Chapter 23 Reverse abdominoplasty
• Tensioned reverse abdominoplasty (TRA) is not suitable for all patients, nor is it a substitute for conventional abdominoplasty.
• The greatest benefit of TRA is the possibility of treating deformities of the superior abdominal wall by using a direct approach to the region. This avoids using conventional abdominoplasty techniques to treat deformities located primarily at the upper abdomen.
• TRA is a simple, fast and easy technique that can be applied in association with other procedures, such as mini-abdominoplasty, liposuction, reduction mammoplasty, and augmentation mammoplasty – either by using prostheses or by means of retromammary insertion of dermal-fat flaps that would be resected from the most cephalic portion of the abdominal flap.
• Flap fixation to the aponeurosis drastically reduces the incidence of seroma formation. The upper traction of the flap reshapes the upper abdomen and distributes its supporting forces across the abdominal aponeurosis. This principle reduces tension on the resulting scar, favoring its quality and preventing postoperative displacement of the new mammary sulcus.
Introduction
The first description of skin and adipose tissue resection in the upper abdomen was made by Thorek in 1942.1 However, in 1977 Rebello & Franco described and systematized the approach through the inframammary sulcus for abdominal plastic surgery.2 After this period, reverse abdominoplasty was practically forgotten about for many years. This was primarily because it was said to result in poor esthetic results with regards to the inframammary scars.3
This chapter proposes a modification of the original technique, based on the upper traction of the flap and its strong fixation to the abdominal aponeurosis, resulting in a tension-free inframammary scar.4 The inframammary scar extension and the dissection amplitude are determined by the intensity of the supraumbilical deformities.
Preoperative Preparation
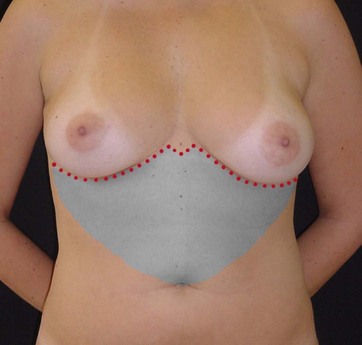
• Group 1: Larger amounts of skin to be resected require incision unification at the midline. In this group, the flap is dissected towards the umbilical scar, forming a single U-shaped tunnel (Fig. 23.1).
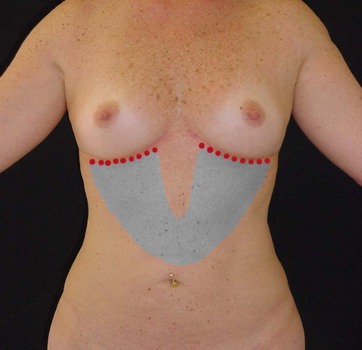
• Group 2: These patients have little or moderate supraumbilical skin laxity and no diastasis of the abdominal wall. The incisions will be limited to the inframammary regions, without unification at or crossing the midline. The flap dissection will produce two oblique tunnels towards the umbilical scar. The width of each tunnel will be determined by the breast width; and each tunnel joins the contralateral portion halfway between the inframammary sulcus and the umbilical scar (Fig. 23.2).
Surgical Technique
The flap to be dissected should be infiltrated with saline solution and epinephrine, at a concentration of 1 : 500 000. Epinephrine (1 mg) is used for each 500 ml of saline. The amount varies depending on the extension of the area to be treated and the patient’s measurements. One liter is needed for the entire abdominal surface, and about 500 ml for just the superior half are usually used. In cases of excessive fat, the procedure begins with a liposuction, which can be limited to the flap region or include the entire abdominal wall.5 In both groups, dissection is performed with electrocautery at the anterior aponeurotic plane, resulting in one or two dermal-fat flaps (Fig. 23.3).
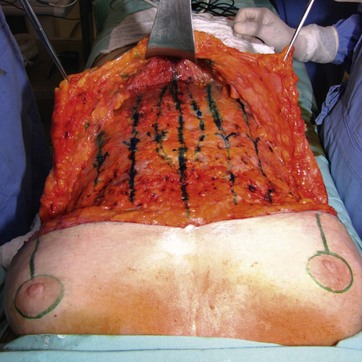
FIG. 23.3 Dissected flap showing traction lines and the midline fascia plication markings in methylene blue.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


