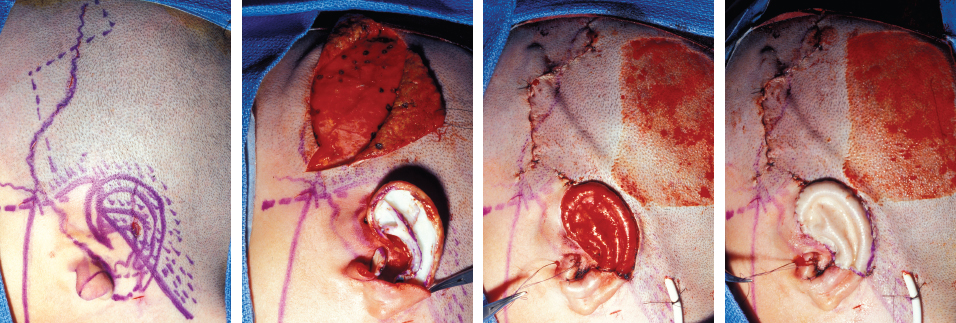
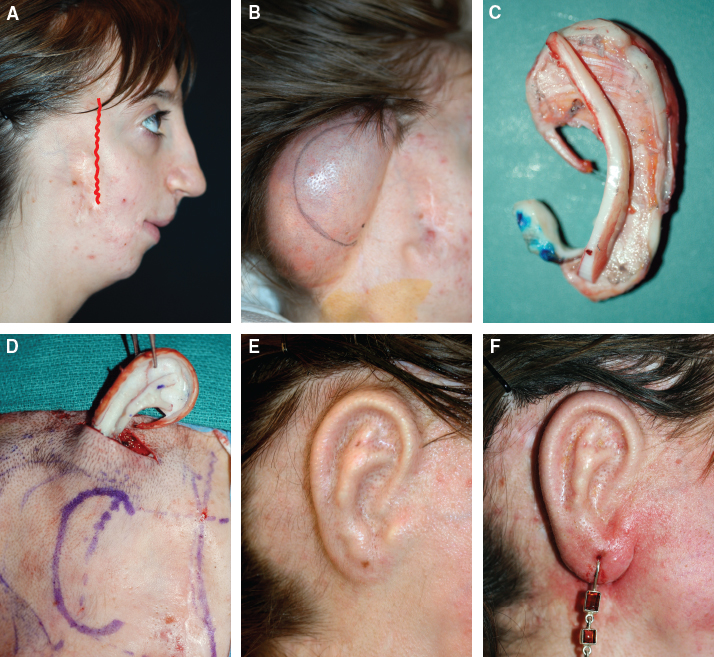
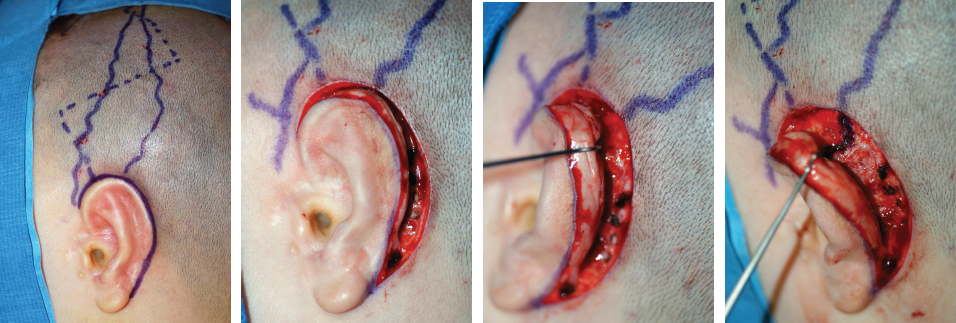
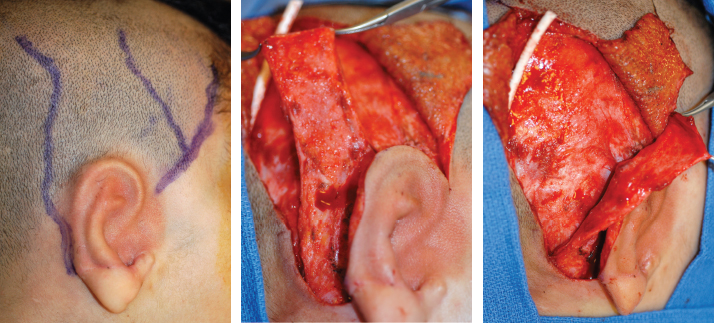
CHAPTER 5 The ear is situated posterior to the temporomandibular joint and projects over the mastoid process of the temporal bone on the cranium. Therefore the ear can almost always be positioned correctly despite facial asymmetry. However, surgeons must understand the need for flexibility if reference facial landmarks are used to correctly position the ear. They must remember that the two profile views of the patient are very rarely seen simultaneously and that the position of the two ears is only seen together from the frontal and posterior views. Thus some compromise regarding the position of the ear may be acceptable in the horizontal plane but never in the vertical plane. The distance between the lateral canthus and the auricular area is often shorter on the affected side in cases of facial asymmetry. This patient with hemifacial microsomia (HFM) and lobular-type microtia had a first-stage reconstruction placing the framework in a more anterior position than the normal ear to use the non-hair-bearing area to cover it. Soon after the second stage and before surgery on the mandible, the ears are in a symmetrical position from the frontal view, which is essential. Symmetry in the vertical plane is not only critical for a good aesthetic result from the frontal view but also for adequate support for glasses. Here, the ear has been placed in the correct position, and the appearance of slight asymmetry is the result of the chin asymmetry and hypotrophy of soft tissue that have not yet been corrected. Pearl 1. The patient should put on a pair of glasses to appreciate the correct level of the ear. The correct vertical position of the ear can also be appreciated from the posterior view, because it excludes the asymmetry of the face. 2. Some patients who routinely wear glasses before their ear reconstruction find a clever solution, particularly when presenting with bilateral microtia. This patient with a complex facial malformation uses custom-designed glasses. Fig. 5-4 This patient with a bilateral HFM uses custom-designed glasses. Fig. 5-5 This patient presented with severe hemivertebral fusion. He had facial asymmetry, and thus the ear was reconstructed, taking all landmarks into account. Although the position of the ear is correct, it seems lower than the other one because of the shortness of the neck on the affected side. The mandible will either be corrected early if severe or may be delayed until after the ear reconstruction. When it is corrected after ear reconstruction, an asymmetry of the inferior part of the ear will always be present. Because the ear is located not on the face but on the cranium, it is possible to correctly analyze and use the fixed landmarks of the normal side. However, surgeons should warn their patients that although the ear has been placed in the correct skeletal position, residual asymmetry will be present until facial asymmetry is also corrected. Fig. 5-6 This patient who presented with a subtle HFM had an ear reconstruction with good symmetry of the ear position, but her facial symmetry will be improved after fat grafting and genioplasty, which will be performed after skeletal maturity. Fig. 5-7 This patient, seen after 10 years of follow-up, presented with HFM. She had a right auricular reconstruction but did not want correction of the mandible. She had almost no remnants, and the reconstruction was performed with a satisfactory result. The ear has a correct position and good symmetry in the vertical plane. However, when the patient is observed from a worm’s-eye view or other angles, persistent facial asymmetry is evident, which is the main issue. The development of the mastoid is particularly important, because it will support the reconstructed ear. In cases of underdevelopment of the mastoid, in which the hollow is not very deep, a block of cartilage can be added beneath the inferior part of the framework from the antitragus to the intertragal notch (see Chapter 3.) This projection piece, known as PIII, adds projection to the lobule and antitragus and limits the descent of the framework into the mastoid hollow. When the depression is severe, the surgeon cannot expect the mandibular correction to affect the auricular depression, because the ear is located behind the temporomandibular joint and ramus of the mandible. This raises the question of how and when this depression can be corrected. In severe cases we perform fat grafting in two or three procedures to improve the quality of the hypoplastic skin before ear reconstruction. Perhaps in the future vascularized tissue transfer could be considered for reconstructing this hollow. Bone grafting or the use of alloplastic material has also been suggested. For each of these techniques, the optimal time needs to be determined: before the first stage, during the second stage, or after completion of the ear reconstruction. Fig. 5-8 This patient with HFM had an ear reconstruction and subsequent correction of the mandible (A-C). However, hypoplasia of the mastoid is evident. The result of the ear reconstruction alone is satisfactory, but the inferior part of the ear sits in a hollow behind the vertical ramus of the mandible (D). A late follow-up (10 years) shows that this sunken lobule has created an oblique axis of the ear (E and F). In such cases the hollow should be corrected, but the ideal timing and exact procedure to perform are not yet established. A low hairline is commonly seen in HFM. Even when no clear signs of facial asymmetry are obvious, we have found that the absence of a preauricular sideburn is pathognomonic for the syndrome. Usually, if sideburns are absent, some evidence of asymmetry is present, even if minor. We have also found a high incidence of low hairline in Treacher Collins–Franceschetti (TCF) syndrome. In this condition the sideburn will usually be anteriorly projecting onto the cheek, and the course of the superficial artery is very commonly ectopic. Preoperative Doppler ultrasonography is very useful in these cases. If, after determining the ideal position of the ear, part of the ear is placed under the postauricular hairline, the use of temporal fascia must be considered (see Chapter 4). We routinely use a “harmonic scalpel” to elevate the fascia, which facilitates the dissection. The hairy skin and temporal fascia may be removed only during the second stage in cases in which a small amount of hair may cover part of the upper part of the helix. There is a spectrum of severity of low hairlines. Fig. 5-9 The non-hair-bearing skin located in the auricular area is always preserved and will be used to partially cover the inferior part of the framework at a level that will vary according to skin laxity. In this case of lobular-type microtia, the remnant will allow the use of the lobule to cover the inferior part of the framework, and the superior two thirds will be covered by a temporal fascia and split-thickness skin graft harvested from the scalp. Fig. 5-11 The hairline is ultralow in this case, and complete coverage of the framework with temporal fascia must be planned. A large fascia was elevated, which allowed coverage not only of the external surface of the framework but also part of its posterior surface, reconstructing the sulcus. Thus the ear reconstruction was performed in one stage. This patient had severe HFM with facial asymmetry, ectopic remnants, and hypoplasia of the mastoid (A and B). A first operation was performed to excise the ectopic remnants and improve the quality of the auricular skin with fat grafting (C and D). Six months later, the first stage of the ear reconstruction was performed, covering the upper part of the ear with a temporofascial flap. The dressing was removed at day 3 and showed that the skin graft covering the temporal fascia had taken. This aspect and color are typical on day 3 (E). It usually takes 6 to 12 months for resolution of the edema and fibrosis and final definition of the contours. When performing a temporofascial flap during the first stage, we routinely wait 12 months before performing the second stage (F). Although the final result after the secondary stage was satisfactory, the asymmetry of the face must still be corrected to achieve symmetry (G-I). Lasers may be used in some situations to prepare the auricular area, particularly when a low hairline is present and the temporal fascia cannot be used. Nevertheless, because the scalp is not as thin as the retroauricular skin, a laser alone will not give the skin potential needed to follow the contours of the framework. That is why in the following case we used tissue expansion before performing the laser treatment. In addition, laser treatment is more effective when used on the hair-bearing skin with a tissue expander in situ. This is most likely the result of the relative ischemia and sparsity of the hair follicles undergoing laser treatment. Fig. 5-13 This patient had a complex malformation of the face and has undergone a cleft lip repair and removal of some very ectopic auricular remnants. The route of the superficial temporal artery is ectopic anteriorly, and the hairline is very low (A). A very atypical approach was used, in which an expander was placed under the hair-bearing scalp located at the posterior border of the ideal location of the ear. After laser treatment of the hair overlying the expander, some non-hair-bearing skin needed to be advanced into the sulcus during the second stage (B). TYPE I, PII, PII framework (C). During the first stage, a simple skin incision (type 3b) allowed insertion of the framework (D). The skin potential obtained allowed the insertion of the framework, including posterior projections (E). Six months later the sulcus was reconstructed (type D); advancement of the non-hair-bearing area was obtained from the laser treatment performed on the expanded skin. At the 1-year follow-up, no hair regrowth was observed, and the patient is ready for an ear piercing (F). In cases of microtia, the superficial temporal artery can be ectopic; part of the artery is located under the ideal location of the ear. Because it is localized and protected during the first stage, it is advantageous to elevate the framework without adherent soft tissue, preventing damage to this ectopic artery. Fig. 5-14 This case demonstrates the advantage of elevating the framework by closely following its posterior surface. The artery was found traveling within the superficial fascia and was preserved by following the posterior surface of the cartilage. The next step was to elevate the scalp skin flaps to prepare the temporofascial flap, which will have a short root to cover the cartilage block and the exposed cartilage behind the framework. Fig. 5-15 When the superficial temporal artery is ectopic anteriorly, the surgeon must incorporate it into the reconstruction. As seen in this case, a fascial flap is alternatively used with axial vascularization from the occipital artery. The surgeon must shave the scalp widely and mark the course of all arterial branches with Doppler mapping. Remnants are considered ectopic when they are located outside of the ideal position of the reconstructed ear. Drawing the ideal location of the ear first will help to determine whether the remnants can be used without compromising the ideal position of the ear. The remnants can frequently be used if they are ectopic but in the auricular area. We commonly encounter two different situations: ectopic remnants without an auditory canal and ectopic remnants with an ectopic auditory canal. If the ectopic remnants are too far from the ideal position of the ear and cannot be used, they should be excised.
Particular Cases of Microtia
PARTICULAR PROBLEMS
Asymmetrical Face
Asymmetry of the Zygomatic Area

Cervical Spinal Cord Malformations

Hypoplasia of the Mandible
Hypotrophy of the Mandible


Hypoplasia of the Mastoid

Low Hairline


Laser Hair Removal for Low Hairlines
Ectopic Artery
Ectopic Remnants
Ectopic Remnants Without an Auditory Canal
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine