Replacement of Expander With Permanent Implant
Eric G. Halvorson
Joseph J. Disa
DEFINITION
Exchange of an expander for a permanent implant is performed as the second stage in two-stage implant breast reconstruction, following mastectomy and tissue expander placement (covered in previous chapter).
The advantages of two-stage implant reconstruction (compared to autologous reconstruction) include shorter operation, lack of donor site, shorter hospital stay, shorter recovery, patient control over final volume, and a “perkier” result.
The disadvantages of two-stage implant reconstruction include multiple postoperative office visits for expansions, discomfort associated with the expansion process, a second (albeit outpatient) surgery, and the permanent risks of implants (capsular contracture, rupture, rippling, infection, malposition, and exposure).
PATIENT HISTORY AND PHYSICAL FINDINGS
The initial consultation will have taken place prior to mastectomy and tissue expander placement; however, it is important to review the patient’s interim medical history prior to the exchange procedure, as interim changes are not uncommon as a patient progresses through breast cancer treatment, and their medical problems to assess risk factors for wound healing complications, for example, diabetes, radiation therapy, obesity, and smoking.
If patients have had radiotherapy, then waiting 3 to 6 months before performing the exchange procedure is advised.
Physical examination of the breasts is performed to evaluate expander size and position as well as the soft tissue envelope.
Implants often require position adjustment using capsulotomy and/or capsulorrhaphy.
Radiation changes are noted (if applicable), and if the skin and soft tissue surrounding the mastectomy scar are very thin, then an IMF approach to the exchange procedure should strongly be considered. Cutaneous recurrence should always be excluded.
Areas of soft tissue deficiency are evaluated for possible autologous fat grafting. This is fairly common in the upper pole.
Donor sites are also assessed. The medial thighs and hips are good donor sites. The abdomen should be spared as a possible future donor site for autologous reconstruction, if appropriate.
Expander size and volume is reviewed and determines implant selection (covered in the following text).
SURGICAL MANAGEMENT
Ideal candidates for two-stage implant reconstruction are thin, nonsmokers undergoing bilateral mastectomy who have not, and will not, receive radiotherapy.
Smokers are prone to wound healing complications and infection.
Radiotherapy increases the risk of infection, implant exposure, and capsular contracture.
Although obesity increases the risk of complications for most procedures, unless other risk factors are present, the exchange procedure on obese patients is very safe. Most of their risk will have occurred during the mastectomy and expander placement.
The exchange procedure can be an opportunity to modify implant position and also address some excess skin via lenticular excision.
Preoperative Planning and Implant Selection
Good communication with the breast surgeon and medical oncologist ensures oncologic goals are maintained and that reconstruction is appropriately staged.
The exchange procedure is typically delayed until one month following chemotherapy.
If radiotherapy is planned, the exchange procedure can be performed between chemotherapy and radiation, or 3 to 6 months following radiation. This is often determined by the preferences of the medical oncologist and radiation oncologist.
Patients on extended adjuvant therapy can safely undergo the exchange procedure; however, the specific agent must be assessed for risk of wound healing complications and/or thromboembolic events, and a discussion with the medical oncologist is advised.
Prior to the exchange procedure, the patient must be marked in the standing position.
The IMF is marked on each side and the midline is drawn between the sternal notch and xiphoid process.
A horizontal line is drawn from the lowest point of the IMF on each side to the midline, which helps identify vertical asymmetries in expander position.
The medial silhouette of each expander is marked, which helps identify horizontal asymmetries in expander position.
The ideal contour for the final implants is marked, revealing areas where capsulotomy will need to be performed to adjust the implant pocket.
If applicable, areas of soft tissue deficiency are outlined for autologous fat grafting, and the donor sites are marked.
Final implants are selected primarily based on volume, although width should be taken into consideration. A full discussion of implant types is beyond the scope of this chapter.
The majority of surgeons use smooth, round, high-profile silicone implants for reconstructive purposes, although textured anatomic silicone implants are also available.
Patients with very wide chests may require a moderateprofile implant that will have a larger base diameter for a given volume (although less projection).
A comparison of saline vs silicone implants is also beyond the scope of this chapter, but suffice it to say that the issue is controversial. The authors’ preference is to offer both types to patients noting the following advantages and disadvantages for each implant type:
Saline
Advantages: Implant rupture is immediately detected; removal/replacement of a ruptured implant is simple and quick.
Disadvantages: Re-expansion may be required if implant ruptures and is not replaced expeditiously; firmer than silicone, although this difference is negligible when good soft tissue coverage is present; higher potential for rippling if underfilled.
Silicone
Advantages: Softer, more “natural” feel
Disadvantages: Rupture is often clinically silent until capsular contracture and/or extracapsular rupture occurs, removal of a ruptured implant is a difficult operation that can involve removal of native tissue thus compromising subsequent reconstruction, and monitoring for silent implant rupture using magnetic resonance imaging (MRI) is not proven and has a definite risk of false positives and unnecessary surgeries.
Positioning
Patients are placed in the supine position under a general anesthetic with arms padded circumferentially and abducted at 80 to 90 degrees. The patient is positioned such that the sternum is parallel to the floor via head elevation or reverse Trendelenburg.
TECHNIQUES
▪ Implant Exchange
First Step—Removal of Tissue Expander
As noted earlier, the patient is marked in the standing position. Asymmetries are noted, and the ideal contour for the final implants is marked.
If performing fat grafting, the donor sites should be injected with tumescent solution at the beginning of the case to allow the epinephrine to take effect.
The mastectomy scars have often widened during expansion and these can be excised.
A stair-step approach to the implant pocket is usually performed, so any wound breakdown in one layer does not expose the suture line of the other layer.
If the scar is oriented obliquely (TECH FIG 1A), 2 to 4 cm of superomedial skin elevation will expose the pectoralis major, which can be incised parallel to the muscle fibers.
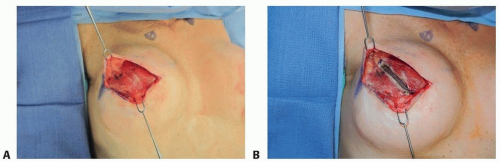
TECH FIG 1 • A. If the oblique incision is used for mastectomy, it is easy at the exchange procedure to elevate a superomedial flap exposing the pectoralis major muscle where it tends to be thicker. This will allow a “stair-step” approach to the implant pocket. Any wound healing issue at one level will not expose the suture line at the other level. (From Halvorson EG. Two-stage implant breast reconstruction. In: Mulholland MW, ed. Operative Techniques in Surgery. Vol 2. Philadelphia, PA: Wolters Kluwer; 2014.) B. A muscular incision is made parallel to the pectoralis major muscle fibers to access the implant pocket. The capsule is also incised with cautery, and the expander is bluntly separated from the capsule. (From Halvorson EG. Two-stage implant breast reconstruction. In: Mulholland MW, ed. Operative Techniques in Surgery. Vol 2. Philadelphia, PA: Wolters Kluwer; 2014.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access