-staged procedure mainly depends on tunnel and hardware management.2,4,5
It is generally believed that the overall clinical outcome after revision ACL reconstruction is inferior compared with primary procedures.2,5–13 Thus the importance of counseling the patient preoperatively about less satisfactory results than in primary ACL reconstruction must be emphasized. However, taking an inferior result into account, as described in the current literature, one might be quickly less optimistic about producing an optimal result after revision reconstruction. Therefore it should be our primary goal to be as perfect as possible with diagnostics and decision making as well as surgery in order to offer the patient a successful outcome, as in primary reconstruction. Thus we strongly recommend the use of a clearly defined diagnostic and treatment algorithm in order to fulfill that goal.
Failure Analysis
Radiographic Evaluation
The performed radiographs should routinely include the following:

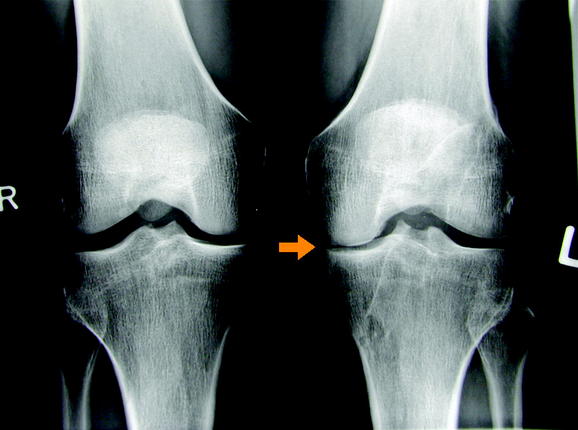
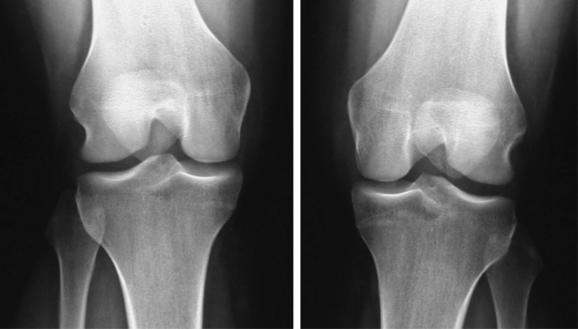
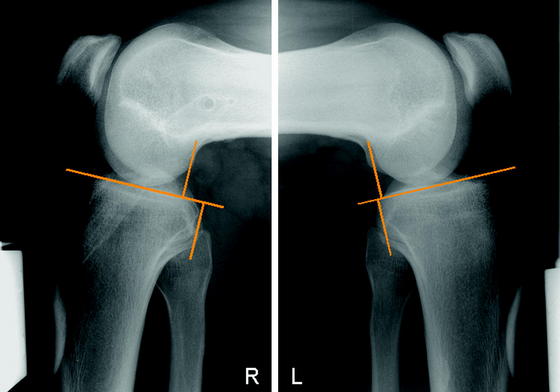
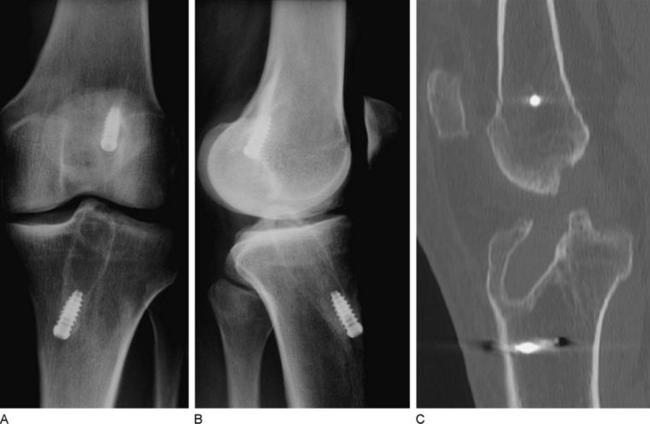
In cases with clinically apparent varus or valgus malalignment or posterolateral insufficiency, long standing radiographs should be made to assess the need for additional axis correction. In case of tunnel enlargement, a computed tomography (CT) scan is indicated to clearly analyze its dimensions (Fig. 57-6).
Concomitant Pathology
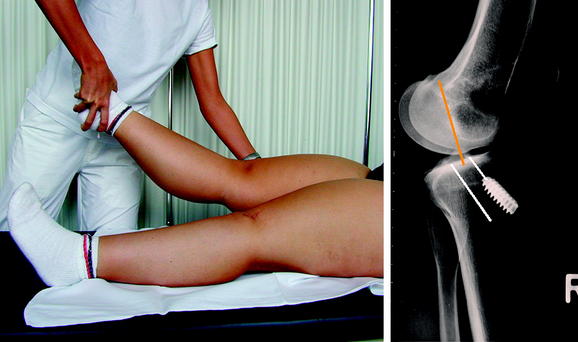
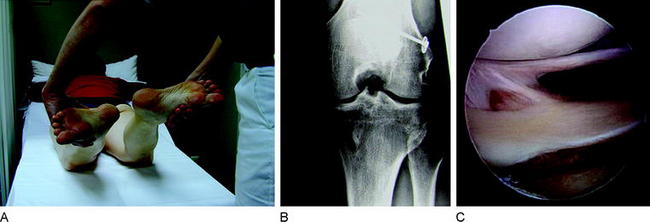
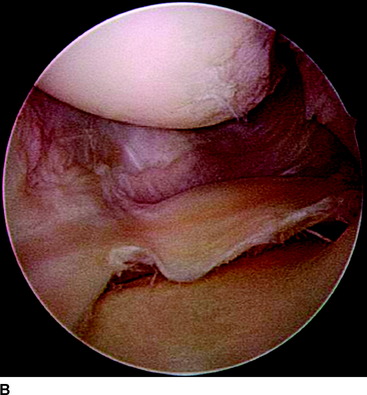
The stabilizing functions of the single knee ligaments are not strictly separated. Secondary graft failure can often be found in combination with unrecognized concomitant ligament pathology, even in perfect ACL reconstructed knees. In fact, all the knee restraints work as a unit and normal knee stability can only be achieved if all ligaments are intact. In cases of ACL insufficiency, secondary restraints such as the posterior oblique ligament (POL) and the posterior horn of the medial meniscus might compensate for the instability. However, if there is medial collateral ligament (MCL) insufficiency (especially POL) and/or a subtotal medial meniscus loss, the freshly reconstructed ACL might not be able to absorb the particular forces and might stretch out. In principle this can be applied to any other combination of ligamentous knee injuries. Thus all directions of knee instability, especially rotatory instabilities, have to be assessed carefully during clinical (and radiological) examination. In detail these instabilities include the PCL (see Fig. 57-5), lateral or posterolateral rotatory instability (PLRI; Fig. 57-7), anteromedial rotatory instability (AMRI), anterolateral rotatory instabilities (ALRI), and MCL or posteromedial rotatory instabilities (PMRI; Fig. 57-8).

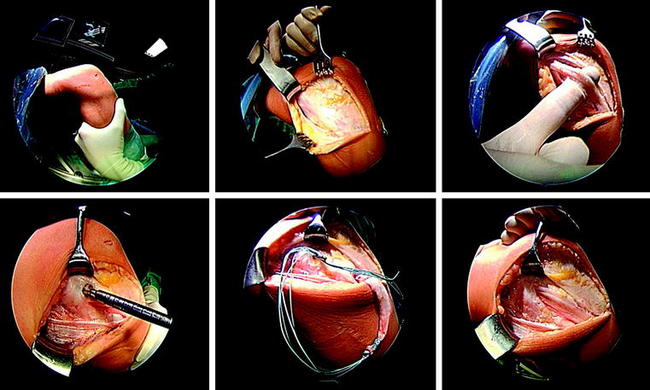
Now we have to question which of these concomitant pathologies needs to be addressed surgically in revision procedures. If an AMRI or PMRI is present, a certain grade of instability might be left untreated in a revision case, as the influence of these instabilities is still not clearly defined and the outcome of surgery (MCL, POL, PMRI) often is unsatisfactory. If there is severe valgus opening, a posteromedial reefing (e.g., that according to Hughston) or a ligament grafting could be done.17,18 Whether a microperforation of the medial structures according to Rosenberg is successful in these conditions needs further clinical research. In cases of lateral instabilities including PLRI and ALRI, the situation is different. In former years a grossly positive pivot shift was often treated by an additional anterolateral stabilization such as according to Lemaire19–21 (Fig. 57-9). At present, an additional extraarticular procedure is not routinely recommended; however, in revision reconstructions one might make an exception. In cases with only a slight anterior translation combined with a gross pivot shift, one might consider an additional anterolateral stabilization in selected cases if the femoral ACL graft position is lateral (10-o’clock position). If, for example, a revision reconstruction with lateral femoral tunnel placement does not restore the pivot shift during revision surgery, one might consider an additional Lemaire procedure in these rare cases. However, only one peripheral concomitant pathology should always be addressed during ACL revision reconstruction, the PLRI (see Fig. 57-7), because the high failure rate of ACL reconstruction in combination with a PLRI is well known.22–24
In principle, single-staged repair of any of these combinations is possible if boundary conditions allow for the planned surgical procedure. One major exception has to be assessed carefully, which is clinically apparent as the “fixed posterior subluxation.” Normally this phenomenon is discussed in the context of PCL insufficiency and repair. However, it has been demonstrated that approximately 15% of all patients with PCL insufficiency underwent previous isolated ACL reconstruction.25 The reason for this failure often is a wrongly interpreted positive Lachman test, which in the case of PCL insufficiency and an intact ACL might demonstrate an increased way with a firm endpoint. Thus it is of great importance to always evaluate the PCL in ACL deficient knees. Additionally, the PCL deficient knee easily subluxates to posterior during ACL graft fixation, which might lead to a fixed posterior subluxation.26 This results in changed femorotibial biomechanics and high patellofemoral reaction forces. Patients who demonstrate a fixed posterior subluxation often suffer from very early and severe degenerative lesions. If a fixed posterior subluxation is diagnosed, the initial treatment includes the wear of a special brace (PTS Brace, Medi GmbH, Bayreuth, Germany), which pushes the tibia to anterior.25,26 Depending on boundary conditions and ligamentous instability, revision ACL reconstruction as well as PCL reconstruction might be indicated.26
Hardware Management
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 EZLoc Femoral Fixation of a Soft Tissue Graft
EZLoc Femoral Fixation of a Soft Tissue Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


