Reconstructive and Esthetic Breast Surgery
3.3.1 Mastopexy and Lifting
Aims and Methods
The main focus of breast surgery is on the various breast-conserving, ablative, and reconstructive techniques used to treat breast cancer. Plastic surgery and reconstructive techniques are employed both in the oncoplastic operations performed on patients with breast cancer and in the cosmetic procedures performed on women who are dissatisfied with the shape of their breasts. Because of the significance of the breasts for a woman’s self-image, many women are unhappy with the shape they were born with or with the physiological changes in shape produced by aging. Deriving from this unhappiness is the need to lift the aging breast and correct the breast ptosis that develops in many women in the course of their lives and following pregnancy. The breast surgeon has an obligation to treat the woman’s wishes with respect, dispel unreasonable expectations, present realistic options, and also explain that surgery may be waived in a situation that is ultimately not pathological. The technical aspects of breast tightening or lifting will be presented below and placed in context with the oncoplastic techniques described elsewhere in this book.
Indications and Contraindications
Indications
Indications for cosmetic mastopexy (breast lifting) include the affected woman’s unhappiness with her self-image. Breast ptosis is defined by the position of the nipple–areola complex in relation to the inframammary fold. The position regarded as esthetically “normal” is well above the inframammary fold. In mild (grade 1) ptosis, the nipple–areola complex has sunk to the level of this fold. If it is below the inframammary line but above the lower outline of the breast, this is moderate (grade 2) ptosis; severe (grade 3) ptosis is present when it forms the inferior outline of the breast.
Contraindications
Mastopexy is contraindicated especially in very young patients who have not yet completed their families, particularly if pregnancy is planned in the near future. Pregnancy can greatly alter breast anatomy so that good operative results may be completely lost. It is also specifically, albeit theoretically, contraindicated in pregnant patients, minors, and young patients in whom breast development is still incomplete. Great caution is warranted in patients with inadequately treated and unstable underlying psychiatric disorders (bipolar disorder, depression). Circulatory disorders of the skin, smoking, diabetes mellitus, and concomitant corticosteroid treatment are relative medical contraindications.
Operation Risks and Informed Consent
Because of the elective nature of the procedure, the patient must be informed in detail about all possible complications: bleeding and secondary hemorrhage, possibly with the (very rare) need for transfusion with the resulting risks of hepatitis B and C and HIV infection, nerve injury, paresis, impaired sensation, especially of the nipple–areola complex, delayed wound healing, and the necessity of secondary operations. Other possible though very rare complications include loss of the nipple–areola complex as a result of impaired perfusion, loss of the entire breast due to purulent infection (extremely rare), scarring, an ugly cosmetic result, nonpermanent operation success, anesthesia incidents, and postoperative complications such as thrombosis, embolism, and death. Possible deformities of the breast and postoperative asymmetry of form and volume, especially with regard to the nipple–areola complex, must be discussed. Because of the medicolegal necessity of comprehensive information, the risks must be presented in the correct order. As health insurance companies may be critical, patients should also be informed of the possible financial consequences of complications due directly to the operation: many health insurers are no longer willing to pay for the treatment of complications of cosmetic surgery.
Operation Planning
Preparation for all cosmetic operations follows a similar pattern:
Medical history, clinical examination to assess the anatomy
Inspection, palpation, exclusion of breast disease requiring direct treatment
Exclusion of clinically occult breast cancer by age-appropriate imaging (mammography, ultrasonography)
Detailed discussion with the patient about her motives, wishes, and expectations. The risk (including medicolegal risk) of a dissatisfied and litigious patient postoperatively is particularly great when expectations are unrealistic. A psychological assessment may be warranted.
Detailed demonstration of the patient’s actual condition with explanations: degree of ptosis, pre-existing asymmetry, chest wall anatomy and its importance for breast contour, differences in size. Make a photographic record. The patient often notices obvious but long-standing asymmetry only postoperatively. Careful preoperative discussion can help to avoid major postoperative problems.
Discussion of different surgical techniques with illustration of potential results using photos. Ideal, average, and less successful results should be presented. The patient should have seen pictures of the most important complications. Realistic expectations should be established.
Explanation of the extent of the operation, convalescence, and all possible complications
Consent to the procedure
The incision line is drawn with the patient standing or sitting up, either the day before or immediately prior to operation; the patient should be informed precisely about the position of the scar.
Anesthesiological preoperative investigations depending on the patient’s age and local practice
Thrombosis prophylaxis according to risk factors: low molecular weight heparin
Antibiotic prophylaxis: first or second generation cephalosporin
Moderately difficult to difficult surgery: takes 1 to 2 hours per side depending on the degree of ptosis; surgeon and ideally one assistant
Anesthesia and Positioning
Special Instruments
Breast set: scalpel, fine dissecting scissors, electrocautery knife, electrocautery needle, skin hooks, abdominal towels
Procedure
Preparation
Since a bladder catheter is not placed, the patient should go to the toilet before transport to the operating room.
The patient is identified in the pre-op and operating room: file and patient match, patient confirms the planned operation according to the entry in her file and the preoperative marking.
Intubation versus laryngeal mask
Positioning: semi-sitting positions are favored by many surgeons, as in oncoplastic surgery. The arms are abducted bilaterally (some surgeons prefer them by the patient’s sides).
Skin preparation, sterile draping: thoracic access
Operation
The appropriate technique is chosen preoperatively, jointly with the patient. The shape of the breast largely dictates the incision but the patient should be informed precisely about the position of the scar.
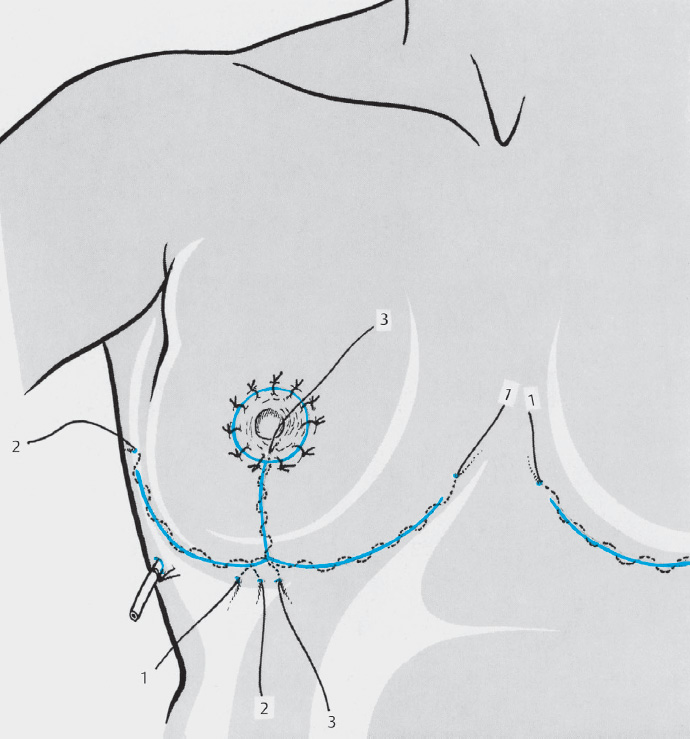
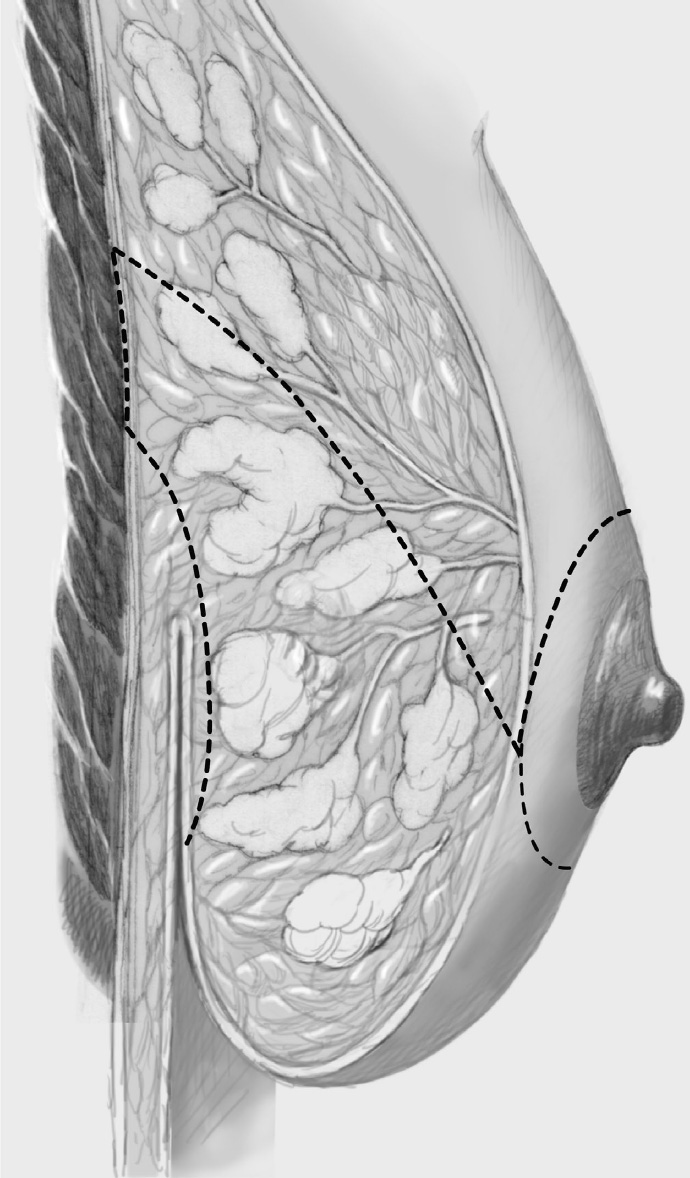
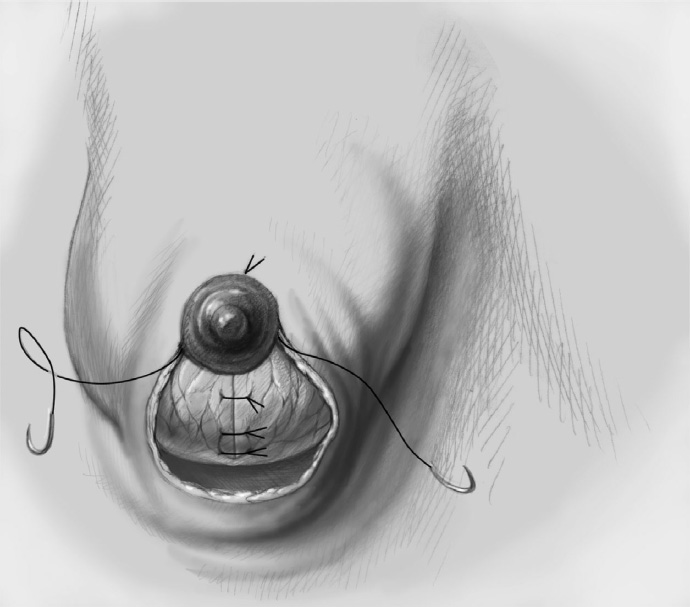
Mastopexy essentially involves tightening of the skin envelope and lifting the breast (fixing the breast to the chest wall to prevent renewed ptosis and relieve pressure on the tightened skin) without a significant reduction in the breast, atrophy of which is often the cause of the undesirable cosmetic situation. The approach is related to that of reduction mammoplasty, as intramammary dissection is also required for the mastopexy. Accordingly, the access route is used to dissect the breast free (subcutaneous or retroglandular dissection plane) and then fix the superior or periareolar part higher on the chest wall by suturing it to the pectoralis fascia. The reduced skin envelope is then placed over the repositioned breast and the nipple–areola complex is brought again into a central position.
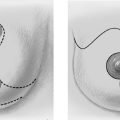
Four incision techniques are used for breast reduction: periareolar incision, periareolar incision with inferior vertical extension (equivalent to the Marchac or LeJour reduction technique), B-technique (rarely also called the L-technique), and inverted T. Other techniques apart from these four approaches may be used but ultimately these are minor variants.
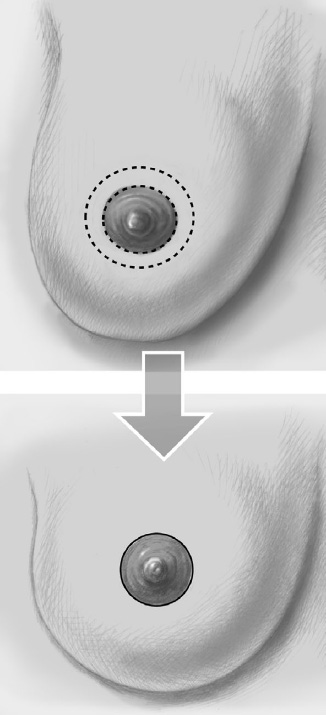
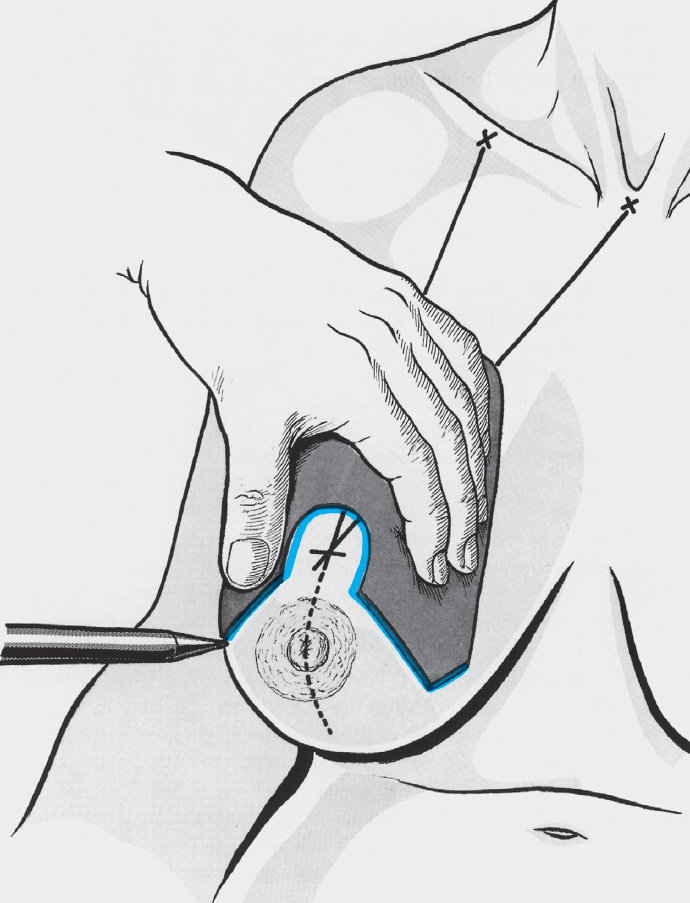
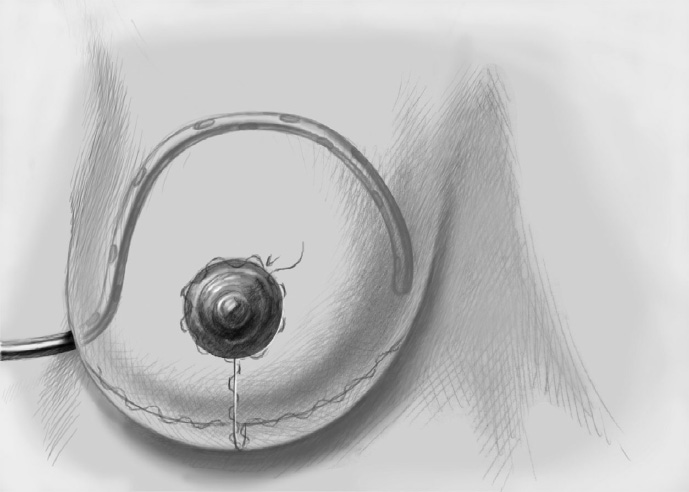
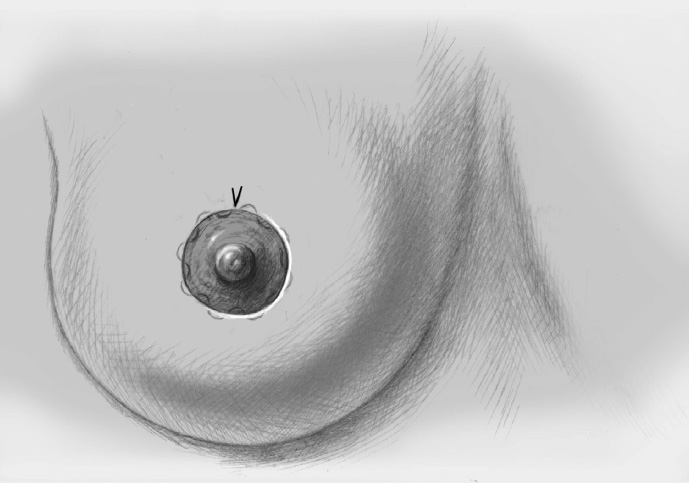
If the ptosis is mild and the breasts are not too heavy, a purely symmetrical or eccentric periareolar incision may be chosen. In principle, a symmetrical or asymmetrical ring of epidermis around the nipple is excised and the remaining skin envelope is thereby tightened when it is reapproximated. The main disadvantage is that the lateral projection of the breast cannot be altered and the tightening is often insufficient or short-term with loss of projection height. In addition, the diameter of the resected ring of skin must not be greater than 10 cm as otherwise the excessive creasing effect will persist even when the breast is elastic. Before reapproximating the two circular incision lines, the outer one is shrunk by a gathering suture. Use of a slowly absorbable suture material is recommended.
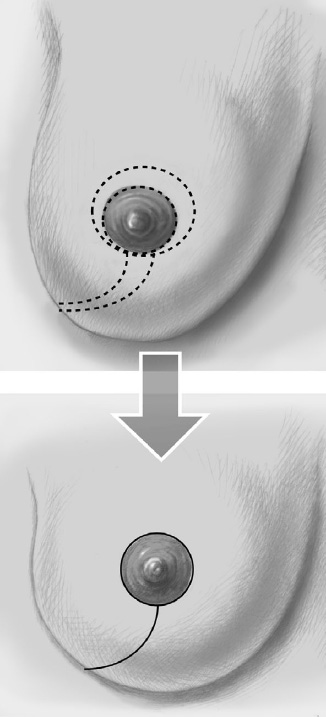
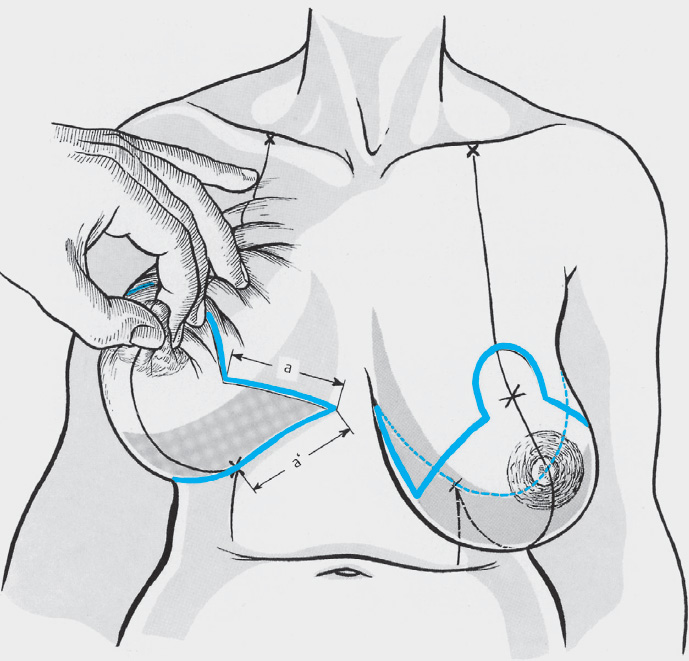
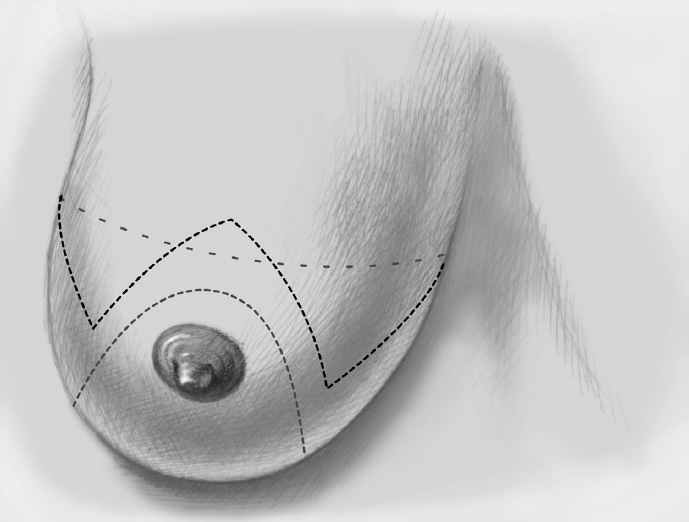
The classic B-technique with periareolar de-epithelialization extended laterally can be chosen to correct mild to moderate ptosis. The skin envelope is reduced centrally and in an inferolateral direction. Mastopexy is achieved by separating the upper part of the breast subcutaneously from the skin with fixation in a cranial direction.
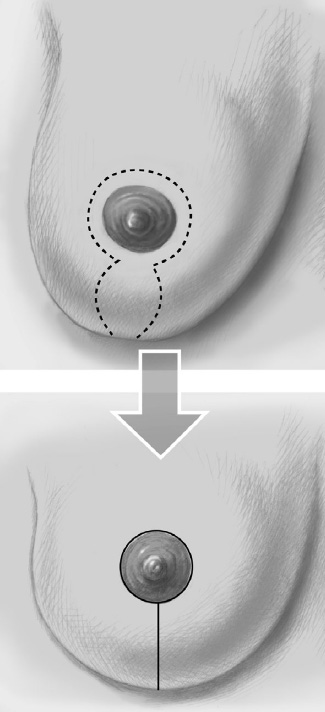
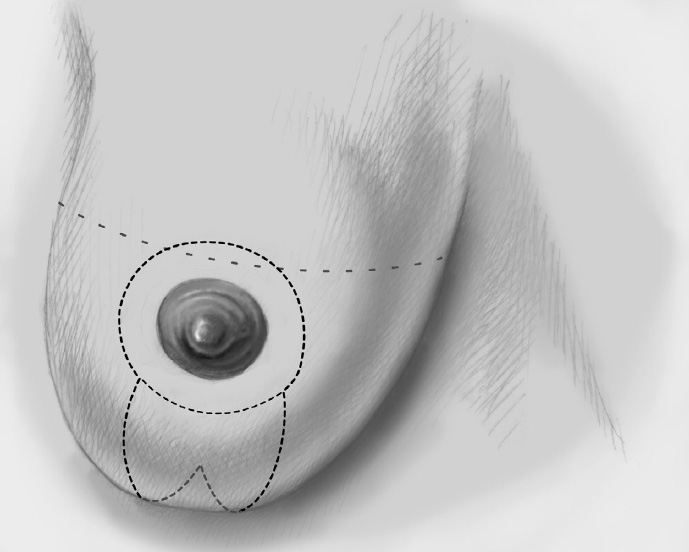
Periareolar de-epithelialization with vertical extension the 6-o’clock position (without T), essentially corresponding to the LeJour and Marchac reduction mammoplasty incisions, is also suitable for mild to moderate ptosis. In this case, the breast is divided in the midline below the nipple and dissected down to the pectoralis major. It is dissected free posteriorly and then lifted in a cranial direction.
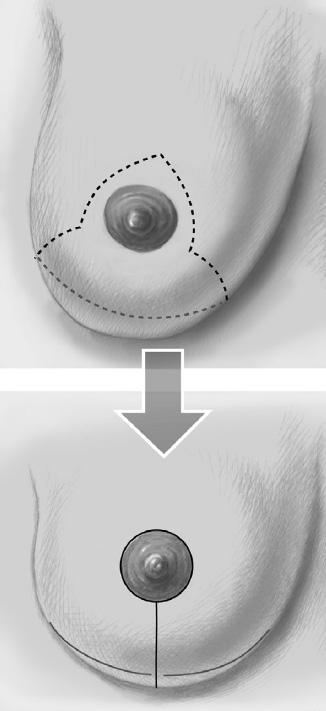
For severe ptosis, which is often associated with large heavy breasts and is therefore usually corrected as part of reduction mammoplasty, periareolar de-epithelialization combined with an inverted T (anchor shape) is the incision of choice. This allows the breast to be reshaped with maximum reduction of the skin envelope.
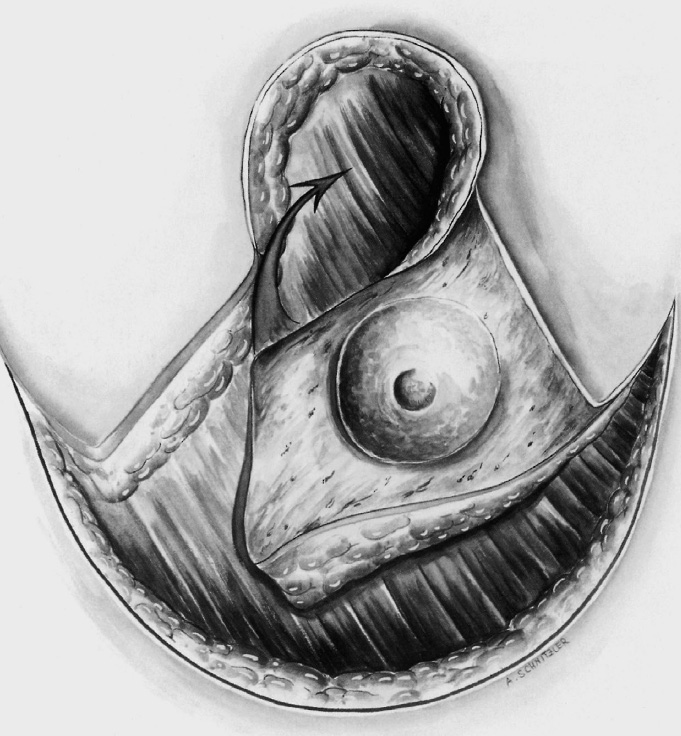
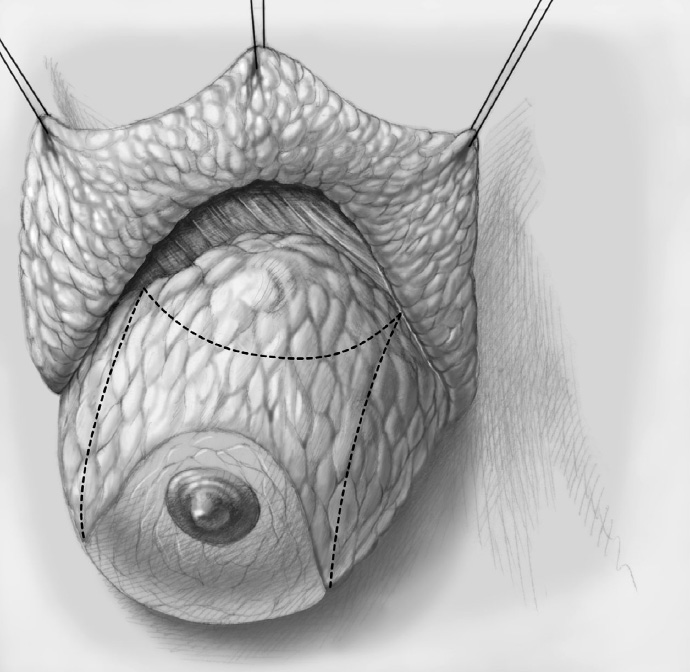
De-epithelialization is performed according to the chosen incision pattern and the skin envelope is separated from the breast (see Chapter 3.3.2).
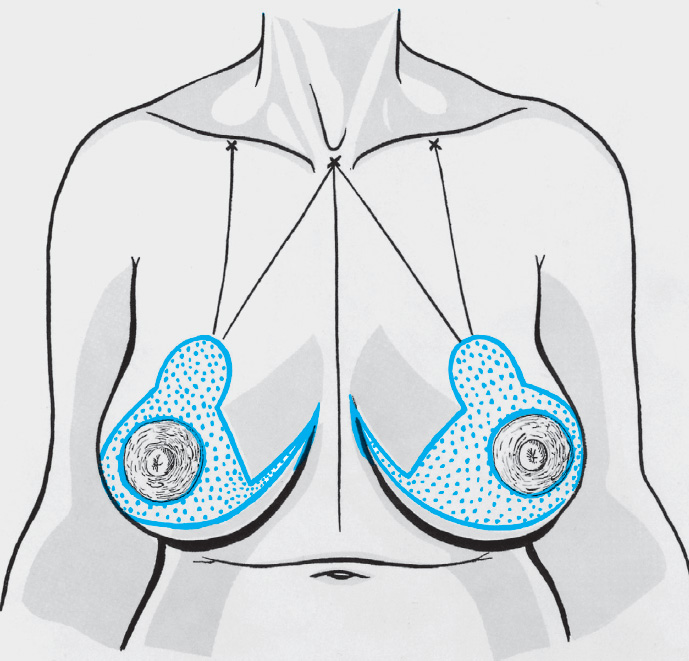
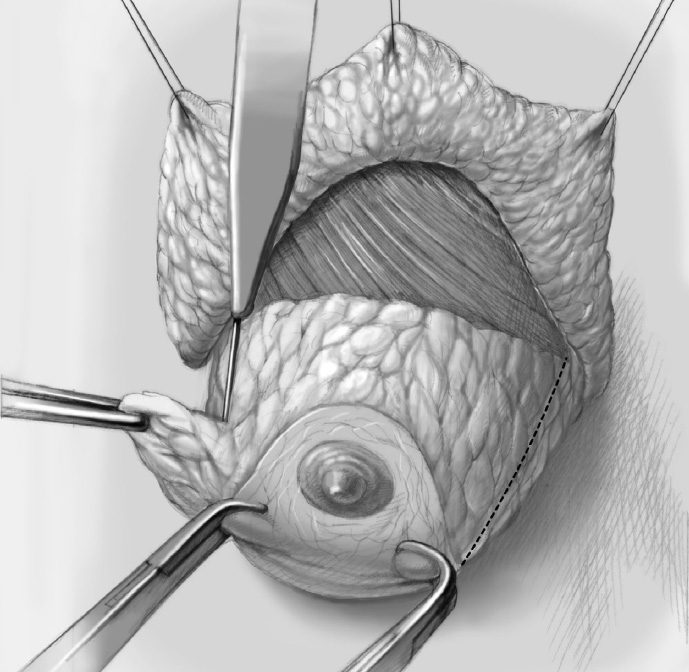
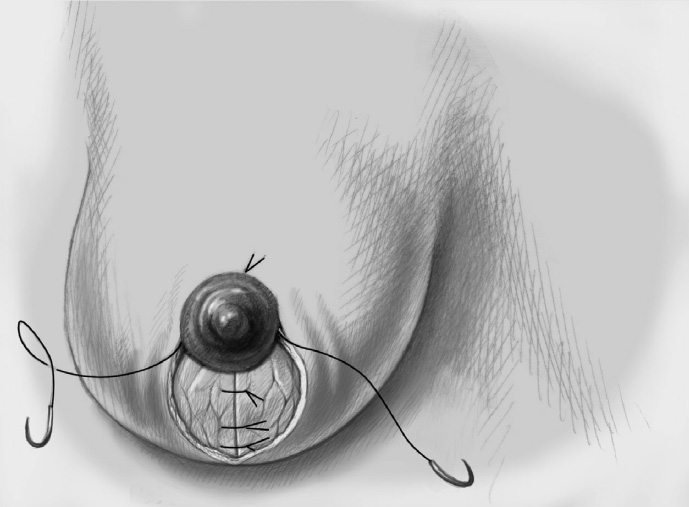
The breast is fixed to the chest wall.
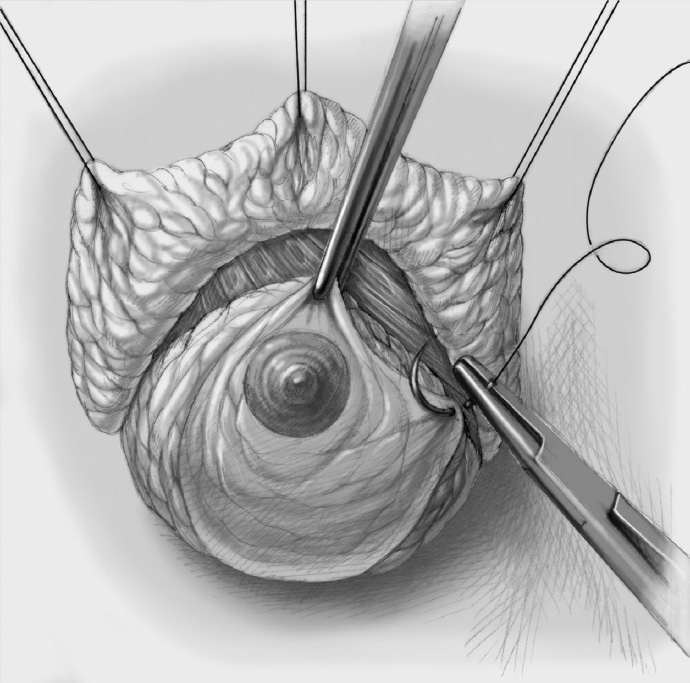
The tightened skin envelope is approximated subcutaneously and closed with an intracutaneous suture. Depending on the chosen technique or incision, a gathering suture in the vertical part of the incision (LeJour) or a periareolar purse string suture is necessary for approximation of the skin envelope.
Special Technique Mastopexy and Lifting
Complications
Secondary bleeding and impaired wound healing are rare complications (1–2%), with impaired wound healing occurring in both the skin and breast tissue.
The main complication is an ugly cosmetic result or rapid loss of the operative result as part of the continuing aging process or due to constitutionally “slack” connective tissue, which is often the cause of the marked ptosis in the first place.
An important complication will occur from the outset if the patient’s unrealistic expectations cannot be met even with the best operation technique. Open communication between surgeon and patient is important with all operations. This applies even more for cosmetic plastic surgery. A diplomatic “no” from the surgeon is better than a predictably unrealistic result.
Concomitant and Postoperative Treatment
Since the final outcome of the operation is only apparent after 8 to 12 weeks when healing is complete, the patient should be followed up over this period so that justified or unjustified dissatisfaction can be addressed and a need for surgical correction can be identified promptly. Follow-up examination a year after the operation is desirable.
Limits of the Methods
There has been much dispute about the pros and cons of cosmetic plastic surgery. However, there is no denying the significance of social pressures. If people are accepted as ultimately self-determining beings who make largely free and rational decisions, their desire for realization of the technical possibilities of cosmetic plastic surgery must be respected. The experienced surgeon must know when the patient is an unsuitable candidate.
3.3.2 Reduction Mammoplasty
Aims and Methods
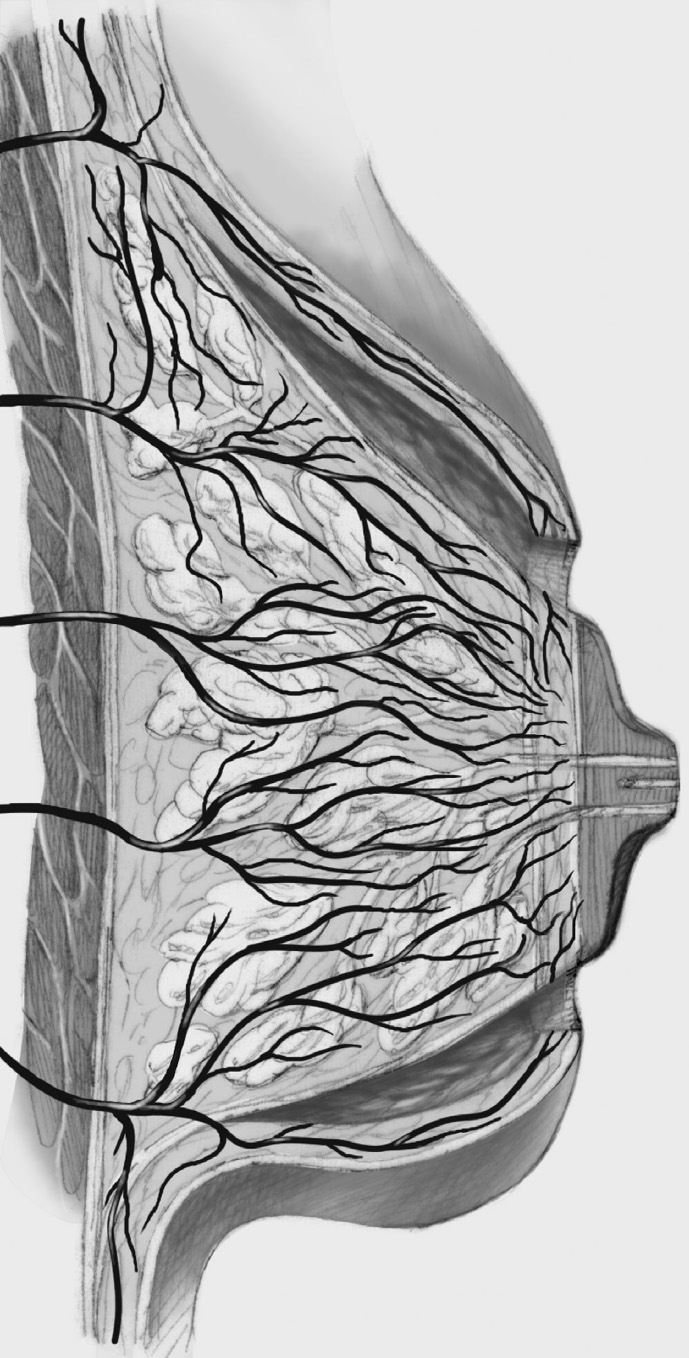
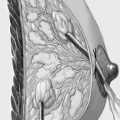
Importance of the operation. Unlike breast augmentation, which is very largely psychologically motivated, the desire for breast reduction in Europe and North America derives predominantly from a woman’s unhappiness with the size of her breasts and the resulting functional problems. Women with hypertrophic and ptotic breasts complain of a sensation of heaviness leading to physical and mental discomfort, grooves on their shoulders from the pressure of bra straps, poor posture, and pains in the neck and back. Unilateral mastectomy results in disability with regard to physical activity and sports and in difficulties with finding clothes that fit. Weight reduction usually leads to only a slight reduction in breast size. For all these reasons, compared with augmentation, breast reduction is much more a therapeutic procedure than a cosmetic operation. An important further aspect of breast hypertrophy is ptosis of the nipple–areola complex. Managing and/or transposing this nipple–areola complex is the main problem of the surgical techniques: to ensure an adequate blood supply and preservation of sensation following repositioning, the nipple–areola complex must remain on a tissue pedicle that maintains some of the intramammary and especially the subcutaneous blood supply, even after reduction of adjacent tissue.
Methods. The classic technique, rarely used nowadays, is the Strömbeck reduction mammoplasty, in which the nipple–areola complex is pedicled horizontally. The McKissock reduction mammoplasty, with a vertical (superoinferior) pedicle, is the origin of the techniques employed today. Reduction mammoplasty consists of two steps, which can be considered completely separately, even though they are generally performed together in certain combinations:
the skin incision, which adjusts the skin envelope to the new breast volume and prepares for the transposition of the nipple–areola complex, and
the nipple–areola complex pedicle relative to the resected parts of the breast, which significantly influences the blood supply of the newly positioned nipple.
The incision encompasses four basic techniques: the purely periareolar incision; the periareolar incision with lateral extension (B or L technique); the periareolar incision with vertical extension, also known as the perivertical or vertical incision (e.g., in the LeJour and Marchac techniques); and the periareolar incision with extension as an inverted T (“anchor” incision, e.g., in the classic McKissock technique). As regards the variations in the nipple–areola complex pedicle, the horizontal or lateral pedicle proposed by Strömbeck is used only rarely today. It has been superseded by the superoinferior McKissock pedicle or its recent variants, viz. the central, central-inferior, and superior pedicle. The classic (historical) approaches of Strömbeck and McKissock will be presented below, partly to provide a better understanding of these operations, which are difficult to visualize, and this will be followed by a description of current methods. The principle of the current methods is that intramammary tissue reduction can be combined with a range of techniques to reduce the skin envelope (Chapters 1.3 and 3.3.1). The main aim of most of the alternative incision patterns (see above) is to reduce the size of the resulting scar. The advantages of the classic technique combined with a superoinferior pedicle (largely corresponding to the McKissock method) are the good remodeling of the breast overall and the secure blood supply of the nipple. Any deviation in the form of a smaller skin incision demands more experience in breast surgery, as intramammary resection and remodeling are all the more difficult the smaller the access. In essence, the intramammary options include:
the central-inferior pedicle, where the breast tissue is reduced lateral, posterior, and superior to a central-inferior pedicle bearing the nipple,
the central pedicle, where a central tissue pedicle is divided completely from the skin envelope and reduced in circular fashion, and finally
the superior or central-superior pedicle, where the reduction is performed mainly in the inferior, central, and posterosuperior parts of the breast. With this technique, the pedicle is made mainly through the superior skin envelope, so it is not recommended for extreme macromastia with pronounced ptosis.
While the cosmetic surgeon usually adopts one or two breast reduction techniques, the different tumor locations in the breast require knowledge of the entire range of intramammary reduction techniques for tumor-adapted reduction mammoplasty.
Indications and Contraindications
Indications
Reduction mammoplasty is indicated for large and usually pendulous breasts of different shape (bell-shaped, saclike). The patient’s unhappiness on account of her symptoms is a further factor. The ptosis may be more or less severe. Mastopexy (breast lifting) provides adequate treatment for ptosis on its own. The very rare juvenile macro- or gigantomastia, excessive and often asymmetrical growth of the breasts during puberty, is a special indication. In this situation, reduction mammoplasty may be reasonable even before puberty is complete, though with the risk of a need for further reduction.
Contraindications
An elevated individual anesthetic risk and unrealistic expectations on the part of the patient regarding the cosmetic outcome are contraindications. Various medications, especially those containing acetylsalicylic acid and salicylates, increase the risk of bleeding and secondary hemorrhage (already increased by the large wound areas of the operation) and should be discontinued in good time. Pregnancy and as yet incomplete breast growth are classic contraindications. A relative contraindication is likely if the patient has not yet completed her family, as the ability to breast-feed can be impaired, depending on the technique. Pregnancy greatly alters breast anatomy. This must be made clear to a patient who is planning a pregnancy and wants breast reduction.
Operation Risks and Informed Consent
Because of the elective nature of the procedure, the patient must be informed in detail about all possible complications: bleeding and secondary hemorrhage, possibly with the need for transfusion with the resulting risks of hepatitis B and C and HIV infection, nerve injury, paresis, delayed wound healing, liponecrosis, impaired sensation, especially of the nipple–areola complex, the necessity of secondary operations, loss of the entire breast extremely rarely, scarring, an ugly cosmetic result, anesthesia incidents, and postoperative complications such as thrombosis, embolism, and death. Because of the medicolegal necessity of comprehensive information, the risks must be presented in the correct order. As health insurance companies may be critical, patients should also be informed of the possible financial consequences of complications due directly to the operation: many health insurers are no longer willing to pay for the treatment of complications of cosmetic surgery. Specific risks that must be made clear to the patient prior to breast reduction are impaired wound healing, which may lead to poor cosmetic results, development of broad hypertrophic scars, impaired nipple sensation, necrosis of the nipple (especially in the case of extreme macromastia) with complete loss of the nipple and the need for nipple reconstruction, and difficulty with or impossibility of breast-feeding. The patient must be aware that all of the listed complications occur much more often in smokers. Quitting smoking at least before and after the operation is highly advisable. If the patient wants to lose weight—which will naturally contribute to a lower complication rate—she should plan to do so before the operation as postoperative weight loss is more likely to impair than improve the final cosmetic result and may lead to recurrence of the breast ptosis.
Operation Planning
Preparation for all cosmetic operations follows a similar pattern:
Medical history, clinical examination to assess the anatomy
Inspection, palpation, exclusion of breast disease requiring direct treatment
Exclusion of clinically occult breast cancer by age-appropriate imaging (mammography, ultrasonography)
Particularly in the case of severe macromastia, intertrigo and fungal infections should have been treated preoperatively by consistent therapy and consistent drying.
Detailed discussion with the patient about her motives, wishes, and expectations. The risk (including medicolegal risk) of a dissatisfied and litigious patient postoperatively is particularly great when expectations are unrealistic. A psychological assessment may be warranted. However, because of their suffering over many years, patients who have had breast reduction are usually among the most satisfied patients postoperatively.
Detailed demonstration of the situation with explanations for the patient: degree of ptosis, asymmetry, chest wall anatomy and its importance for breast contour, differences in size. Make a photographic record (which forms part of every cosmetic operation). The patient often notices obvious but long-standing asymmetry only postoperatively. Careful preoperative discussion can help to avoid major postoperative problems.
Discussion of different surgical techniques with illustration of potential results using photos. Ideal, average, and less successful results should be presented. The patient should have seen pictures of the most important complications.
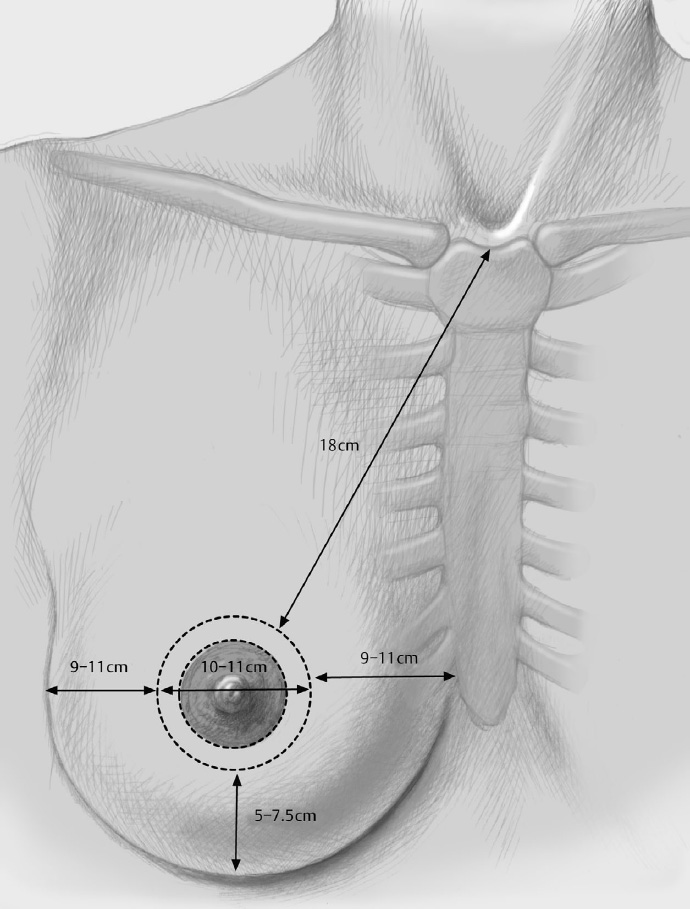
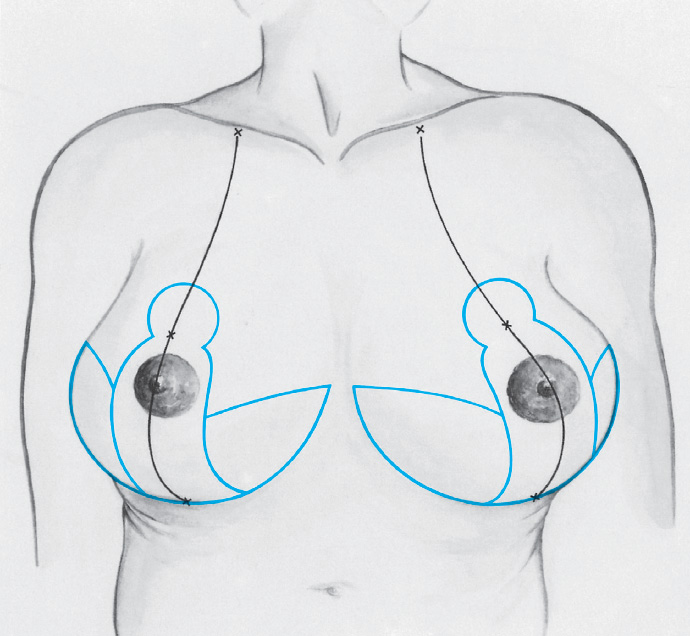
Even more than with other cosmetic operations, reduction mammoplasty requires careful measurement and assessment of the breast, taking certain guidelines into account for the reconstruction. The upper border of the (new) nipple–areola complex should be about 19 to 21 cm from the sternal notch (up to 23 cm with severe macromastia) and be roughly in the midclavicular line, that is, 7 to 9 cm lateral to the center of the sternum. The lines connecting the nipple–areola complex on both sides and the sternal notch should roughly form an equilateral triangle. The lower border of the areola should be at the level of the submammary fold, that is, 5 to 7 cm from the chest wall. The (new) nipple–areola complex should have a diameter of about 4 to 5 cm. With these measurements, depending on the patient’s age, the nipple–areola complex will be at about the level of the middle of the upper arm (young patient), or a little lower down (two-thirds, older patient).
Although these “optimal” breast dimensions, which can be found in many textbooks, provide a certain framework for action, they are targets that should ultimately be attained only after the healing process is complete. The experienced surgeon knows that a particular danger in breast reduction is a nipple that is finally too high. Because of the postoperative retraction of the skin envelope (especially in the younger patient), it may make sense in an individual case to position the nipple somewhat lower when marking preoperatively.
The extent of the operation, convalescence, and all possible complications are explained.
Discussion of the financial aspects. A report is prepared for the health insurer and if necessary attending the health insurer’s medical assessor may be arranged.
Consent to the procedure
Anesthesiological preoperative investigations depending on the patient’s age and local practice
Thrombosis prophylaxis: low molecular weight heparin
Antibiotic prophylaxis: first or second generation cephalosporin
Difficult surgery: takes 2 to 4 hours; surgeon and one assistant
Anesthesia and Positioning
Special Instruments
Breast set: scalpel, fine dissecting scissors, electrocautery knife, electrocautery needle, skin hooks, abdominal towels
Procedure
Preparation
The marks are drawn with the patient standing, the day before or immediately prior to operation.
If a bladder catheter is not placed, the patient should go to the toilet before transport to the operating room.
The patient is identified in the pre-op and operating room: file and patient match, patient confirms the planned operation according to the entry in her file and the preoperative marking.
Intubation versus laryngeal mask
Positioning: semi-sitting positions are favored by many surgeons, as in oncoplastic surgery. The arms are abducted bilaterally and secured adequately. Partially elevating the patient is required in every case. Some surgeons demand mobile arms.
Skin preparation, sterile draping: thoracic access
Some authors recommend injecting local anesthetic and vasoconstricting substances to improve hemostasis and also to facilitate intramammary dissection. If this injection is given, it must be ensured that an identical volume is injected on both sides.
Operation
Reduction Mammoplasty—Strömbeck Method—Horizontal Pedicle
The Strömbeck method, now virtually obsolete, is presented here to facilitate a better conceptual understanding of modern techniques.
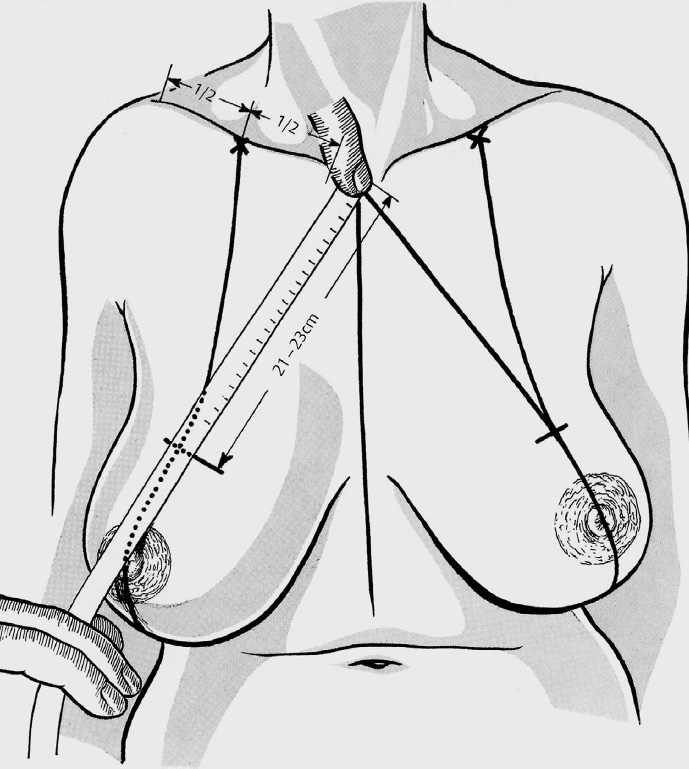
The new nipple position is determined with the patient standing and with her arms hanging down. It is on the line joining the middle of the clavicle and the nipple at the level of the submammary fold, which is 20 to 22 cm (19–25 cm) from the sternal notch, depending on height.
The outlines of the new nipple–areola complex and lateral skin flaps are drawn, freehand or using a template, with the midline of the template on the midclavicular–nipple line. The height of the skin flaps is 5 to 6 cm and this gives the distance from the areolar border to the submammary fold.
The submammary fold is drawn, checking that the medial and lateral skin flaps are long enough to meet in the middle of the submammary fold. If the two skin flaps do not meet in the middle, they must be extended accordingly, with only the lower corner of the skin flaps displaced toward the midclavicular line.
A line is drawn from the medial to the lateral corner of the wound, running parallel to the submammary fold and a little below the areola. The skin above this line is de-epithelialized as far as the limit marked by the template, sparing the nipple–areola complex.
The tissue below this line is excised as far as the submammary fold. If the breasts are not too big, according to the original method the two upper corners of the skin flap and the two lower corners are joined directly by lines curving downward.
The circular region of the new nipple position is excised with the subcutaneous fat and breast parenchyma down to the pectoralis muscle. The advantage of this approach is that the de-epithelialized bridge between the two skin flaps and the nipple can be incised superficially and can therefore be mobilized better.
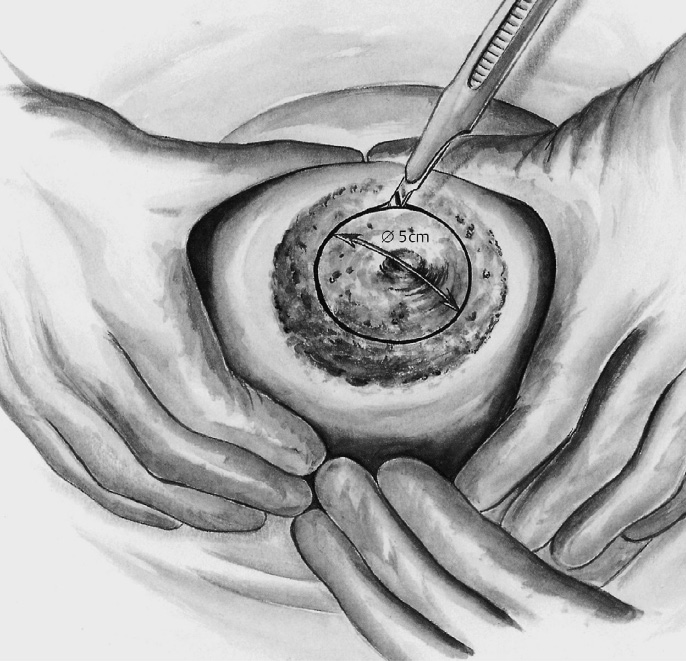
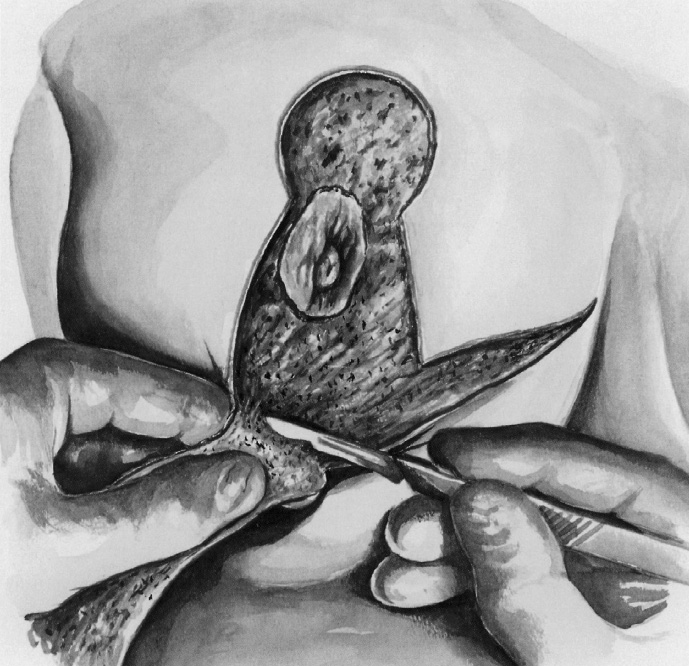
The skin is de-epithelialized: The incision line of the slightly enlarged areola is marked with a round template or nipple ring (diameter 4–5 cm) and incised superficially. The breast is tensed by the assistant’s hands or by tying a tourniquet around its base. After incising the other lines into the dermis but not into the subcutaneous tissue, the keyhole-shaped pattern is de-epithelialized, sparing the nipple and the two side corners.
Excess tissue is resected: The lines between the lateral and medial corners of the wound below the nipple and in the submammary fold are incised down to the pectoralis fascia. The tissue in between is removed. After this, the upper part of the breast is elevated and divided from the pectoralis fascia.
Further glandular tissue on the underside of this flap is excised if necessary with a scalpel or scissors. The removed tissue is weighed and compared with that of the other side. This allows breasts of different sizes to be balanced.
Nipple transposition: In the original method, a round or elliptical cylinder of tissue is excised from the skin to the pectoralis fascia at the site of the new nipple. However, there is also a variant without “upper resection.” In this variant, the dermis is incised vertically at both skin flaps and in the lower part of the new nipple bed. This way, the nipple retains an additional upward connection for its blood supply. It is invaginated when the nipple is transposed. The skin must be mobilized for about 1 to 2 cm around the incision, and also the de-epithelialized dermis in the region of the new nipple position.
After careful hemostasis and approximation of the lower corners of the skin flaps with a towel clip, translocation of the nipple into its new position without force is tested. If this appears to be possible, the lower corners of the skin flaps are fixed to the corresponding site in the submammary fold with an intradermal suture (Vicryl 2–0). Otherwise, the skin is mobilized further around the incision.
A suction drain is placed in the wound cavity behind the breast. The upper corners of the skin flaps and the nipple are then fixed at four points by intradermal sutures (Vicryl 3–0).
The wound edges are approximated by several subdermal interrupted and continuous sutures depending on tension. The skin is closed by intracutaneous sutures in the vertical wound and submammary fold and the nipple is sutured in place with fine nonabsorbable interrupted sutures (monofilament, 4–0).
Modification: The lateral bridge of dermis is divided. If the nipple cannot be readily translocated to its new position in the original method with “upper resection,” the dermis can be incised superficially in the two skin flaps or the lateral bridge can be divided completely provided that the medial flap is wide enough for the blood supply. This is the case particularly when the “lower resection” starts not from the lower corners of the two skin flaps but from the medial and lateral wound corners.
The classic form of the Strömbeck technique is used rarely nowadays. Important disadvantages were the postoperative horseshoe shape of the reduced breast and a relatively high rate of nipple necrosis. However, the technique lives on—for example, in the form of a superomedial pedicle.
Reduction Mammoplasty—McKissock Method—Superoinferior Pedicle
The classic McKissock method is nowadays rarely used in this form. However, it represents the foundation for the various inferosuperior pedicle techniques employed today.
The preoperative planning is the same as that for the Strömbeck reduction mammoplasty. After determining and marking the new nipple position with the aid of a template or appropriately bent wire, the level of the medial and lateral skin flaps, which should be 5 to 6 cm in length, is measured and marked.
The lower corner of these skin flaps is moved somewhat toward the center of the breast so that the 5–6-cm central boundary lines of the skin flaps diverge only slightly inferiorly, that is, they run almost parallel in a superoinferior direction. These boundary lines are extended inferiorly as far as the submammary fold.
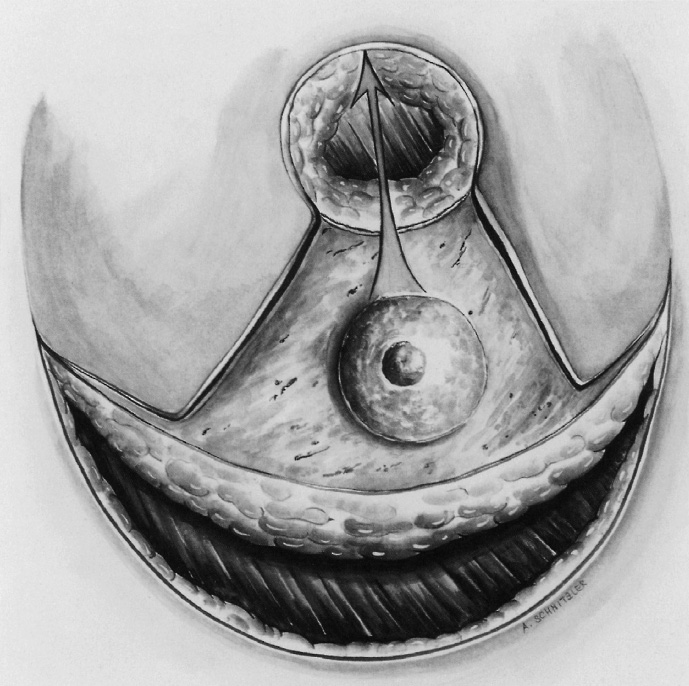
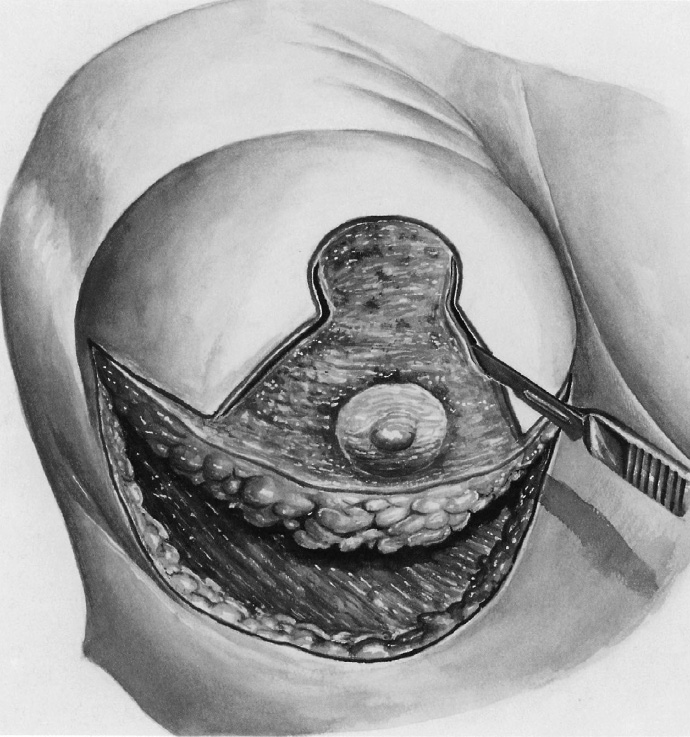
The keyhole-shaped pattern is de-epithelialized, sparing the nipple and areola (diameter 4–5 cm), and the two triangles medial and lateral to this are excised. The medial incision line starts within the new areola boundary line at about the 2-o’clock position and is continued downward as far as the submammary line.
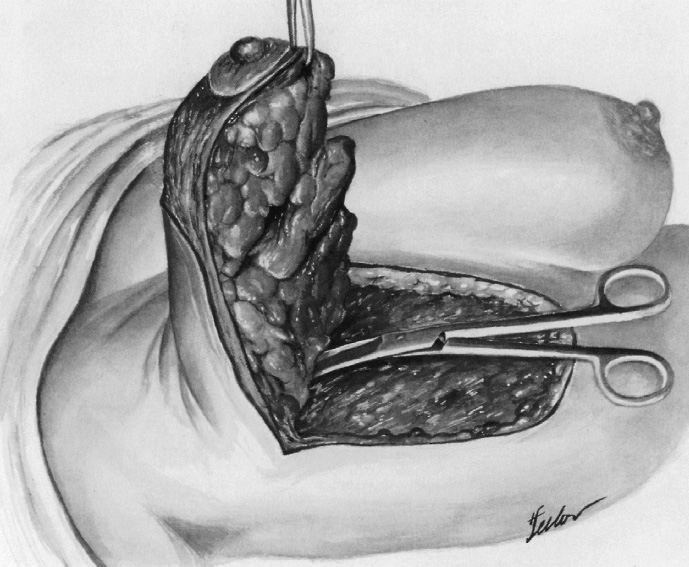
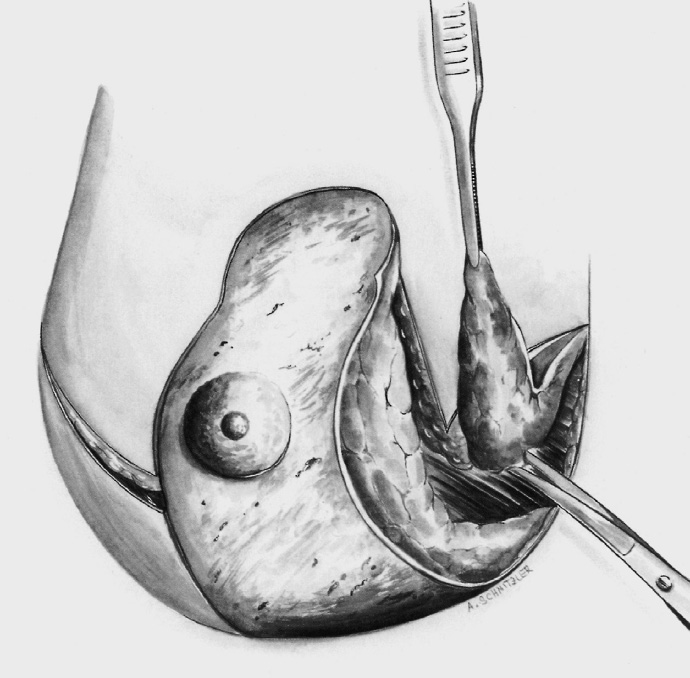
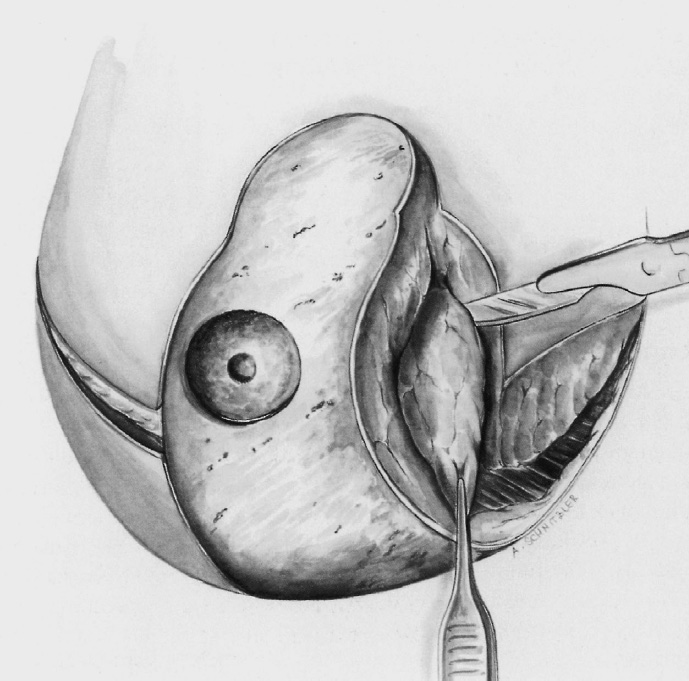
The medial triangle is removed down to the pectoralis major. Bulging breast tissue at the boundary of the medial flap is excised. The lateral longitudinal incision of the vertical de-epithelialized pedicle begins at the 10-o’clock position. When resecting the lateral triangle, a thin layer of fat and breast parenchyma is left on the muscle so as not to destroy the vessels and nerves coursing on the pectoralis fascia from laterally.
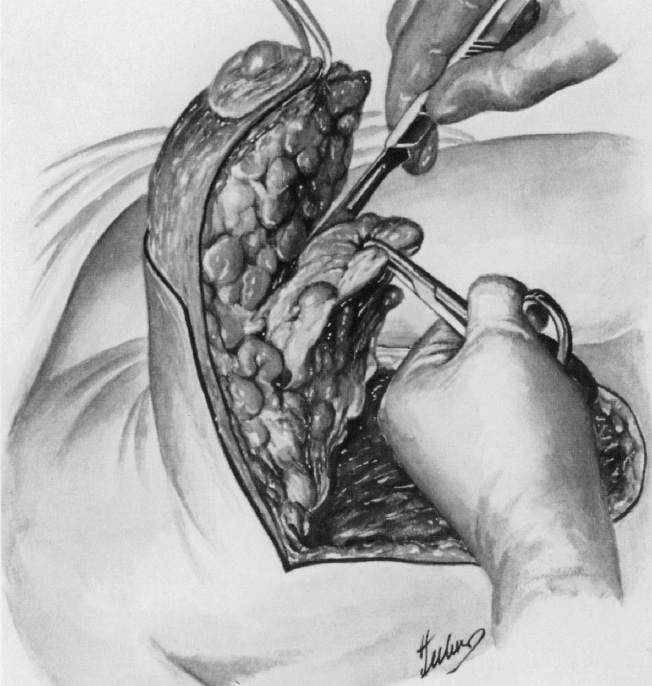
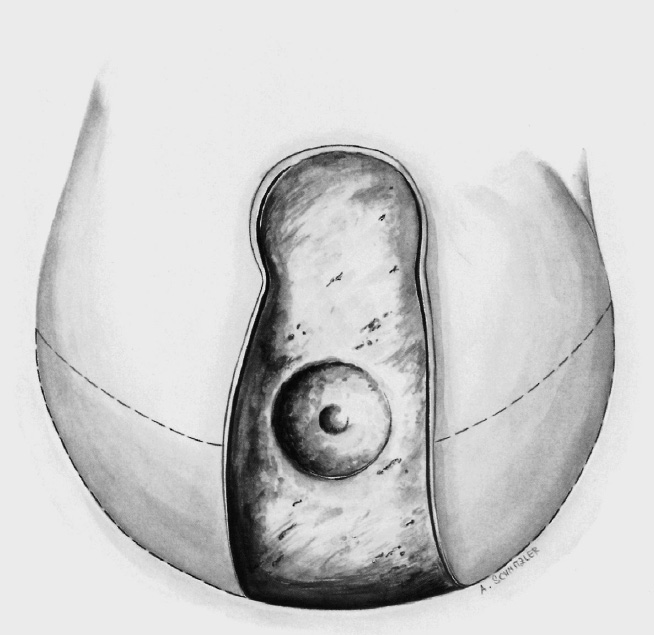
The lateral flap of breast tissue and skin is thinned to a thickness of roughly 2 cm, likewise leaving a thin layer of tissue on the pectoralis muscle. Following bilateral resection, the entire length of the vertical pedicle with the nipple is still connected to the chest wall.
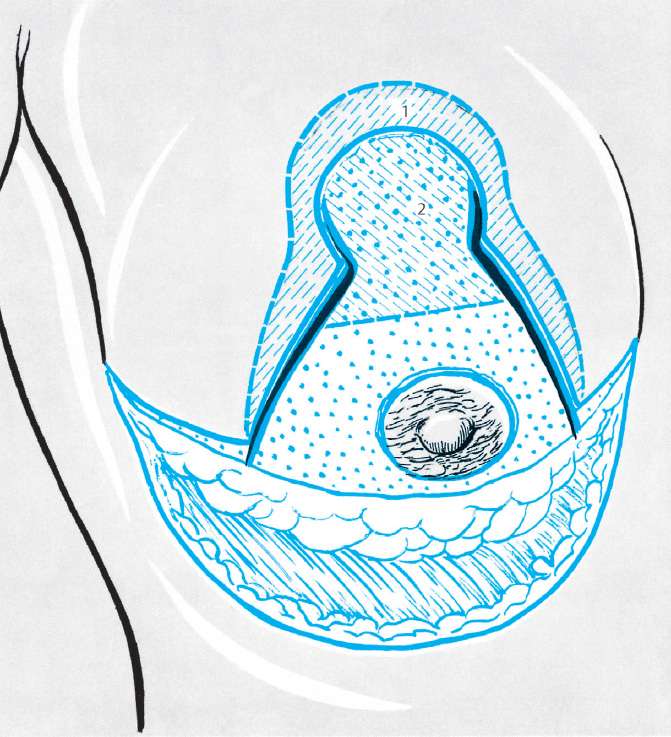
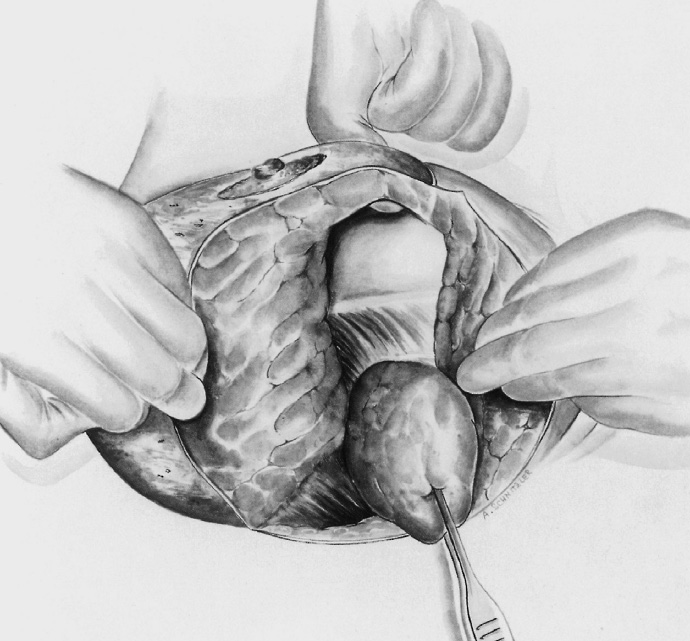
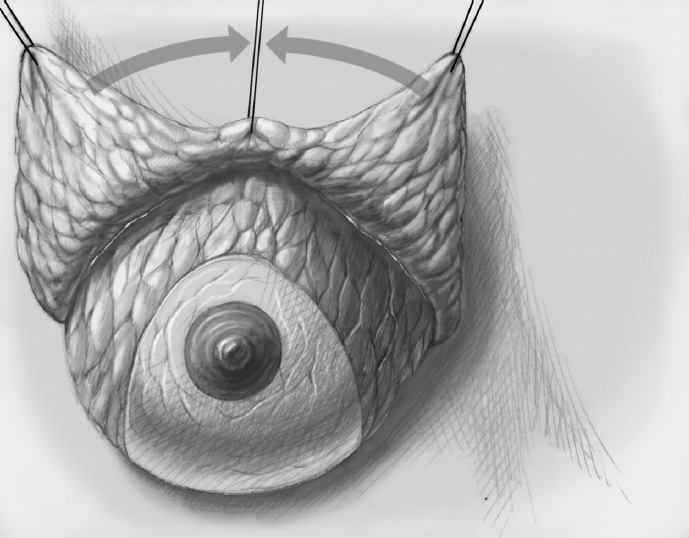
“Central resection”: A triangle of fat and breast tissue is excised from the vertical pedicle so that the cranial part of the pedicle can be folded beneath the new nipple position. The inferior boundary of this triangle extends roughly to the upper border of the areola, and the superior boundary to the boundary of the new areola position.
The thickness of the tissue beneath the new de-epithelialized areolar surface is about 1.5 cm. It is important that as much as possible of the remaining base of the vertical pedicle remains connected to the chest wall.
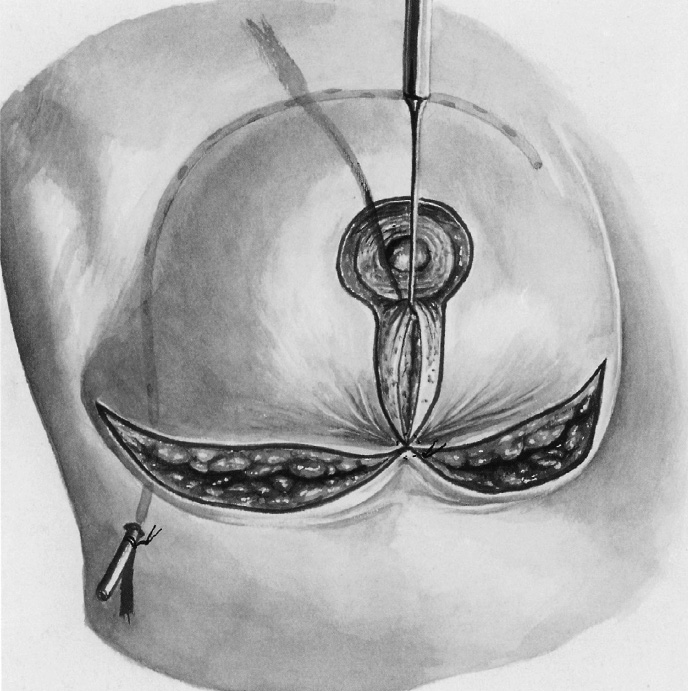
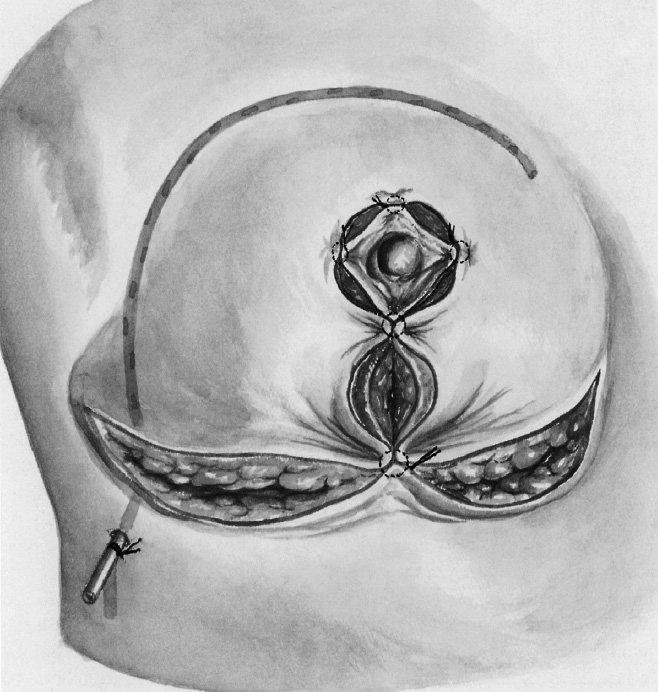
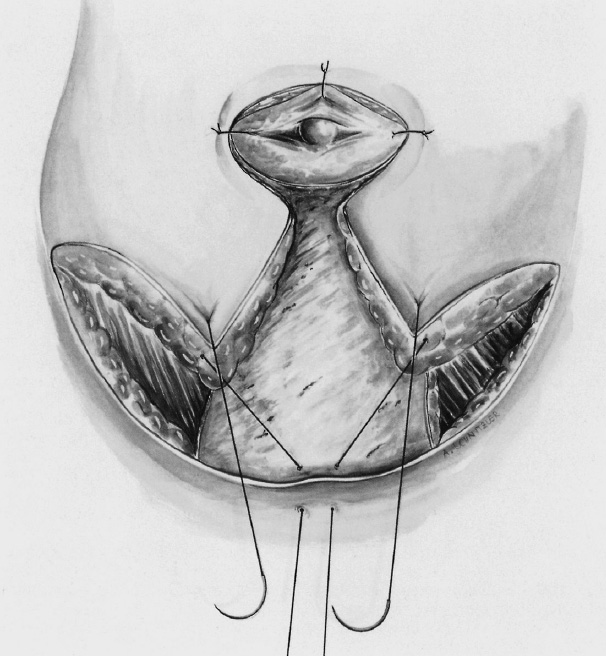
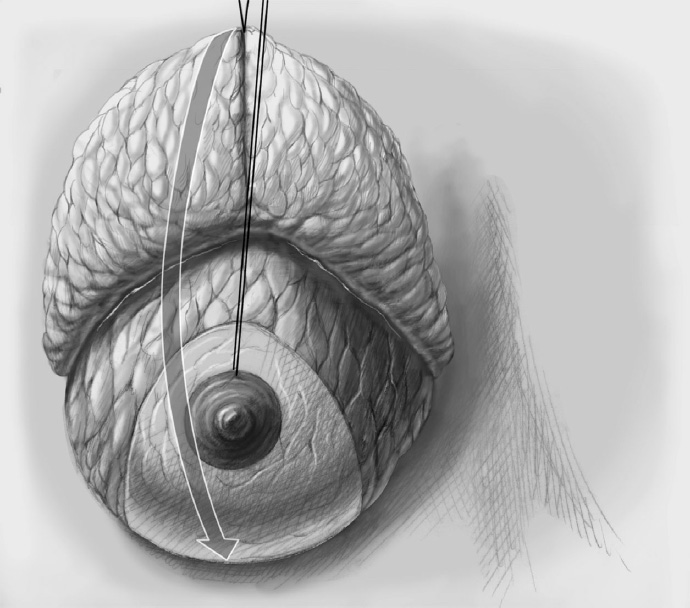
After insertion of a suction drain through a separate stab incision outside the operation wound, the upper part of the vertical pedicle is folded and the areola is fixed in its new position with retaining sutures. The medial and lateral flaps are joined over the inferior part of the vertical pedicle. They are first approximated by temporary positioning sutures and shortened if necessary. Finally, the wounds are closed by continuous intracutaneous sutures.
Central-Inferior Pedicle
This is regarded as a particularly safe method and is therefore suitable also for smokers and elderly postmenopausal patients where perfusion is impaired. Because the breast volume can be reduced by more than 50%, the method can also be employed for very large breasts.
The incision pattern corresponds to an inverted T, with the inferior pedicle (which will be de-epithelialized) kept somewhat broader (as a guide, the scalpel shaft length is approximately 8–10 cm) because this bears and nourishes the nipple–areola complex without an additional superior pedicle.
The new nipple position anteriorly is established initially only by impingement of a finger in the submammary fold but without yet excising the nipple. Caution: Because of the frequent postoperative retraction of the reduced skin envelope, which is now relieved of its weight, the new nipple may come to lie too far superiorly if the surgeon keeps too strictly to the distances recommended in the literature and too little to the individual situation.
To avoid excessive tension of the skin envelope, especially in the region of the submammary fold, it is advisable to make the limb lengths longer than 7 cm (approximately 9–10 cm) and resect the resulting excess skin later (prior to skin approximation). The nipple position too should only be established after approximation of the submammary sutures to avoid a position that is too far cranial.
The long-term target distance between the nipple and submammary fold is about 7 to 8 cm and the distance between the sternal notch and nipple is 19 to 23 cm. The described procedure is intended to achieve these classical dimensions in the long term, following wound healing and skin retraction.
Following the skin incision, the superior skin envelope is dissected off the breast; that is, it is separated from the breast parenchyma in a cranial, medial, and lateral direction.
The breast is resected, mainly in the upper outer part, and somewhat less in the superior and medial part. It is important to leave enough breast tissue behind the areola and in the cranial part as otherwise projection of the areolar region will be poor after it is sutured. Tissue can additionally be resected to right and left of the inferior pedicle.
The skin envelope is approximated subdermally in the region of the vertical limb in preparation for reconstruction of the reduced breast with fixation of the breast on the chest wall and repositioning of the nipple.
The breast is fixed to the pectoralis muscle to avoid postoperative lateral deviation of the “new” breast. The de-epithelialized dermis covering the central-inferior pedicle is sutured to the muscle superolaterally and superomedially with absorbable sutures (Vicryl 0, 2–0). It is useful to place the new breast behind the skin envelope after pulling this down, as this allows the optimal position on the chest wall to be determined.
The skin envelope is again peeled off the breast inferiorly and excess inferomedial and especially inferolateral skin is resected.
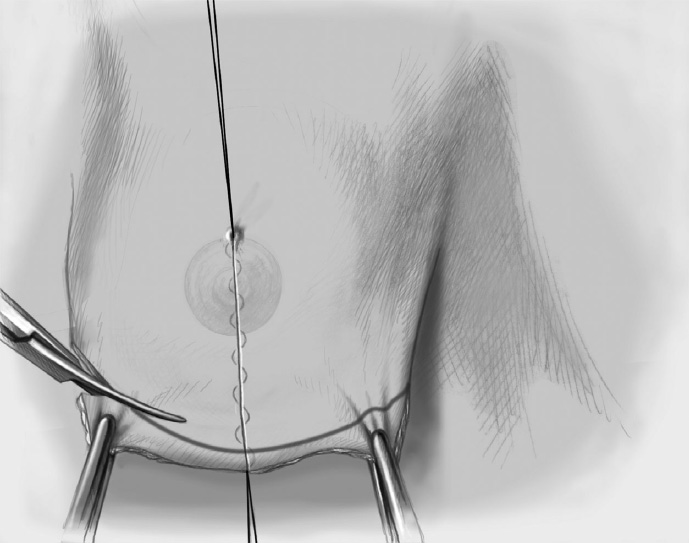
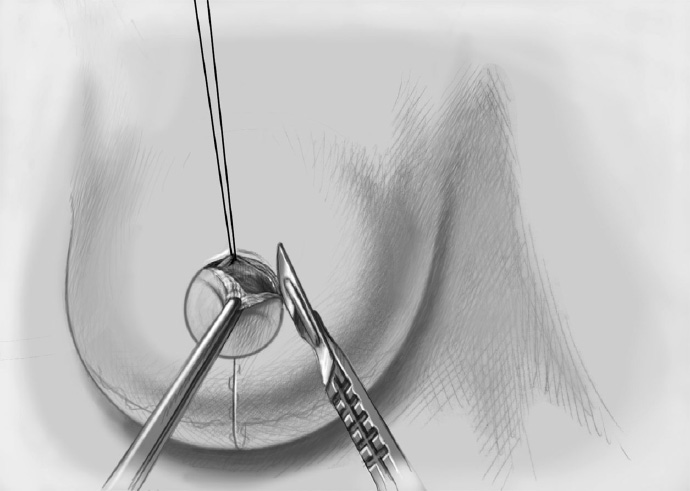
After determining the final position of the nipple–areola complex, the marked area of skin is excised exactly over the nipple. To facilitate positioning, a retaining suture can be placed in the nipple at the 12 o’clock position; this also allows assessment of the tension acting on the nipple (e.g., due to internal fixation). Following skin excision, the nipple can be readily guided to its new position with the retaining suture.
A drain is inserted and the skin is closed in two layers.
Surgeons’ postoperative dressing preferences vary greatly.
Central Pedicle
The central pedicle is usually combined with a periareolar incision to reduce the skin envelope but can also be used with a vertical incision and inverted T. The method assumes good vascularization overall, along with an elastic skin envelope that can shrink (because of the problem of “excess” skin in the suture area). Up to 50% of the breast volume can be resected. The technique is more suitable in young women.
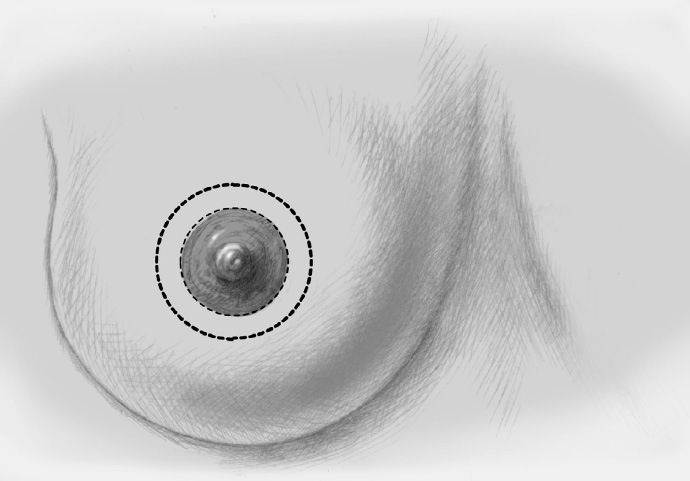
The first step following marking is periareolar de-epithelialization.
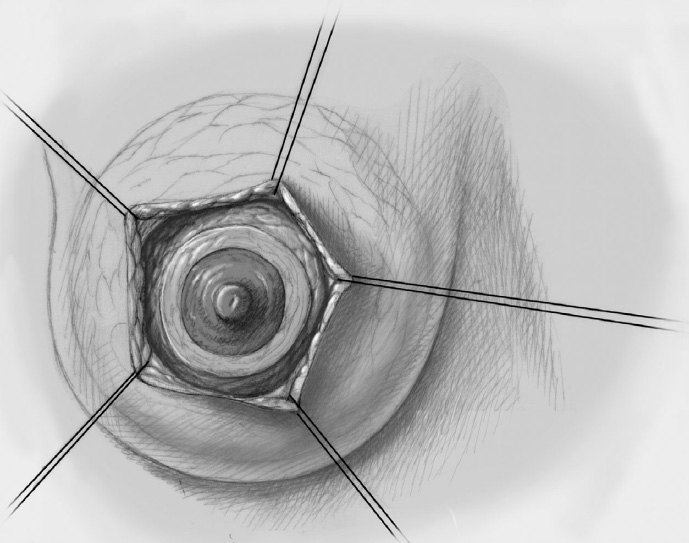
The breast is exposed in a pyramidal shape, starting from the widely deepithelialized ring, by dissecting off the skin envelope in a circle. The skin is divided from the breast in a superior and inferior direction leaving a subcutaneous fat layer of about 1 cm.
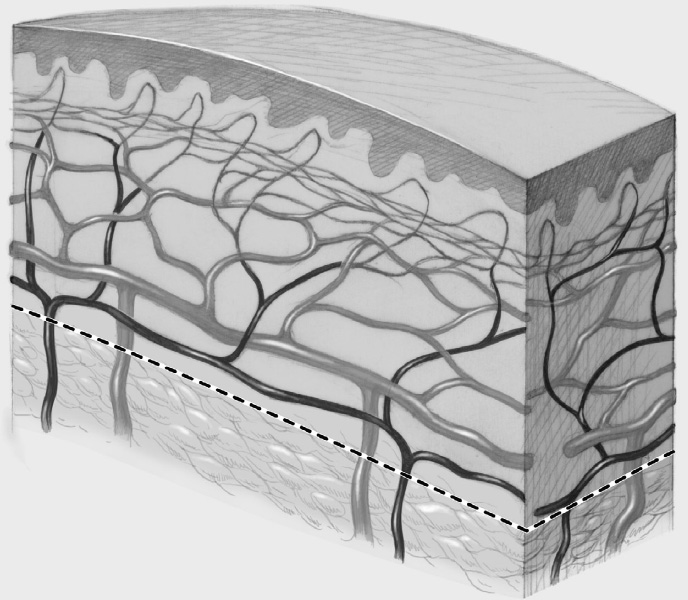
Some authors recommend not dissecting this layer down to the pectoralis fascia to protect the nerves and vessels on the chest wall. However, exposure of the pectoralis muscle makes sense for modeling the breast. The perforating vessels at the periphery entering the subdermal plexus, some of which emerge from the muscle, must on no account be injured.
The central part of the breast is reduced circularly, with the main volume of resection in the upper lateral part.
For internal modeling it is recommended to reshape the reduced breast with interrupted sutures and fix it to the chest wall, especially medially, laterally, and cranially.
As in all reduction mammoplasties, insertion of suction drains is recommended. The inferior part of the wound in particular should be drained for a sufficiently long period as premature removal of the drain can lead to seroma formation and delayed wound healing.
The larger outer skin ring is approximated to the smaller inner ring. A gathering subdermal purse string suture is placed along the outer ring, allowing it to be largely adjusted to the smaller inner ring. This is followed by the normal two-layer approximation. The excess skin shrinks well if the skin is sufficiently elastic.
The technique can be modified by a periareolar incision with segmental (medial or lateral) or vertical extension (downward). This extension is recommended as soon as the diameter of the periareolar ring becomes greater than 10 cm as extreme creasing of the skin persists even after healing above this ring size. The segmental or vertical extension and skin resection make the ring smaller and produce additional skin tightening.
Superior Pedicle
This versatile technique can be used for mild to moderate macromastia.
Marking is particularly demanding with this technique as tightening the skin along the vertical axis (midclavicular line) decides the final breast contour. The new nipple–areola complex cannot be planned as exactly preoperatively as with a central-inferior pedicle.
The incision is usually periareolar and vertical or perivertical. The subsequent operation is also known, with slight variants, as the LeJour technique, and as the Marchac technique when the extension is in the form of a small inverted T.
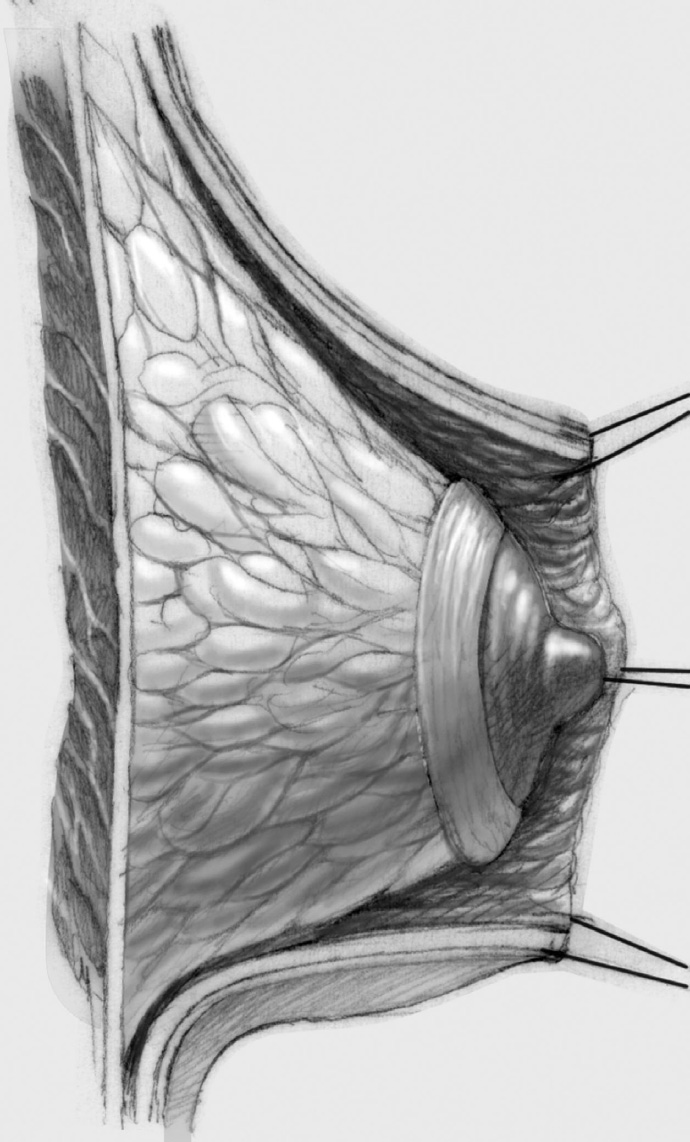
The inferior and centroposterior breast is resected mainly. Dissection is continued down to the pectoralis major, elevating the residual breast in a cranial direction. In a final step, resection is performed “retrograde” in the upper part of the breast also, which is important for the final shape of the breast.
The nipple is repositioned at the most superior point of the appropriately measured de-epithelialization pattern. If repositioning of the nipple over a long distance is necessary, an upward domelike extension of the deepithelialization above the nipple is possible (LeJour technique).
Free Nipple Transplantation
When the breasts are very large and ptotic, transposition produces a risk of nipple necrosis. Free nipple transplantation is therefore better. Free nipple transplantation is employed in women with a very large resection volume where the nipple–areola complex has to be elevated more than 15 to 20 cm, especially if there are additional risk factors for perfusion (postmenopause, breast involution).
Because of the usually severe macromastia, a central-inferior pedicle with classic resection pattern (inverted T) is usually employed. The pattern is marked accordingly and the new nipple position is determined.
The nipple is removed as a full-thickness flap.
The vertical boundary of the two skin flaps is divided during tissue resection. These division lines are elevated to the region of the new nipple position so that a triangle is removed from this region that corresponds to about one-third of the area.
The new nipple position is de-epithelialized.
After closure of the wound edges, the nipple is sutured into its new bed.
Special Technique Reduction Mammoplasty






Complications
Impaired wound healing: This is the most important complication and is often associated with wound infections (3–5%). Perioperative antibiotic prophylaxis is standard and many surgeons cover the patient with postoperative antibiotics also. Impaired wound healing occurs especially at the lower end of the vertical wound (frequency 13–15%), particular if the skin is under tension.
Wide scars and hypertrophic scars: A particularly common (15–20%) “complication” that is especially troublesome cosmetically is the development of wide scars. Smoking and wound approximation that is not tension-free are predisposing factors. The use of monofilament sutures in the skin helps to minimize impaired wound healing, which also promotes the development of wide scars. Wide scars occur more often in young women.
Postoperative bleeding and hematomas: These sometimes require surgical revision and in turn increase the risk of wound infection.
Loss of nipple sensitivity: More or less marked impairment of nipple sensitivity was reported by up to 50% of patients, with 7 to 16% reporting significant reduction.
Nipple necrosis: Total necrosis is observed in fewer than 2% and partial necrosis in up to 5% of patients.
Fat necrosis: The frequency is 2 to 5% but up to 10% in very obese women. Probably due to hypoxia as a result of impaired perfusion, the fat liquefies, often with pyrexia, and perforates spontaneously through one of the lower sutures and leaks if it is not drained. To avoid a fistula that may take months to heal, it is advisable to open the necrotic cavity and remove the necrotic tissue. Indurated nodules arise from small areas of fat necrosis, which are gradually absorbed, but they may persist and become calcified.
Blood loss: On account of the extensive dissection surfaces, blood loss can be relatively high. However, the need for perioperative transfusion has diminished greatly in recent years through improved surgical techniques, use of electrocautery, and immediate hemostasis by electrocoagulation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


