div class=”ChapterContextInformation”>
11. Surgical Reconstruction of Penile Urethral Strictures: Staged Procedures
Keywords
Penile urethral strictureStaged proceduresUrethroplastyBuccal mucosa graftReconstructive urology11.1 Introduction
Staged urethroplasty involves utilizing more than one surgical intervention in the treatment of urethral stricture, diverticulum or fistula. While single stage procedures are favored for obvious reasons, there is a well-established role for staged procedures. Indications include: strictures related to lichen sclerosis (LS), prior reconstructive surgery for hypospadias or urethral stricture, poor tissue quality or a paucity of viable genital skin for flap reconstruction, and an absent lumen precluding substitution urethroplasty. Current staged procedures involve tissue transfer, most commonly using buccal mucosa in the modern era [1, 3]. This chapter will outline the relevant preoperative evaluation in patients with penile urethral stricture or fistula, and describe the surgical technique and reported outcomes of staged urethroplasty for penile urethral reconstruction.
11.2 Preoperative Evaluation
The preoperative evaluation in patients being considered for urethral reconstruction is critical for adequate preoperative counsel and surgical planning. Evaluation should include a detailed history with specific attention to pertinent pediatric urological history, prior surgical interventions, previous history of genitourinary trauma or infection, recent urethral instrumentation, current voiding pattern, and a history of urinary retention especially if associated with renal insufficiency. Additional important patient factors that should be documented include presence of urinary incontinence, erectile dysfunction or chordee, history of malignancy and relevant treatment modalities used (especially radiation), and oral pathology or tobacco use. The aforementioned list is by no means exhaustive, but rather a starting point to frame the subsequent discussion for treatment of urethral stricture. Physical examination is also key when deciding on surgical approach, especially for a penile urethral stricture. Assessment should include documentation of quality and availability of penile skin and soft tissue, circumcision status, location and severity of genital scars, and the presence of LS.
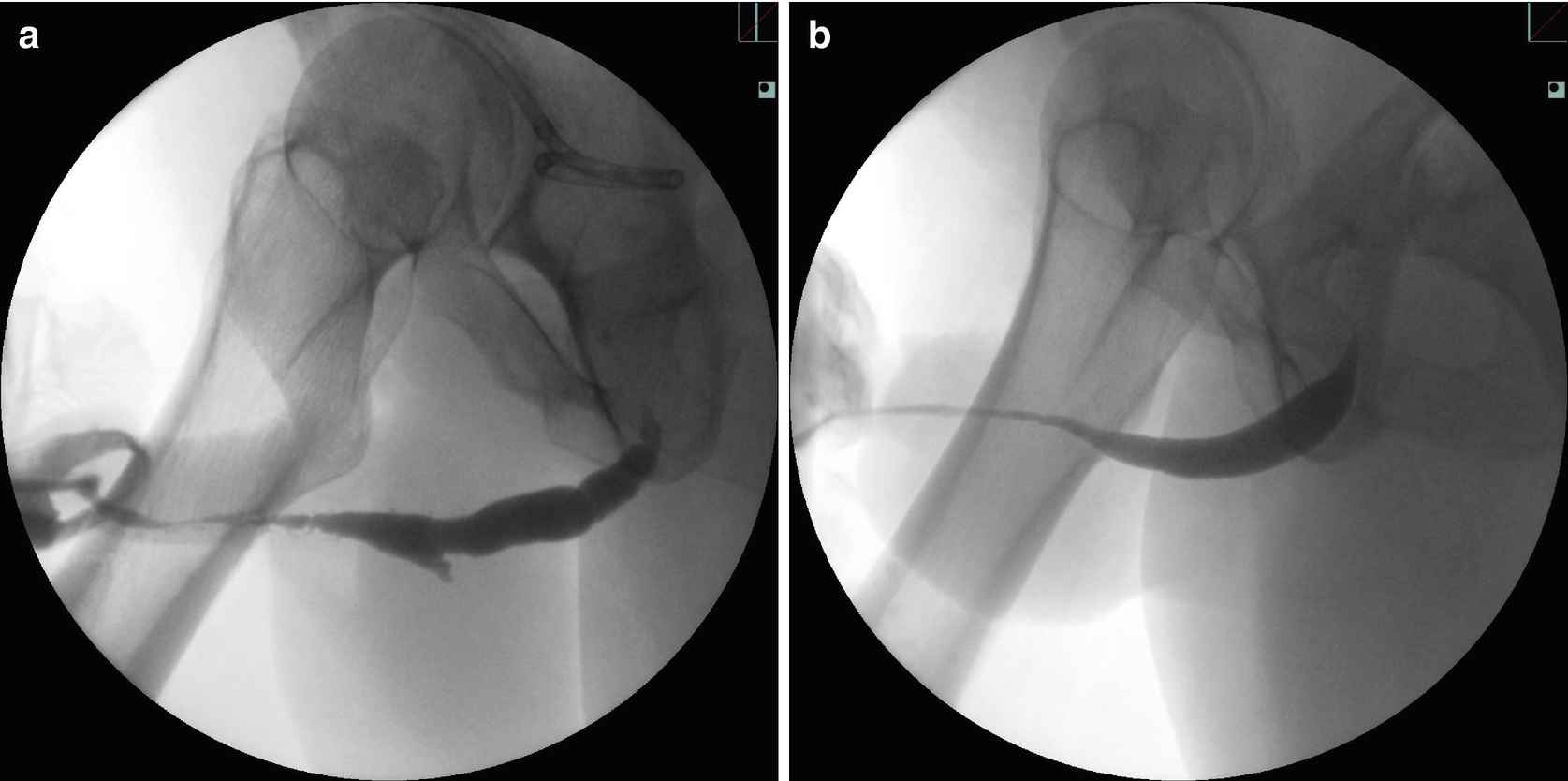
Penile urethral stricture related to: (a) multiple prior surgical procedures for penoscrotal hypospadias and subsequent complications, (b) lichen sclerosis (LS)
Managing expectations and helping the patient understand the timeline for urethral reconstruction is integral to the success of the operation. The period of urethral rest prior to the first stage procedure must be discussed, as well as a possible need for a suprapubic catheter to allow for this if the patient is requiring frequent dilation or performing self-catheterization. Between the first and second stage, a period of 4–6 months is typical for graft take and stabilization, and the patient needs to understand the process of sitting to void through a penile or upper scrotal urethrostomy during this time. Sexual intercourse is allowed approximately 6–8 weeks after the first procedure, and the patient is made aware that semen will also emanate from the urethrostomy. Following the second stage procedure, a catheter or urethral stent is left in the urethra for a period of 18–21 days to permit urinary diversion and urethral healing. Intercourse is again allowed after 6–8 weeks . From a surgical standpoint, patients must also understand the longer term risks of stricture recurrence, urethral fistula or diverticulum, spraying of the urinary stream, and potential need for additional procedures.
11.3 Surgical Technique: First Stage for Penile Stricture
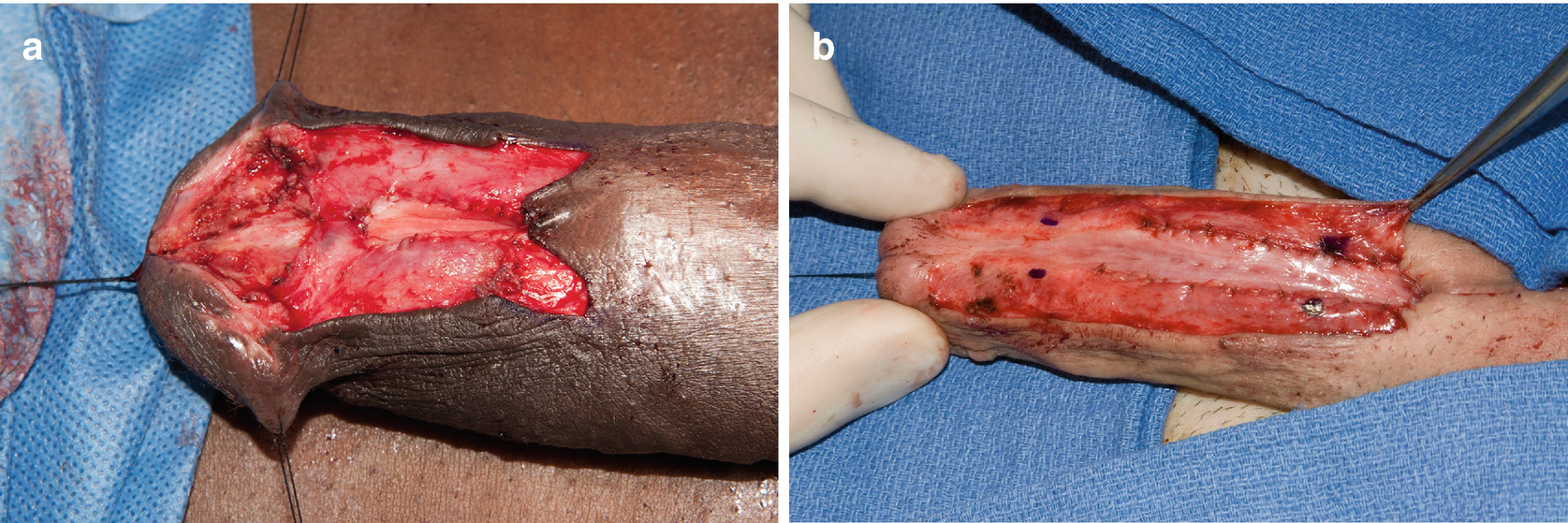
(a) Urethral excision and urethrostomy in patient following prior distal hypospadias repair; (b) Urethrotomy and penoscrotal urethrostomy in setting of LS
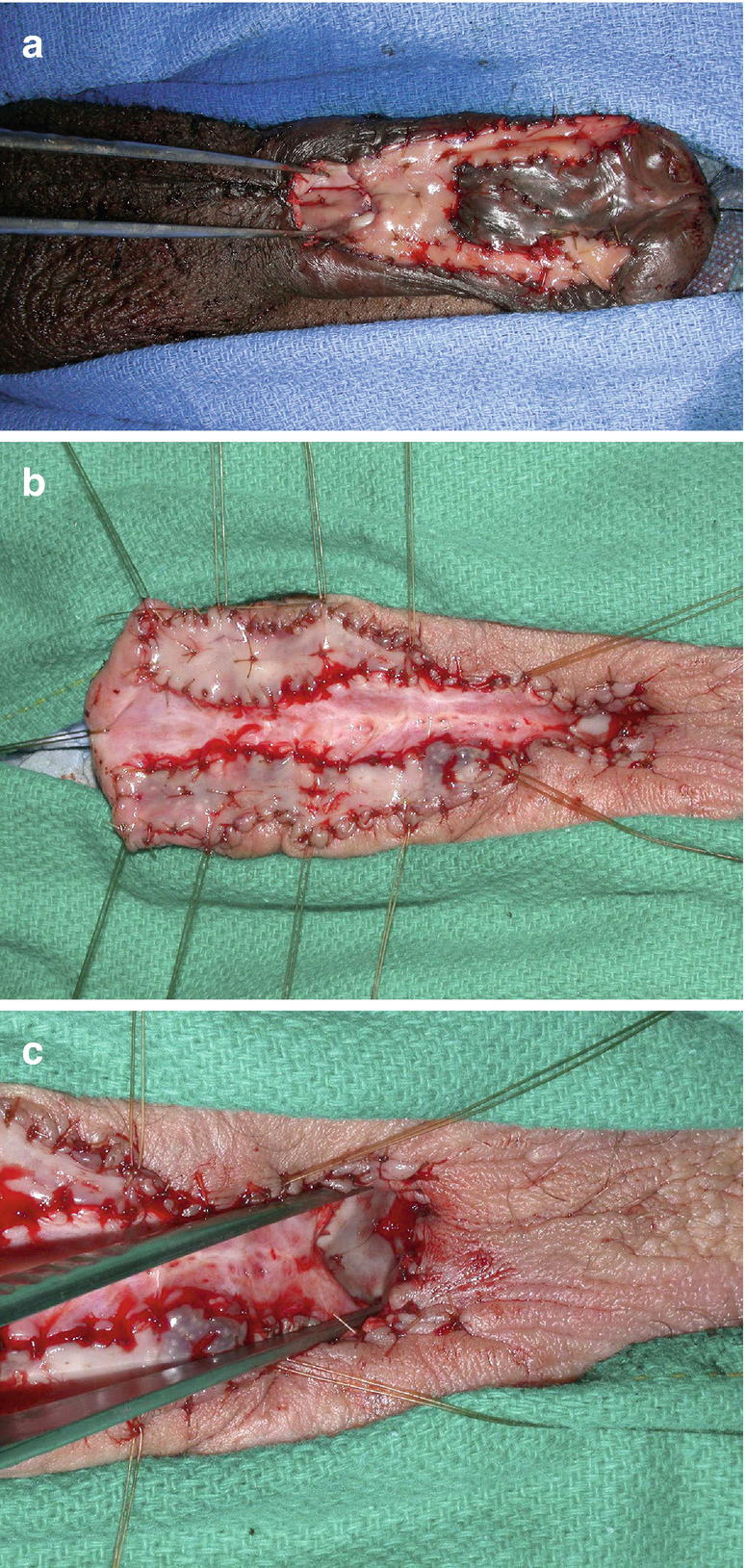
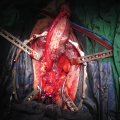
(a) Complex first stage hypospadias patient with proximal dorsal buccal mucosa graft seen between forceps at proximal urethrostomy; (b) Proximal dorsal graft at urethrostomy opening for extensive LS stricture; (c) Closer view of urethrostomy and graft

Related posts:
 Changing Scenario of Urethral Stricture Management
Changing Scenario of Urethral Stricture Management
 Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
 Reconstruction of the Lower Urinary Tract
Reconstruction of the Lower Urinary Tract
 Presentation and Diagnostic Evaluation of Male Urethral Stricture
Presentation and Diagnostic Evaluation of Male Urethral Stricture
 Reconstruction of Panurethral Stricture Disease
Reconstruction of Panurethral Stricture Disease
 Private: Reconstruction of Pelvic Fracture Urethral Injury
Private: Reconstruction of Pelvic Fracture Urethral Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


