The lips play an important role in both human physiology and culture. As the portal of entry for the gastrointestinal system, the mouth and lips take part in the cephalic phase of digestion. The sphincteric action of the orbicularis oris closes the oral stoma creating a seal. Oral competence prevents drooling while the tongue and cheeks manipulate intraoral solid and liquids. Contraction of perioral musculature positions the lips against the bony skeleton, thereby obliterating the gingivobuccal sulci for manipulation of the food bolus toward the teeth for chewing and oropharynx for swallowing. The same complex set of muscular actions enables newborns to suckle.
The lips participate in both verbal and nonverbal communication. Articulation, the physical production of speech sounds, is modified by lip movement. Lip position, shape, and motion are gestures used to express emotion. Indeed, a smile or a frown can be as effective in communication as the spoken word. Finally, kissing is a common means of social greeting as well as a form of intimate expression.
ANATOMY
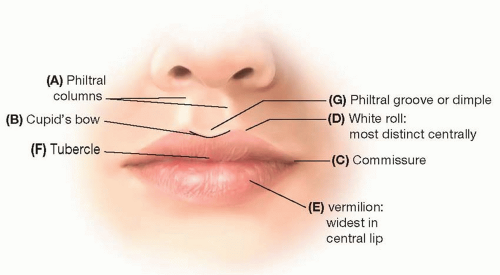
Topographically, the lips are distinct from surrounding structures. The upper lip extends cephalad to the nostril sills and alar base on each side and terminates laterally at the nasolabial creases (Figure 34.1). The upper lip is further divided into subunits by the philtral columns that extend from the nasal sills to the cutaneous-vermilion junction inferiorly. The philtral columns are created by contralateral orbicularis oris fibers that cross the midline to insert directly into the overlying dermis.1 The central depression between the philtral columns is termed the philtral groove or dimple. The Cupid’s bow is the area of the cutaneous-vermilion junction between the philtral columns, termed as such because its shape resembles the mythologic character’s weapon. The lower lip begins laterally at the continuation of the nasolabial creases and is bordered inferiorly by the labiomental crease. The upper and lower lips join at the commissure.
FIGURE 34.1. External lip anatomy. Philtral columns (A). Cupid’s bow (B). Commissure (C). White roll: most distinct centrally (D). Vermilion: widest in central lip (E). Tubercle (F). Philtral groove (G).
The lips’ cutaneous portions terminate at the vermilion-cutaneous junction termed the white roll or white skin roll. The color and elevation of the white roll is created by par marginalis fibers of the orbicularis oris.2 The white roll is most distinct in the lip center tapering gradually toward the commissures. The vermilion, which is composed of keratinized squamous epithelium, transitions distinctly at the red line into nonkeratinized squamous epithelium of oral mucosa. Similar to the white roll, the vermilion is widest in the central lip.
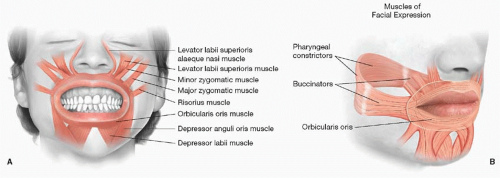
Muscles of the lip and perioral region are best understood by grouping them into functional categories. The maxillary region muscles that are responsible for the upper lip elevation include the zygomaticus major, zygomaticus minor, levator labii superioris alaeque nasi, levator labii superioris, and levator anguli oris (Figure 34.2A). The levator labii superioris, levator anguli oris, and zygomaticus minor contribute to the formation of the nasolabial crease. Retraction and depression of the lower lip are due to combined actions of muscles located around the central mandible, including the platysma, depressor anguli oris, and depressor labii. The mentalis muscles force the lower lip against the mandible, indirectly elevating it and creating a pout. Muscles of the intermaxillary region include the orbicularis oris, buccinator, and risorius. The orbicularis oris is composed of two components: the pars marginalis and pars peripheralis. The par marginalis lies anterior to the pars peripheralis and is mostly limited to the area directly deep to the vermilion. The pars peripheralis extends from deep to the pars marginalis to behind the cutaneous portion of the lip. The orbicularis is the most important lip muscle, providing oral competence through its sphincteric action in the coronal plane. The maxillary and mandibular perioral musculature adjust the sagittal and axial positions of the orbicularis oris. In the axial plane, the combined action of the orbicularis risorius, buccinator, and pharyngeal constrictors forms a muscular ring that presses the lips against the gingiva and teeth clearing intraoral sulci (Figure 34.2B). The modiolus refers to a complex interdigitation of the perioral muscles that retract the corners of the mouth.
The facial and perioral muscles are arranged into four layers based upon relative depth to one another. All of the muscles are innervated on their deep surface, with the exception of the deepest layer that includes the mentalis, levator anguli oris, and buccinator muscle.
Blood supply to the lips is based upon the network off the external carotid artery system. As the facial artery branches from the external carotid artery, it hooks around the mandible body immediately anterior to the masseter muscle. It courses deep to the risorius, zygomaticus major, and superficial lamina of the orbicularis oris muscle and lies superficial to the buccinator, the levator anguli oris, and deep lamina of the orbicularis oris muscle. The facial artery is located approximately 1.5 cm (range 9.2 to 19.8 mm) lateral to the oral commissure where it gives rise to the superior and inferior labial arteries.3 Since labial vessels reliably anastomose with their contralateral counterparts, a lip switch flap can be based at either side. The superior labial artery lies within 10 mm of the lip margin. This may or may not be within the actual red lip. The inferior labial artery is positioned 4 to 13 mm from the margin of the lower lip. The labial vessels lie either within or posterior to the orbicularis oris muscle, but never anterior to it. Within the lips, the facial vein is not a well-formed single anatomic structure, but more closely resembles a venous plexus. Lymphatic drainage proceeds via submental and submandibular nodal chains.
FIGURE 34.2. Lip musculature. Perioral muscles acting in the coronal plane (A). Perioral muscles acting in the axial plane (B).
Motor innervation to the lip musculature is provided by facial nerve (VII) branches. Zygomatic and buccal branches innervate lip elevators and retractors, whereas the marginal mandibular nerve innervates lip depressor muscles. Sensibility to the upper and lower lips is provided by the infraorbital (V2) and mental (V3) branches of the trigeminal nerve, respectively.
DEFECT ETIOLOGY
The major etiology of acquired lip deformities is cancer. Ninety-six percent of lip cancers occur on the lower lip presumably from prolonged sun exposure.4 Overall, squamous cell is the predominant tumor cell type (96%), followed thereafter by basal cell cancers, verrucous carcinomas, and adenocarcinomas. Ninety-seven percent of patients with lip cancer are male. Female patients are significantly more likely than men to have upper lip involvement (20% versus 4%). Uncommon indications for lip reconstruction include trauma, infectious diseases such as noma, vasculitis, vascular anomalies, and burn injury.
HISTORICAL REVIEW
Historical review of lip reconstruction informs current methods of repair. Similar to other areas of plastic surgery, ideas are continually “re-invented” or modified. Crediting a single surgeon with a reconstructive technique can be incorrect since modern reconstruction has evolved after multiple iterations. Table 34.1 is a timeline of lip reconstruction, including a partial list of each author’s contribution.
RECONSTRUCTION
General goals of reconstruction include maintaining a dynamic oral sphincter, a sufficiently sized stoma, and an acceptable cosmetic result. As defect size increases, an adequate reconstruction is progressively more difficult to achieve since additional muscle groups, sensory/motor nerves, and soft tissue are sacrificed. When feasible, the best functional and cosmetic outcomes can be achieved by adhering to the axiom of replacing “like with like.” If possible, a subunit approach to reconstruction leads to superior aesthetic results, so this should be followed particularly for the upper lip, where distinct anatomical structures are present.5 Finally, reconstruction of large defects can be associated with a negative impact on the quality of life with patients avoiding activities such as social interaction or public eating; therefore, potential sequelae should be discussed preoperatively. The plastic surgeon should keep all these aspects in mind when planning any lip reconstruction.
Vermilion
The vermilion should be carefully realigned on each side of any defect since small discrepancies are noticeable from a short distance. To avoid misalignment, regional anesthesia such as mental and infraorbital nerve blocks are preferable to the tissue distortion caused by direct local anesthetic infiltration. Alternatively, the white roll can be temporarily tattooed with methylene blue prior to anesthetic infiltration. During lip reapproximation, sutures should be placed either above or below the white roll, but not directly on it to avoid blurring this distinct anatomical landmark.
The smallest vermilion defects can be repaired either primarily or be allowed to heal by secondary intention. If possible, primary repairs should avoid crossing the white roll. When required, local flaps are harvested from the same lip if possible. The simplest method of repair is undermining of the immediately adjacent intraoral mucosa with defect closure by advancement. This technique is commonly indicated for total lip shaves when a “field defect” is present on the entire lower lip vermilion. The drawback of this approach is that the lip is pulled inward with flattening of its normal pouty appearance. To improve the bulk of vermilion reconstructions, a portion of orbicularis oris muscle can be included with the advancement flap. Wilson and Walker proposed the creation of a laterally based bipedicle mucosal flap harvested from the depth of the gingivobuccal sulcus (Figure 34.3A).6 Skin grafting or secondary intention healing of the donor site facilitates tension-free closure at the vermilion suture line with absent lip retraction. Full-thickness defects of the vermilion that include a majority of the underlying orbicularis but do not extend beyond the white roll can be reconstructed with lateral vermilion musculomucosal advancement flaps supplied by labial vessels on either side of the remaining lip (Figure 34.3B). An incision made exactly at the white roll takes advantage of inherent lip elasticity while keeping the scar hidden along this line. Alternatively, musculomucosal flaps composed of intraoral mucosa and orbicularis can be advanced from the sulcus in a V-Y fashion.
TABLE 34.1 TIME LINE OF CONTRIBUTIONS TO MODERN LIP RECONSTRUCTION
▪
YEAR
▪
SURGEON(S)
▪
CONTRIBUTION
Vermilion
1892
Johannes von Esmarch
Mucosal advancement flap for total lip shave defect
1901
Multiple: Eiselsberg, Lexer, Bakamjian
Tongue flap for either mucosal or vermilion reconstruction
1981
John Wilson
Laterally based bipedicle mucosal advancement flap from the labial sulcus
1984
Morton Goldstein
Vermilion musculocutaneous advancement flap
1987
Colin Rayner
Random cheek musculomucosal flaps based at the angle of the mouth
1992
Julian Pribaz
Musculomucosal flap containing the facial artery
Adjacent cheek tissues
1834
Johann Dieffenbach
Reconstruction of the entire lower lip using full-thickness bilateral cheek transposition flaps
1857
Victor von Bruns
Reconstruction of the lower lip using full-thickness nasolabial flaps based either superiorly or inferiorly
1853
Camille Bernard
Reconstruction of the lower lip using full-thickness cheek advancement flaps with excision of redundant triangles of excess tissue at the flap base
1855
Carl Burow
Formalized excision of triangles from the bases of bilateral cheek advancement flaps
1946
Jerome Webster
Formalized perialar crescentic excisions for partial- and full-thickness upper lip defects, crediting Dieffenbach with the earliest example of this technique
1957
Harold Gilles
Full-thickness quadrilateral rotation advancement flap resembling a “fan” for either upper or lower lip reconstruction
1958
Bromley Freeman
Modification of the Bernard cheiloplasty with partial thickness, rather than full thickness, excision of the Burow’s triangles
1960
Richard Webster
Modification of the Bernard cheiloplasty with inclusion of 1 cm of buccal mucosa for vermilion reconstruction
1974
Miodrag Karapandzic
Musculocutaneous rotation advancement flap of the remaining lip that preserves the neurovascular supply
1983
Ian McGregor
Full-thickness quadrilateral flap similar to a “fan,” but rotates cheek skin into the lip defect rather than the remaining red lip; requires vermilion reconstruction
Opposite lip
1756
Johann Hjertzeel
Lip switch from lower to upper lip for noma
1838
Pietro Sabattini
Lip switch from lower to upper lip for post-traumatic defect
1848
Sophus Stein
Bilateral upper lip switch flaps to central lower lip oncologic defect
1864
Gordon Buck
Lip switch from lower to upper lip, including commissure for post-traumatic defect; secondary commissuroplasty
1872
Jakob Estlander
Lip switch from upper to lower lip, including commissure for oncologic defect
1898
Robert Abbe
Lip switch from lower to central upper lip for cleft deformity
1981
Jerry Templer
Hybrid lip switch referred to as Abbe-Estlander since an upper lip rectangular flap is based away from the commissure and rotated for a lower lip defect
Distant tissues
1974
Kiyonori Harii
Free scalp flap reconstruction of commissure defect
2005
Bernard Devauchelle
Midface transplant, including entire upper and lower lips
Only gold members can continue reading. Log In or Register to continue