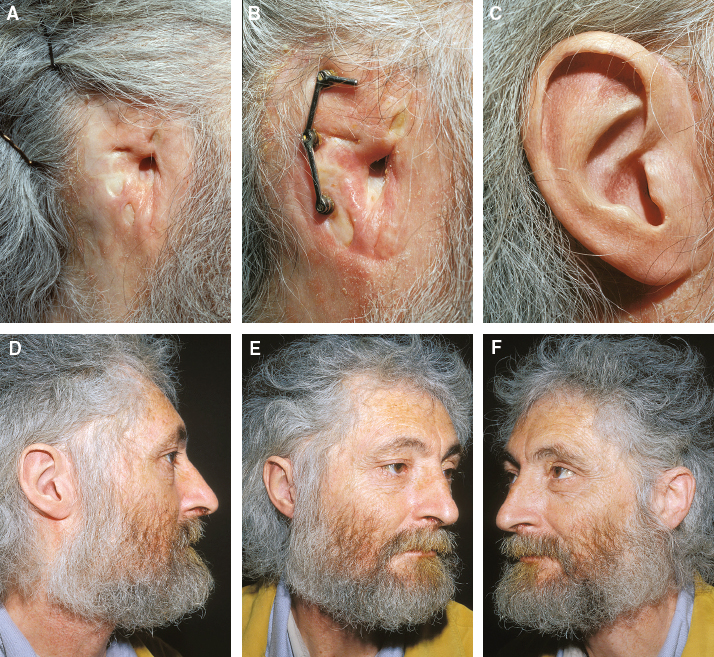
CHAPTER 10 Auricular prosthesis is the oldest technique for ear reconstruction. There are still some good indications to perform this procedure despite the progress in reconstruction with autologous rib cartilage. Surgeons who regularly perform ear reconstruction must recognize when to propose a prosthetic solution. They must be able to perform themselves placement of the intraosseous implants needed to anchor the prosthesis. The result relies on the correct positioning of these implants and the quality of the prosthesis performed by the anaplastologist. In cases of poor local tissue conditions, patients should be informed that an autologous ear reconstruction may fail, and that a prosthesis could become the appropriate solution. Patients should be given all the information regarding the risks of a prosthesis. There are different circumstances when the reconstruction with autologous cartilage will not be the best choice. Usually it is when local skin potential is not sufficient to cover a three-dimensional cartilaginous framework. Other indications include the following: • Posttraumatic cases with scars in the auricular area and a damaged superficial temporal artery • Secondary microtia with poor local tissue conditions and damaged superficial temporal and occipital arteries • Desire of the patient disappointed with the result and who does not want to consider a new reconstruction with autologous cartilage harvested from the contralateral side • Failure of a reconstruction performed in difficult local conditions • Elderly patients In some cases the cartilaginous framework cannot be covered except with a contralateral free temporofascial flap. However, many patients accept the solution of a prosthesis and a wig. Fig. 10-1 During the initial consultation, the local conditions should be precisely analyzed to determine whether fascia surrounding the ear can be used; the surgeon must consider the circumstances and previous surgery. The native tragus is frequently present even after total amputation of the ear and can very conveniently hide the anterior border of the prosthesis. This 20-year-old patient was seen 3 months after an automobile accident. A large temporal scalp flap was used to cover the exposed temporal bone. Doppler examination confirmed that the superficial temporal artery had been damaged. The auricular area had only a scar. Although the patient was young, we gave him the option of placing prosthetic implants in a single stage. We waited 3 months for healing, which also gave the patient time to consider this solution. The temporal scar was revised, and three implants were placed. The result was very satisfactory, as observed after 8 years’ follow-up and the third prosthesis. The anterior border of the prosthesis is best concealed when a native tragus is present. For secondary cases, a new autologous ear reconstruction may be an option (see Chapter 8), in which cartilage is harvested from the contralateral side. However, the prosthetic option should always be discussed with the patient. In some cases the only choices to consider are free flaps, which are not our preferred choice because of the high complication rate. Fig. 10-3 This patient with right microtia was referred to us after failure of the temporal fascia. She had conchal-type microtia with the auditory canal. Before placing the implants, skin expansion was performed under the scalp to excise the scarred skin and the alopecic skin around the auricular area. During placement of the implants, the scarred area was again reduced, and the tragus was repositioned. The prosthesis adapted well to the remaining tragus. This 18-year-old patient had a hemifacial microsomia. Three operations were already done, including the use of temporal fascia and rib cartilage harvested on both sides. The reconstructed ear was positioned too low. The shapeless ear was removed, and the skin flaps were thinned and stretched to leave an even surface. Three osteointegrated implants were placed in the area overlying the ideal position of the antihelix in a single-stage operation. The patient is seen 3 years after surgery. Fig. 10-5 This patient had four surgeries elsewhere for her right unilateral microtia. The temporal vessels were intact, and she had enough costal cartilage for a new framework. However, she was not motivated to undergo a new autologous reconstruction. The remnants were removed, and two osteointegrated implants were placed in the area overlying the ideal position of the antihelix. She was so pleased with her new ear that she asked for a rhinoplasty. Her results are shown 2 years later. Because of the absence of the tragus, the edge of the prosthesis is visible behind the cheek. She conceals it with her hair. Local conditions may compromise the possibility of ear reconstruction. Patients who are informed about the risk of failure and are still motivated should also be informed that a prosthesis is a possible solution in case of failure. This 30-year-old patient already had three operations to reconstruct his ear after an automobile accident. The superficial temporal and occipital arteries were damaged. A fascial flap with a large random pedicle was planned. A Y-shaped skin incision allowed exposure of the fascia in the temporal area where the fascia is thinner and suitable for covering the framework (A and B). The perioperative aspect of the flap covered with a split-thickness skin graft harvested from the scalp seems satisfactory (C). Part of the skin graft failed, but the framework was still covered with granulating tissue (D). Then a new skin graft was placed on it (E). The patient returned to his country with a residual area of granulating tissue (F). An incorrectly treated infection (Pseudomonas) was responsible for almost total resorption of the cartilaginous framework. As previously mentioned to the patient before deciding on reconstruction because of failure, the only solution was a prosthesis (G and H). The patient was very satisfied with the final result. Two years after placement, he returned to have some granulations at the base of the implants treated with electrocoagulation and corticosteroids (I and J). Many elderly patients who have had previous surgery can be offered a prosthetic solution. Although there is no correlation between age and ossification of the rib cartilaginous segment, this can be checked on a CT scan before surgery. These patients may be secondary cases or may already be wearing a prosthesis anchored with glue. In some, a skin tunnel was performed before bone anchoring became the usual technique.
Auricular Prosthesis
INDICATIONS
Posttraumatic Cases

Microtia Secondary Cases

Patients Not Motivated Even if a New Reconstruction Is Possible

Failure of a Reconstruction Performed in Difficult Local Tissue Conditions
Elderly Patients
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine