Repair of Lip Defects With the Abbe Flap
Robert Beinrauh
Joseph H. Dayan
DEFINITION
A full-thickness portion of the lower lip, which includes the mucosa, orbicularis oris muscle, and skin with vermilion, based on the right or left inferior labial artery with mucosal venous attachments1
Used in reconstruction of defects of the upper lip (which do not involve the commissure) between one-third and one-half of the entire lip
A reverse Abbe flap (Estlander-Abbe flap) is the exact same flap only taken from the upper lip to reconstruct lower lip defects not involving the commissure.
We will use the technique for the traditional Abbe flap for this chapter, but recognize the reverse flap is the same technique based on the superior labial artery.
ANATOMY
The lips are a sphincter composed of a concentric ring of mucosa, muscle, and skin, which form a tight seal to prevent liquid from escaping the oral chamber and also to produce the labial sounds used in speech.
Orbicularis oris muscle:
A circumferential ring of muscle around the mouth that functions to compress and purse the lips together
The muscle fibers run horizontally on the upper and lower lips and begin at the modiolus.
There is an oblique extension of the muscle that runs from the commissure to the anterior nasal septum and nasal floor.
The inferior labial artery branches from the facial artery at the angle of the mouth.
PATHOGENESIS
Lip deformities can be congenital or acquired.
Congenital deformities are most commonly cleft lip defects.
Acquired deformities are most commonly due to traumatic or neoplastic etiologies.
PATIENT HISTORY AND PHYSICAL FINDINGS
Abbe flap is an excellent choice for defects of up to approximately 50% of the upper or lower lip.
Upper lip defects of 25% or less and lower lip defects of 33% or less can be closed primarily. However, the Abbe flap may be useful even in these relatively small defects if the philtral column is involved and requires reconstruction.
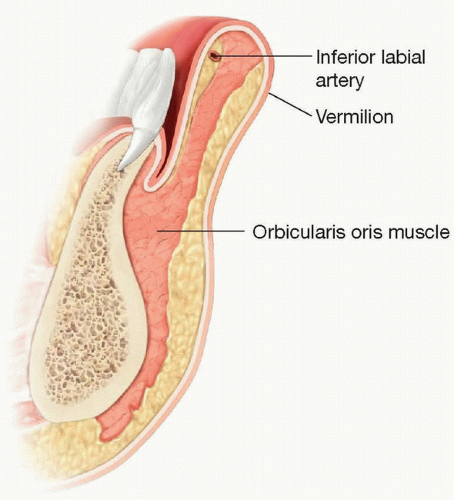
FIG 1 • Cross section of the lip showing inferior labial artery.
Lip defects larger than 50% of the lip may require either larger flaps, staged reconstruction, or a flap from a distant tissue site. However, there is some patient-to-patient variability in these size considerations due to anatomic considerations (ie, the baseline size of the lower lip) and the degree of skin laxity.
The Abbe flap is used for defects that do not involve the lip commissure. The Estlander flap is more useful for more lateral defects that involve the commissure. Abbe flap is excellent for reconstruction of bilateral cleft lip patients with scarred or short philtrums.3
IMAGING
No imaging is necessary for the Abbe flap. However, a pencil Doppler can be helpful to confirm position of inferior labial artery.
SURGICAL MANAGEMENT
Preoperative Planning
Size of the defect and layers of lip involved must be assessed.
The orbicularis oris muscle must be reconstructed to restore lip competence and avoid cosmetic deformities (eg, whistle deformity) with lip movement.
In general, the size of the lower lip Abbe should be less than 30% of the width of the lower lip to avoid microstomia. However, as noted, there is some variability based on skin laxity and anatomic considerations.
Positioning
Supine position and prep as for any facial procedure
Approach
Measure defect and use template of the wound to design the resection size of the lower lip.
The flap should be designed so that it will easily rotate into the defect without tension.
The flap should be located in an area with similar vermilion thickness as the edges of the defect.
Make the horizontal size of the lower lip flap dimension 50% of the horizontal size of the upper lip defect.4
Do not make the inferior extent of the flap extend beyond the mental crease.
Drive the incision laterally along the mental crease.
Note position of inferior labial artery with Doppler prior to incision.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree