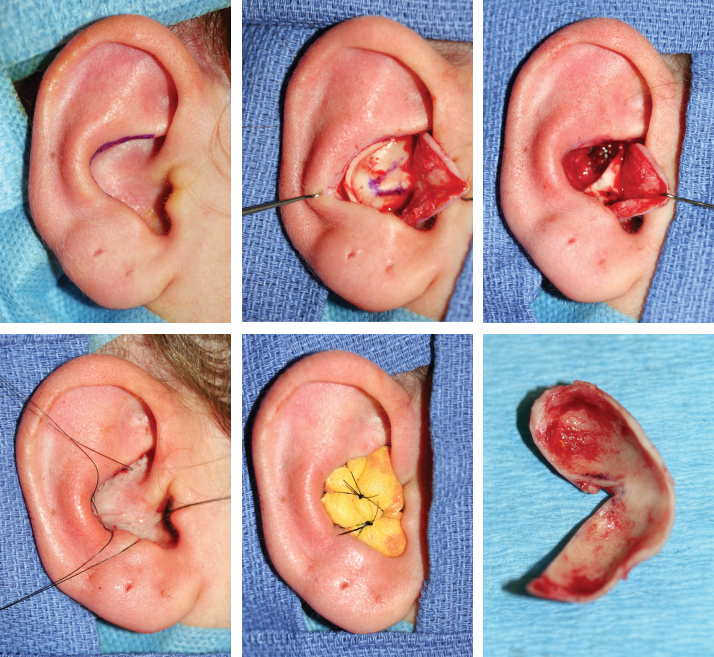
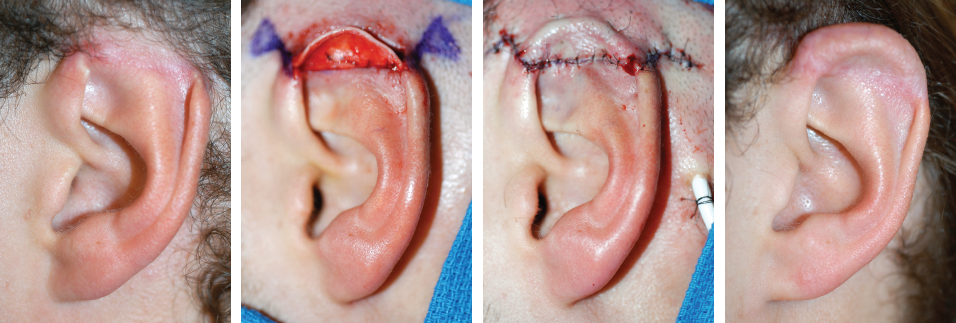
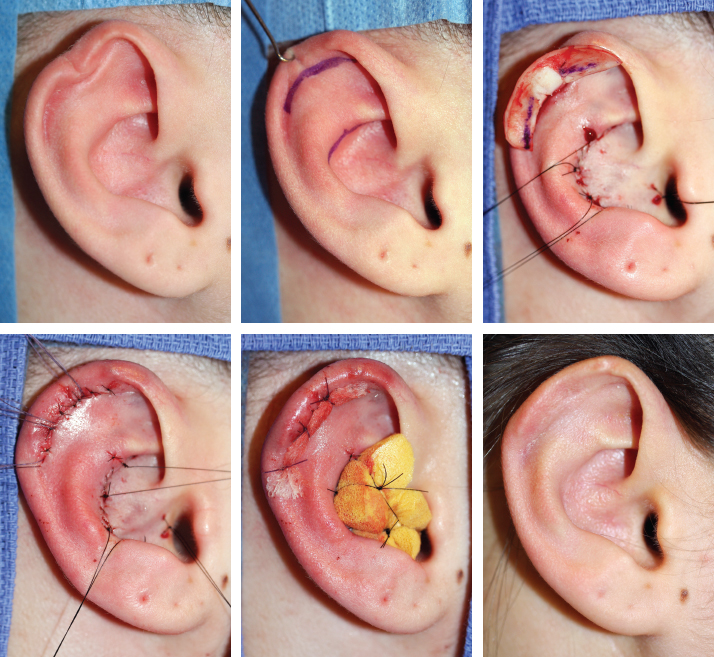
CHAPTER 12 With the principles for partial ear reconstruction in mind, analyzing the defect, choosing the best support, and deciding if the surgery will be done in one or two stages are straightforward. The complete operative plan can be decided in the first preoperative consultation (see video 12-1). Reconstruction with costal cartilage will be selected with the following rule in mind: Fibrocartilage harvested from the conchal bowl can only be used when the defect involves no more than a quarter of the ear and no more than two adjacent planes (see Chapter 11). Conchal fibrocartilage can be harvested through a posterior or anterior approach to the conchal bowl. Except in cases requiring a posterior approach for a specific reason (that is, previous scars or particular contours to correct), the anterior approach will allow better exposure of the conchal bowl, easier dissection, preservation of the root of the helix, and effective placement of bolster sutures in the concavity of the concha. The anterior skin incision follows the antihelix in the upper part of the posterior wall of the concha. Other than the root of the helix, the entire floor of the conchal bowl must be harvested, even in cases where it will not be entirely used. This is very important, because it will prevent residual irregularities. The root of the helix and the posterior lining of the auditory meatus must be preserved to prevent stenosis at the entrance of the canal. Bolster sutures are applied to prevent hematoma and to mold the skin to the remaining contours. The conchal graft has a crescent shape, which can be modified as required. Its size is up to one quarter of the circumference of the ear and maintains two planes. Pearl The entire floor of the conchal bowl must be harvested, even in cases where it will not be entirely used. This will prevent residual irregularities. The root of the helix and the posterior lining of the auditory meatus should be preserved to prevent stenosis at the entrance of the canal. Deciding whether to reconstruct with conchal cartilage in one or two stages is often difficult. Conchal cartilage is soft and elastic and will not withstand significant compressive forces. If tension on the skin closure is excessive, then reconstructing in two stages is necessary. Fig. 12-2 This case demonstrates a defect after ear piercing that was reconstructed in a single stage. Skin was sufficient, but the chondritis had resorbed some of the cartilage in the upper part of the ear. An ipsilateral conchal cartilage graft was harvested and reshaped to reproduce the missing contours and was placed under the existing skin. Bolster sutures at both the recipient and donor site were left in place for 4 days to maintain adequate contours. This case demonstrates a partial traumatic defect in the upper part of the ear that had been closed to the surrounding skin. Reconstruction was performed using a contralateral conchal graft and an advancement flap from the sulcus, which in this area is not deep and only just allowed coverage of the graft. A second stage was necessary to elevate the reconstructed segment and to skin graft the posterior surface of the framework. An additional operative step is to decide whether to place the conchal graft anterior or posterior to the existing cartilage. Either can leave a noticeable line at the junction point unless fastidious care is taken to accurately oppose the edges. Placing the conchal graft posteriorly is often easier.
Reconstruction With Conchal
and Costal Cartilage
RECONSTRUCTION WITH CONCHAL CARTILAGE
Harvesting the Conchal Cartilage Graft
Demonstrative Cases
What Not To Do
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine