Fig. 13.1
Three-partition method for the upper surface of the skull base
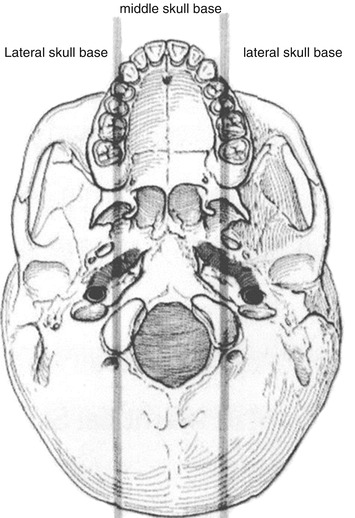
Fig. 13.2
Krespi partitioning method for the lower surface of the skull base
2.2 The Range of the Defects After Craniomaxillofacial Tumor Surgery
As mentioned above, the defects after craniomaxillofacial tumor surgery often include a diverse range of complex tissue defects. Thinking from different perspectives, the contents included in complex tissue defects also differ to some extent. In terms of tissue types, the defects after craniomaxillofacial tumor surgery may include parenchymal defect, the dura mater defect of the skull base, the bone structure defects of the skull base, craniomaxillofacial bone defect, defect of the upper respiratory tract mucosa, intraoral mucosal defect, and skin and soft tissue defect, and the defects after craniomaxillofacial tumor surgery are often the complex defects consisting of abovementioned different tissue types. From the perspective of coronal position, the craniomaxillofacial area can be divided into different anatomical areas such as frontal area, temporal area, orbital area, zygomatic area, suborbital area, nasal area, and lateral facial area, and the defects after craniomaxillofacial tumor surgery are often the complex defects involving multiple areas among abovementioned areas. From the perspective of the skull base partition, the anterior cranial fossa defects can include the dura mater, skull base bone, orbital contents, nose, maxilla, and palate; the middle cranial fossa defects can include the dura mater, skull base bone, maxillary bone, soft tissues in preauricular area and the parotid area, mandible, external ear, and temporal bone, and the posterior cranial fossa defects can include the dura mater, skull base bone, occipital bone, retroauricular soft tissue, external ear, and temporal bone. The defects after craniomaxillofacial tumor surgery are often the complex defects consisting of different areas among abovementioned partitions.
2.3 Classification of the Defects After Craniomaxillofacial Tumor Surgery
Because the defects after craniomaxillofacial tumor surgery are more complicated with a wider range, currently, there are rare classifications for the defects after craniomaxillofacial tumor surgery at home and abroad. The vast majority of the literatures are based on the partitions of the intracranial or extracranial skull base to assess the defects after craniomaxillofacial tumor surgery. Since the partitioning methods for the extracranial skull base have not been unified, the use of the method according to the partitions of the skull base to classify the defects after craniomaxillofacial tumor surgery will lead to confusion in the classification of the defects after craniomaxillofacial tumor surgery, which is not conducive to selecting the appropriate repair method and comparatively analyzing the curative effects and survival parameters of different data. Furthermore, the partitioning method of the skull base usually does not include the anatomical structures adjacent to the skull base such as the brain, orbit, nasal cavity, paranasal sinuses, and upper and lower jaw bones, which actually has certain differences with the clinical practice. American Memorial Sloan Kettering Cancer Center (2007), depending on different scopes of the defects after craniomaxillofacial tumor surgery, presented a relatively simple classification method for the defects after craniomaxillofacial tumor surgery (Fig. 13.3). They divided the upper surface of the skull base into two parts of anterior cranial fossa and middle cranial fossa in a horizontal direction at first, and then the defects in anterior cranial fossa are divided into three types of lateral defect, central defect, and anterolateral defect. In the coronal direction, any type of anterior cranial fossa and middle cranial fossa defects can include one or several anatomical defects among the nasal cavity, maxilla, orbit, mandible, skin, and mucous membrane. The classification method is relatively simple, but the defects of tissues such as the posterior cranial fossa and the adjacent external ear and parotid gland are not taken into account.
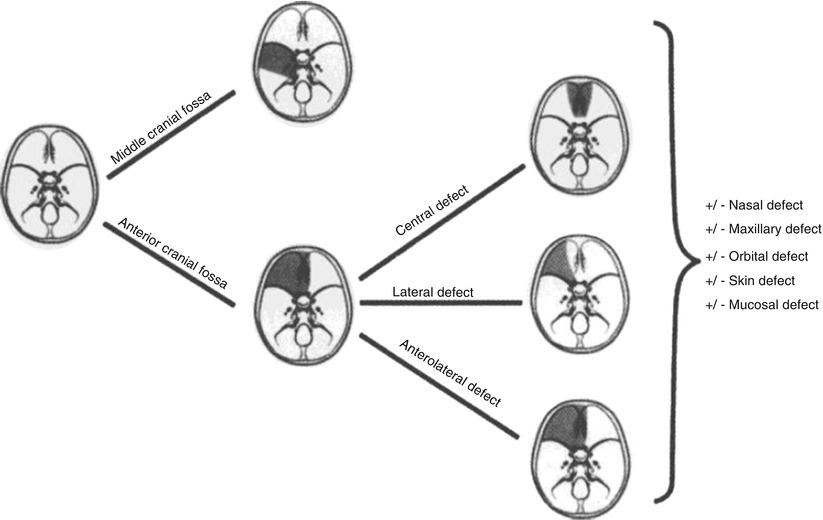
Fig. 13.3
Classification method for the defects after craniomaxillofacial tumor surgery of the American Memorial Sloan Kettering Cancer Center
3 Functional Reconstruction of Defects After Resection of Cranial and Maxillofacial Tumors
No matter in the past or present, all treatments of craniomaxillofacial tumors attach great emphasis to the thoroughness of the first treatment, and the concepts of en bloc resection or block resection, super-radical surgery or extended radical surgery, as well as the surgical methods such as combined craniomaxillofacial resection, carotid artery resection, and total tongue – total throat resection – successively appear. However, on the one hand, the abovementioned super-radical surgery or extended radical surgery provides a certain guarantee for the thoroughness of the surgery; on the other hand, it leads to the loss of a large amount of craniomaxillofacial and cervical tissues, secondary deformity, and disability, thus severely affecting the quality of life of patients. With the progress of technology and the improvement of malignant tumor cure rate, at the same time of pursuing the cure of the tumors, both doctors and patients are also eager to restore the original appearance and function, and the change in concepts promotes the development of resection and the repair and reconstruction of craniomaxillofacial tumors. The functional reconstruction of defects after craniomaxillofacial tumor surgery is to carry out immediate or delayed reconstruction of craniomaxillofacial tissue defects or organ loss due to tumor resection, so as to achieve the purpose of restoring the function and appearance. The functional repair and reconstruction of defects after craniomaxillofacial tumor surgery are the emerging technologies which are developed on the basis of craniomaxillofacial oncological surgery and are the results of the rapid development of reconstructive surgical techniques, extensive application of medical biological materials, and especially the application of microsurgical techniques and dental implant surgical technique combined with oncological surgical techniques. With the development of perforator skin flap, fascia skin flap, and sensory skin flap as well as the application of materials such as absorbable reconstruction plate, screws, and implants, the modern concepts on repair and reconstruction require the reconstruction surgeons to carry out individualized repair and reconstruction which are tailored and varied with each individual with minimal tissue damages and complications, so as to maximize the recovery of the appearance and function of the craniomaxillofacial area and improve the quality of life of patients. This section will introduce the repair and reconstruction of defects after craniomaxillofacial tumor surgery with different ranges and different types.
3.1 Advantages and Objectives of Functional Reconstruction of Defects After Craniomaxillofacial Tumor Surgery
Since the end of the twentieth century, especially in the last 10 years, the immediate repair and reconstruction of defects after craniomaxillofacial tumor surgery have become the mainstream and preferred surgical method, which is due to that the immediate repair and reconstruction have more advantages.
3.1.1 Advantages of the Immediate Repair and Reconstruction of Defects After Craniomaxillofacial Tumor Surgery
- 1.
The immediate repair and reconstruction of defects are conducive to protecting important exposed tissues or organs, such as the carotid artery and brain tissue, so as to reduce the incidence of postoperative complications.
- 2.
The basic anatomic structure and morphology can be recovered early in patients, which contributes to early implementation of other subsequent combination therapy and early recovery of physiological functions.
- 3.
It is beneficial to the rehabilitation of patients after surgery to eliminate or reduce the psychological and psychiatric injuries of the patients due to residual defects.
- 4.
It can save medical resources and medical costs.
3.1.2 Objectives of Repair and Reconstruction of Defects After Craniomaxillofacial Tumor Surgery
For different types of defects after craniomaxillofacial tumor surgery, their objectives of repair and reconstruction are also not the same. In terms of small defect of the cerebral tissue, its objectives of repair and reconstruction are to restore anatomically the integrity of the cranial cavity and the structures which maintain the normal intracranial pressure and prevent the brain and its nerves and bloods as the vital center of the human body from suffering the physical traumas (mechanical trauma, freezing, hyperthermia, and ionizing radiation), chemical damage, and microbial attack. In terms of a wide range of complex craniomaxillofacial defect, its objectives of repair and reconstruction are as follows:
- 1.
To repair the defect or cover the exposed dura mater and prevent the brain tissue exposure, cerebrospinal fluid leakage, retrograde intracranial infection, and cerebral herniation.
- 2.
To support the brain tissue and eyeballs and periorbital tissues. The skull defects due to surgery may cause serious complications such as encephalocele and epilepsy as well as exophthalmos and enophthalmos in patients. Therefore, properly repairing the skull and its subsidiary structure to restore the normal anatomical structure of the cranial cavity as far as possible in this type of surgery has very important significances for preventing the complications after craniomaxillofacial tumor surgery and ensuring the success of the operation.
- 3.
To separate traffic between the brain tissue and oronasal cavities, provide sufficient tissue to fill the dead space, and restore the nasal and oral mucosal lining as far as possible.
- 4.
To reconstruct the orbital, nasal, and oropharyngeal cavities and reconstruct the three-dimension morphology and function of craniomaxillofacial bones and soft tissues. From the perspective of aesthetic form, the skull is the basis to construct the contour of the upper face. For the skull defects due to surgical resection, the accurate and appropriate repair not only creates an anatomical basis for reshaping the craniofacial appearance but also plays a very important role in the remodeling the self-confidences and social psychologies of the patients and improving their quality of life.
3.2 The Principles for Functional Reconstruction of Defects After Craniomaxillofacial Tumor Surgery
Because the defects after craniomaxillofacial tumor surgery are mostly the complex defects comprising of different types of tissues and different anatomical structures, different types of tissues have their own reconstruction principles. For example, the principles for repair of dura mater defect are that the dura mater sac is completely closed without cerebrospinal fluid leakage, the repaired tissues have strong anti-infection ability and no rejection reaction, and the adhesion between the cerebral cortex and the repaired tissues is reduced, while the repair of skull base defects should primarily focus on the coverage and protection of the dura mater to reduce the chance of meningeal and intracranial infections. Therefore, the principle for skull defect reconstruction is to basically restore the integrity of the bony cranial cavity, isolate and prevent the infection of extracranial source, and reconstruct the shape of the skull. As for soft tissue defects, the appropriate repair method should be selected according to the scope of the defect. The medium and small skull base defects should be repaired preferably selecting the adjacent local tissue flap, and the large skull base defects or craniomaxillofacial complex defects should be repaired preferably selecting revascularized free tissue flap. The indications for repair of craniomaxillofacial defects with revascularized free tissue flap are as follows: ① The massive soft tissue defect which must be repaired. ② There is obvious dead space in the skull base. ③ Serious damages to maxillofacial anatomical morphology. ④ The defects in the temporal fossa, infratemporal fossa, parotid bed, and midface region. ⑤ Carotid artery exposure. ⑥ The patients have previous history of radiotherapy or craniofacial surgery.
Currently, the method of carrying out hard tissue reconstruction for skull defect in the same period remains controversial. Domestic and foreign scholars believe that the skull defects which are less than 4 cm2 can be filled with myoplasm and skin graft or repaired with pad or repaired with through transposition of nasal septum to get a good effect; the skull defects which are more than 4 cm2 can be repaired with the free temporal bone and iliac bone; the harvested bone block is made into a wedge shape and embedded in the defect area at first and then is fixed with thick silk or knot tying silk. And then the pre-prepared split-thickness skin graft is lined on the nasal surface of the skull base after the bone is fixed, which is greater than the bone defect by 1–2 cm2, and subsequently the iodoform strip is packed in its underneath to prevent slippage or untight fitting; thus such three layers of materials form a sandwich-like artificial skull base to get a good effect. The advantage of the abovementioned repair method is simple, but it only applies to patients with tumors that primarily occurred in the ethmoidal sinus in which the partial maxilla (frontal sinus) is resected and most of the maxilla exists, which can play a good role in supporting the repaired tissues. If a wide range of complex defects after craniomaxillofacial tumor surgery are repaired with free bone and free skin graft transplantation, this will easily lead to necrosis, falling off, and failure of the repaired tissues.
- 1.
Imola et al. [10] (2003) believed that the indications for repair of the defects after craniomaxillofacial tumor surgery with bone tissue are as follows: ① The large defect in the bone of the skull base which leads to brain herniation. ② The near-total or total orbital roof defect which can lead to exophthalmos. ③ The lateral orbital wall or orbital floor defect which can lead to exophthalmos. ④ The cranio-orbital defects which lack adequate soft tissue support or generated craniofacial deformities. ⑤ The defects in the maxilla, mandible, and the glenoid fossa of the temporomandibular joint which cause facial deformities, occlusal disturbance, and chewing dysfunction
- 2.
We consider that the indications for hard tissue reconstruction of skull defects in the same period are as follows [12]: ① The bony defect in skull vault ≥3.0 cm.
② The bony defect of the skull base ≥1.5 cm. ③ The bony defect of the skull base <1.5 cm but with dura mater defect, or there are larger dead spaces in epidural area. ④ The intracranial important neurovascular structures are exposed in the skull defect area, and the thickness of the skin and soft tissue is insufficient to protect their safety. ⑤ The important sites such as frontal orbit affect the appearance.
As for the materials for hard tissue reconstruction, the titanium mesh, nonvascularized bone grafts, or vascularized bone graft can be selected according to defect status.
3.3 The Influencing Factors on the Selection of Functional Reconstruction Methods for the Defects After Craniomaxillofacial Tumor Surgery
Imola et al. [10] (2003) considered that the influencing factors on the selection of functional reconstruction methods for the defects after craniomaxillofacial tumor surgery include: the size of the dura mater defect, the degree of openness between the cranial contents and the upper digestive tract (upper respiratory tract) (including the range of craniomaxillofacial skin, soft tissue, bone, and mucosa defects), whether the patients have preoperative radiotherapy or plan to have postoperative radiotherapy, whether the patients have local and systemic disease factors which affect the healing, and the reliability of local tissue to be used for repair.
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


