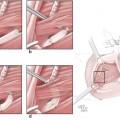
Fig. 8.1
Brown classification of maxillary defects (2000). (a, e) Class 1, (b) Class 2, (c) Class 3, (d) Class 4, (f) Subclass a, (g) Subclass b, (h) Subclass c
1.1.1 Classification of Vertical Defects
The vertical defects are divided into four classes according to the status of unilateral maxillary defect, of which they are divided into Class 1 and Class 2 according to whether there exists an area of oronasal fistula and they are divided into Class 3 and Class 4 according to the degree of orbital invasion. Specific classification is as follows:
- 1.
Class 1 defects – Maxillectomy without involvement of the sinus cavity.
- 2.
Class 2 defects – Low maxillectomy, including resection of walls of maxillary sinus and alveolar processes with preservation of the orbital floor and part of orbital tissue.
- 3.
Class 3 defects – High maxillectomy, including orbital floor or part of orbital tissues; the skull base may be involved, but the eye ball is preserved.
- 4.
Class 4 defects – Radical maxillectomy includes orbital exenteration, and the anterior skull base resection may or may not be included.
1.1.2 Classification of Horizontal Defects
The horizontal defects are divided into three subclasses according to the extent of resection of alveolar bone and palate:
- 1.
Subclass a – Unilateral resection of alveolar bone and palate without exceeding the midline and involving the nasal septum
- 2.
Subclass b – Resection of alveolar bone and palate exceeding the midline and involving the nasal septum
- 3.
Subclass c – Resection of total alveolar bone and palate
The vertical defects in the maxilla will make a huge impact on the appearance of the midface, while the horizontal defects will cause more functional disorders in chewing, swallowing, and pronunciation.
Brown classification covers the two aspects such as deformity and dysfunction (teeth occlusion, chewing, and pronunciation) in the midface (nose and paranasal sinuses, eyeballs) caused by the maxillary defects.
After Brown classification had been applied in clinic for years, Brown et al. (2010) also proposed a modified classification on this basis (Fig. 8.2). In addition to the original four classes, the vertical defects additionally include Class 5 defects that there exist the orbital and maxillary defects, but the alveolar process and palate are intact, and Class 6 defects that there exist nasal and surrounding maxillary defects; the horizontal defects additionally include a subclass of transverse defects that are less than or reach half of the hard palate. Since this modified classification is latestly proposed and has not yet been acknowledged by scholars worldwide, this chapter still uses Brown classification (2000).

Vertical defects
Horizontal defects
Fig. 8.2
Brown modified classification of maxillary defect (2010). (a) Class 1, (b) Class 2, (c) Class 3, (d) Class 4, (e) Class 5, (f) Class 6, (g) Subclass a, (h) Subclass b, (i) Subclass c, (j) Subclass d
1.2 The Principles for Repair and Reconstruction of the Maxilla
1.2.1 The Open Repair Should be Applied in Patients with Primary Maxillary Sinus Cancer and Highly Malignant Tumor
Because of the importance and complexity of the invasion range and the adjacent area of primary maxillary sinus cancer, and its poor biological behavior and survival rate, there is a certain difficulty in controlling the radical resection and safety margin. In view of such principles for facilitating the timely detection and treatment of postoperative recurrence of maxillary malignant tumor, the authors suggest that, for some maxillary tumors with higher malignant degree such as primary maxillary sinus cancer and osteosarcoma and combined with sinus wall damage, at the same time of performing radical tumor resection, the open repair methods of using the man-made support such as titanium mesh to maintain the appearance of the midface and wearing a prosthesis can be applied firstly, and then the surgical reconstruction can be implemented at 2 years after surgery when there is no local recurrence and distant metastasis.
1.2.2 The Patients with Tumors Which Can Be Radically Resected Can Be Treated with Immediate Closed Repair and Reconstruction
After radical maxillary tumor resection, due to simultaneous defects in bone tissues such as the orbital bone, cheekbone, and nasal bone, the patient’s appearance can be affected in different degrees. With the development of CT, MRI, and endoscopic techniques, the concerns in the past that the immediate use of autologous tissue to repair and reconstruct the maxilla may affect the examination of tumor recurrence are gradually eliminated, and there is no data to support that the prognoses of patients with surgical reconstruction are poorer than those of patients without surgical reconstruction. Therefore, for patients with tumors of higher malignant degree that primarily occurred in the palate and gingiva, the lesions are relatively limited and do not invade the maxillary sinus; for patients with tumors which can be completely removed or some patients with tumors of low malignant degree, the lesions invade the maxilla but do not invade through the sinus wall; the authors advocate that the closed repair and functional reconstruction are performed at one stage, according to the defect statuses in maxilla and adjacent bones; the artificial prosthesis (biological material or titanium mesh) can be used as scaffolds to reconstruct the anatomical shape, and then the oral surface or nasal surface is covered with the free composite tissue flap to restore the alveolar crest and palate and reconstruct the nasal passage and separate the oral and nasal cavities. The implants can be transplanted immediately or delayedly to restore the patient’s chewing function finally.
1.3 The Objectives and Requirements for Repair and Reconstruction of Maxillary Defects
The repair and reconstruction of maxillary defects should also take into account the recovery of function and appearance, and the effective targeted measures should be taken in accordance with the cause, location, extent, and type of the defect. The ideal reconstruction method must meet the following objectives and requirements [22]:
- 1.
Fill the defects caused by tumor surgery or trauma.
- 2.
Separate the oral and nasal cavities.
- 3.
Restore the support structure of the maxilla.
- 4.
Recover the function of tissues and organs of midface such as chewing, pronunciation, and swallowing.
- 5.
Reconstruct the position of the eye or fill and beautify the orbit after eye enucleation.
- 6.
Maintain a specific nasal airway.
- 7.
Provide necessary bony support for midface tissues such as the upper lip, nose, and cheek, thus avoiding the lower eyelid ectropion.
- 8.
Repair and reconstruct the appearance of the midface.
However, to date, there is no any kind of reconstruction method which can reach the objectives of all these maxillary reconstruction. For this purpose, the scholars from various countries continue to explore the ideal method of reconstruction.
1.4 The Basis for Repair and Reconstruction of Maxillary Defects and Its Meaning
At present, the method and timing of repairing the defects after resection of maxillary tumor remain controversial. For a very long time in the past, the traditional prosthesis occupied a dominant position in the repair of maxillary defects, and a surgery on donor site can be omitted. The prosthesis can fill the dead space, separate the nasal and oral cavities, and restore some chewing function and can be removed and put on at will, which is very favorable for observing whether there is early tumor recurrence. But its disadvantages are also obvious. Due to the fact that its retention condition is poor and it is not closed with the surrounding tissue, its adhesive force and attachment force are reduced accordingly; it tends to produce leakage and tilting, thereby affecting the functions such as sucking, chewing, and speech; and it is also not conducive to cleaning the oral environment; the long-term compression of prosthesis can cause secondary trauma and form the traumatic ulcers, so the postoperative recovery of the patient is not satisfactory.
In recent years, the vascularized tissue is transplanted to repair the maxillary defect, and this has been accepted by a growing number of physicians and patients; these techniques also make up the flaws of repair of maxillary defects with prosthesis fundamentally [5, 7–12, 17, 18, 22]. Therefore, the immediate repair with free composite tissue flap combined with the endosseous implant appears; thereby, not only the oronasal fistulas in the patients can be immediately closed, but also the chewing function, phonetic function, and nasal ventilation function of the patients after surgery can be recovered to varying degrees because of the repair with bone graft and the implant of better quality. In the past, the main concerns against the immediate repair are the worries that due to the covering of the dead space after maxillectomy by tissue flap, if the tumor recurs in future, the recurrent tumor foci cannot be directly observed with the naked eye, which may delay the diagnosis and treatment of the patient. With the development and popularization of modern medical imaging such as nasal endoscopy, CT, and MRI, it is possible to find the recurrent tumor foci earlier and earlier, which is conducive to the monitoring of early disease recurrence. Meanwhile, there is no literature suggesting that the survival rate of patients with immediate reconstruction is lower than that of the patients without immediate reconstruction; on the contrary, the survival rate of patients with immediate reconstruction is greater than that of the patients without immediate reconstruction.
For the ideal timing for repair and reconstruction of maxillary defects, the author thinks it should be performed immediately as soon as possible after surgery, because the immediate repair after surgery is conducive to early functional recovery and prevention of scar contracture; otherwise, the surgical reconstruction at the second stage will be harmfully affected, and the scar contracture will be more serious during postoperative radiotherapy. The long-term scar contracture and no hard tissue support in the infraorbital region after surgery often result in collapse and deformity of the midface of the patient, and it also brings some difficulties to the second-stage reconstruction. For the patients with defects in the intraoral mucosa, especially at the rear of the soft palate, if the tissues are not fixed and the muscle bundles are not accurately aligned during surgery, the obvious postoperative contracture can also occur. Therefore, the soft palate function will gradually decline and even is lost, and this leads to secondary velopharyngeal insufficiency and hypernasality in the patients after surgery, even if the second-stage surgery is performed in such patients, and it is quite difficult to improve the soft palate function after surgery. Therefore, the author believes that it should be advocated that the maxillary defects are immediately repaired with vascularized composite tissue flaps on the basis of strictly following the surgical indications and ensuring the safety margin.
2 Method for Repair and Reconstruction of Maxillary Defects
Because the pathological patterns and size ranges of various tumors involving the maxilla are different, and the anatomical structure of the maxilla itself is complex, the types and respective contents of the maxillectomy are different; thus, the resulted maxillary defects are not confined to a single defect and are complex series of diverse areas including small communication between the mouth and nose, and even the larger cranio-maxillofacial defect and the defects of different types and in different sites require different methods for repair and reconstruction; the surgeons engaged in the repair and reconstruction should select the most appropriate method for maxillary reconstruction according to the respective needs of each type of defects and each patient and reach the doctor-patient consensus as far as possible. So far, a lot of methods for repair and reconstruction have been used in repair and reconstruction of maxillary defects by various scholars worldwide, and they have gone through the test of time and practice, and especially the long-term effects are evaluated. Under the premise of strictly selecting indications, all the properly selected methods for repair and reconstruction will play their respective roles. These methods include skin graft transplantation and prosthesis repair, local tissue flap repair, regional tissue flap repair, artificial implant material, free bone (autograft, allograft, xenograft bones) transplantation, and vascularized tissue flap (fascia skin flap, myocutaneous flap, osseous myocutaneous flap, sandwich tissue flap, perforator skin flap, prefabricated or pre-formed tissue flaps, etc.). Of course, some of the abovementioned methods have gradually been eliminated, while other methods are being vigorously promoted by various scholars worldwide.
2.1 The Traditional Methods for Repair and Reconstruction of Maxillary Defects
The prosthodontic repair is mainly used for limited maxillary defects such as Class 1 defects of Brown classification, and the patients who are not suitable for repair with vascularized tissue flap and whose remaining teeth have enough support strength. The local tissue flaps such as palate island flap and buccal fat pad flap allow the surgeons to exchange for repair of smaller maxillary defects with minimal damage; some regional tissue flaps such as temporalis muscle flap and submental island flap have all been successfully used to reconstruct relatively larger defects in midface and maxilla. But because the regional tissue flaps often lack sufficient amount of tissue to fill the defect, as well as the length of the vascular pedicle is insufficient to reach the defect area, it is subjected to certain restrictions in application in repair and reconstruction of larger maxillary defects.
The artificial implant materials used in the reconstruction of the maxilla include titanium mesh, titanium, and biomaterials, of which the titanium mesh is most widely used and reliable. The safety of maxillary reconstruction with titanium mesh has long been recognized by the majority of scholars, because the titanium and titanium alloys have stable physical, chemical, and biological properties, good biocompatibility, light weight, high strength, corrosion resistance, and low conductivity and have the advantage of being transmitted by X-ray which other metals do not have. The application of titanium mesh in repair and reconstruction is dated back to its application in repair of defects in the skull, skull base, and orbital floor caused by tumors or trauma, and some scholars use it for reconstruction of maxillary defects, and the titanium mesh can be used alone and can also be used in combination with soft tissue flaps or free bone transplantation. Because the titanium mesh has a better image quality on CT and MRI, therefore, the use of the titanium mesh to reconstruct the mandible does not have an effect on the monitoring of tumor recurrence. Another advantage of the titanium mesh is that it has sufficient strength to support the midface and orbital contents. Tideman (1993) [3] first performed repair of maxillary defects by means of casting titanium mesh scaffold, filling it with autologous iliac bone, and wrapping it with temporalis myofascial flap; its recent application in four cases has obtained satisfactory results. But the shaping precision and flexibility of the casted titanium mesh are poor; there is a certain difficulty in making relatively great adjustment during surgery, coupled with reasons such as inadequate tissue volume in single temporalis myofascial flap; and it may result in exposure of titanium mesh after surgery; therefore, the technology has not been promoted. In addition, although the postoperative appearance of titanium mesh is generally satisfactory and the operation is relatively simple, however, if the surgeon is inexperienced and local blood supply and decreasing tension are ineffective, this can cause postoperative wound infection, fistula formation, and increase the probability of exposure of titanium mesh; it should be used with caution especially in patients with Class 3–4 defects of Brown classification or in patients who have received radiotherapy or need to have postoperative radiotherapy.
2.2 Reconstruction of the Maxillary Defect with Vascularized Free Tissue Flap
The vascularized free tissue flap can be used to reconstruct simultaneously the compound and complex defects in maxilla and midface and is not affected by the location of the donor site, and the vascularized free tissue flap includes two types such as soft tissue flap and hard tissue flap. The soft tissue flap mainly plays roles in covering or filling the defects and eliminating the dead space, but the soft tissue flap cannot be used for bone reconstruction of the maxillary defect and therefore cannot achieve the purpose of implanting artificial tooth for repair. The new alveolar crest repaired by soft tissue flap is relatively blunt, and at the same time, it is more difficult to restore the shapes of the buccal gingival sulcus and palatal arch, showing a trampoline-like form, and most patients are unable to wear partial or half mouth denture. In addition, although the recent results are often unsatisfactory, because of factors such as muscle atrophy and gravity action, the long-term effect of soft tissue flap reconstruction, especially the recovery of appearance, will be far less than expected. Since the 1990s, along with the application of vascularized composite bone muscle (skin) flaps in reconstruction of maxillary defects by various scholars worldwide, the vascularized composite bone muscle (skin) flap combined with the planting techniques are extensively used, which opens up a new era for repair and reconstruction of maxillary defects. The advantage of vascularized composite bone muscle (skin) flap is that it can reconstruct the osseous pillar and appearance of the midface and make up the shortcoming that the soft tissue flap cannot serve as the support due to the long-term atrophy; the chewing function can be reconstructed combined with the implant denture technique, so as to achieve the true meaning of the functional reconstruction of maxilla.
2.2.1 The Indications for Maxillary Reconstruction with the Vascularized Free Tissue Flap
The related indications for maxillary reconstruction with the vascularized free tissue flap are a problem worthy to be discussed. Although a variety of pedicle or free soft tissue flaps were used to fill or cover the dead space caused by maxillary defects, the author thinks it can only be called as repair; contemporarily, the application of composite bone muscle (skin) flap combined with implant placement recovers the occlusal relationship and the chewing function of the maxilla. Since both the function and appearance are recovered, it can only be called as reconstruction.
In the following circumstances, it may be considered that the vascularized free flaps are used for maxillary reconstruction:
- 1.
The patients have concomitant oral mucosa (skin) defects in the adjacent site and the defects are larger, for example, the concomitant larger tissue defects in sites such as the buccal mucosa (skin), soft palate, and lateral pharyngeal wall can be repaired with the latissimus dorsi muscle, pectoralis major muscle, transverse rectus abdominis myocutaneous flap, or anterolateral thigh skin flap.
- 2.
For the patients with more limited range of tumor, such as Class 2 defects of Brown classification and with younger age, the authors advocate that the fibula composite flap is used for repair; if the bilateral defects exist, it is also considered that the iliac bone muscle (skin) muscle flap or the shoulder blade myocutaneous flap is used for repair, and the implant denture repair can be performed immediately or at the second stage.
- 3.
The resection range is larger; for the patients with Class 3 defect of Brown classification, the authors recommend that the titanium mesh is taken as the support frames of the anterior wall of maxillary sinus and the inferior wall of orbit; the fibula composite flap is used to close the communication between mouth and nose simultaneously in the tooth socket area.
- 4.
The follow-up has been performed for 2 years after maxillectomy, and there are no patients with recurrent tumors who ask for autologous tissue repair.
2.2.2 The Common Methods for Maxillary Reconstruction with Vascularized Free Tissue Flap
As mentioned earlier, currently, the common methods for maxillary reconstruction with vascularized free tissue flap are divided into two types, soft tissue flap and hard tissue flap, and the soft tissue flaps include the radial forearm skin flap, anterolateral thigh skin flap, pectoralis major myocutaneous flap, transverse rectus abdominis myocutaneous flap, and the transverse rectus abdominis myocutaneous flap; the hard tissue flaps include the fibula myocutaneous flap, iliac osteo-myocutaneous flap, shoulder blade myocutaneous flap, and radial forearm osteocutaneous flap. Various methods have their own indications and advantages and disadvantages. Given the limited space, this section will focus on the reconstruction of the maxilla with more commonly used radial forearm osteocutaneous flap and the fibula myocutaneous flap.
2.3 Application of the Computer-Aided Design/Computer-Aided Manufacturing Technology in the Maxillary Reconstruction
Although the vascularized composite bone flap has played a dominant role in the reconstruction of maxillary defects, for bone graft shaping and facial appearance reconstruction, except on the basis of skull specimens, the previous operators always carried out estimation according to individual clinical experience, whose subjectivities can be imagined, so that the repeatability was poor, and it was difficult to recover the ideal appearance of the midface, which had a certain distance from the requirements for reconstruction of maxillofacial appearance and function. Therefore, how to achieve the optimum combination and have a good construction and prediction before surgery? The appearances and the application of technologies such as the rapid prototyping and computer-aided design (CAD)/computer-aided manufacturing (CAM) provide reliable guarantees for reconstructing new ideal morphology of the maxilla to restore its original appearance and function and realize individualized reconstruction in the true sense. The rapid prototyping is a high-tech manufacturing technology which started to be commercialized at the end of the 1980s. Since the CAD/CAM system had characteristics such as precision, visualization, and strong operability, this technology was introduced into surgery soon and gradually showed its advantages in the field of oral and maxillofacial surgery. For example, Tideman et al. (1993) performed immediate repair for the defect after maxillectomy using combined methods such as pure titanium mesh scaffold casted by CAD/CAM technology, filling with autogenous iliac bone block and the transfer of temporalis myofascial flap to cover the inner and outer layers of the scaffold, which recently received satisfactory results. Since 2000, the author [10, 11] had been applying the CAD/CAM technology as the means of model surgery for reconstruction of large maxillary defects (Class 2–3 defects of Brown classification), had been using the preoperative prefabricated titanium mesh to recover the appearance of the maxilla, and thus had achieved a good reconstruction effect through reconstructing the anatomical shape of the maxilla. The specific surgical approach will be detailed later.
The application of CAD/CAM technology in the reconstruction of maxillary defects has the following advantages compared with the traditional method: First, it can more accurately recover the appearance of the maxilla and thus effectively carry out anatomical reconstruction. Secondly, the osteotomy guide is designed preoperatively according to the model to determine the fixed locations of osteotomy line, titanium mesh, and titanium plate, which is conducive to guiding the accurate placement of the bone graft and the axial direction of implant placement during surgery to prevent postoperative deviation, in addition, which can effectively save time and attain the result with half effort. But it still has disadvantages such as longer production cycle, weakened bone area which is not conducive to stent bending, and slightly higher costs.
2.4 Reconstruct of the Maxilla Using the Radial Forearm Skin Flap Combined with CAD/CAM Prefabricated Titanium Mesh
The radial forearm skin flap was formed initially by a Chinese scholar Professor Yang Guofan (1978). Because it has advantages such as long vascular pedicle, thick diameter, larger area for harvesting the skin and fascia, and simpler preparation, it is considered to be a good choice for the reconstruction of oral mucosa and has been widely used. In the reconstruction of maxilla, the radial forearm skin flap is used previously to mainly reconstruct the soft palate defects and the limited Class 1 defects of Brown classification. Since 2000, the author had been applying the CAD/CAM technology as the means of model surgery for reconstruction of large maxillary defects – Class 2–3 defects of Brown classification – and had been using the preoperative prefabricated titanium mesh to recover the appearance of the maxilla. The anatomic structure of the maxilla at one stage was reconstructed with the method of folding the free radial forearm skin flap to repair the oral and nasal wounds, and thus the functions such as chewing, speaking, and ventilation were restored. To 2002, it had been clinically applied in 19 cases, and the satisfactory results had been obtained. This method makes the three-dimensional reconstruction of large maxillary defects more accurate and more individualized. This method will be introduced in the following paragraph through taking the reconstruction of Class 3 defects of Brown classification for an example.
2.4.1 Preoperative Preparation
- 1.
In addition to routine preoperative examination to exclude systemic disease and other surgical contraindications, the patients with the maxillary cancer should undergo three-dimensional CT examination to determine the lesion range and the invasion status in the adjacent tissues; the patients with malignant tumors should be examined to determine whether the cervical lymph node metastasis exists and to exclude the possibility of distant metastasis.
- 2.
Allen’s test is performed in the forearm, the refluxes of the superficial palmar arch and deep palmar arch are inspected, and the patency of the cephalic vein is also inspected. One side with better reflux and no history of previous surgery, trauma, and intravenous chemotherapy is selected as the donor site and is protected.
- 3.
Three-dimensional CT data of the maxilla are recorded on a CD. The engineering technicians will read data via CAD/CAM software and then simulate the maxillary resection on the computer and form the maxillary defect images on the affected side. The maxilla at the healthy side will be copied to the affected side using the principle of mirror symmetry to produce a mirror image of the affected side after reconstruction, namely, the rehabilitation image. According to computer images, the rapid prototyping technology is used to produce the corresponding rehabilitation model. Three-dimensional titanium mesh stents of the orbital floor, the inner side of the nasal cavity, the maxillary anterior wall, and the bottom wall are prefabricated on the rehabilitation model of the maxilla before surgery.
- 4.
Before surgery, the oral cavity clean governance is performed, and the skin in surgical area is shaved and cleaned, and the 400–600 ml of blood is prepared.
2.4.2 Surgical Procedures
- 1.
The general anesthesia with tracheal intubation is carried out, and then the routine disinfection and draping are performed.
- 2.
Incision design. The extraoral incision starts from the vermilion border of the lower lip at 1 cm from the medial side of the corner of the mouth, along the vermilion border, outward along the vermilion border to the corner of the mouth, then from the corner of the mouth and parallel to the nasolabial groove (correspond to the body surface projection of the posterior margin of deltoid muscle) and travels obliquely downward to cross the lower margin of the mandible and reach an area at 2 cm below the lower margin, and then a parallel incision is performed in the neck at 2 cm below the lower margin of the mandible, bypass the underneath of the mandibular angle. The cervical incision may be extended to a site below the mastoid tip, or an additional longitudinal cervical incision is performed for cervical lymph node dissection. The starting point of the intraoral incision is continued to the starting point of extraoral incision in vermilion border of lower li and travels obliquely downward to the upward side of the mandibular buccal gingival sulcus and then parallel to the mandibular buccal gingival sulcus and along pterygomandibular folds to bypass the maxillary tuberosity and then along the maxillary gingival sulcus to cross the midline (Fig. 8.3).Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


