Frequent in:
Aase S.
Baller-Gerold S.
Congenital microgastria-limb reduction complex
Deletion 13q S.
Fanconi pancytopenia S.
Holt-Oram S.
Levy-Hollister S.
Nager S.
Oculo-auriculo-verterbral spectrum
Radial aplasia-thrombocytopenia S.
Roberts-SC phocomelia
Rothmund-Thomson S.
Townes-Brocks S.
VATERR Association
Yunis-Varon S.
Occasional in:
De Lange S.
Foetal aminopterin/methotrexate S.
Foetal valproate S.
Fibrodysplasia ossificans progressiva S.
Fraser S.
Fryns S.
Hypomelanosis of Ito
Lenz microphthalmia S.
Miller S.
Monozygotic (MZ) twinning and structural defects—general
MURCS Association
Popliteal pterygium S.
Trisomy 18S.
Classification
Müller, in 1937, introduced the concept of a teratogenic sequence resulting in increasing severity of thumb hypoplasia [6]. He didn’t specify the precise anomalies associated with a particular grade of severity, although many subsequent reviews have attributed four grades of hypoplasia to his name. In 1967, Blauth refined Müller’s concept, defining five grades of thumb hypoplasia (Fig. 8.1) [7, 8]. A number of modifications to this classification have been suggested. That of Manske is most commonly quoted in the literature, but does involve significant changes to the definitions of Blauth [9, 10]. Blauth viewed the hypoplastic thumb according to grades of severity, with increasing bone and joint hypoplasia accompanied by increasing soft tissue hypoplasia. He distinguished Grade 2 from Grade 3 according to the presence or absence of a CMC joint, retaining the thumb in the former case but advising reconstruction of an alternative CMC joint in the latter. Manske moved this distinction into a sub-classification of Grade 3, in which Grade 3A has a CMC joint and Grade 3B does not. Buck-Gramcko added a 3C in which only the distal one-third of the metacarpal remained (Fig. 8.2) [11]. The Manske classification distinguishes between Grades 2 and 3A by the absence or presence of extrinsic musculotendinous anomalies. Such a sub-classification suggests that extrinsic anomalies develop with more severe grades of hypoplasia but are not present in less severe grades (Grades 1 and 2), and that these occur after the insult to intrinsic musculotendinous units. In my experience, if surgical reconstructions of thumb intrinsics, MCP joint instability and first web hypoplasia are indicated, there are always some extrinsic anomalies. These may or may not deserve reconstruction. It is of interest that neither the classification of Blauth nor Manske considered the stability or mobility of the CMC joint in those grades in which the proximal metacarpal is present (Blauth Grade 2, Manske Grades 2 and 3A). Manske specifically equated the presence of the proximal metacarpal with a stable CMC joint and proximal metacarpal absence with an unstable joint. Buck-Gramcko defined the 3A thumb as having an unstable CMC joint and described significant extrinsic anomalies within Grade 2.
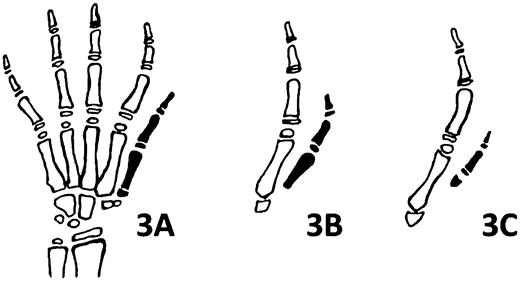
Fig. 8.1
Blauth grades of thumb hypoplasia 1–5. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.2
Classification of thumb hypoplasia as modified by Manske (Grades 3A and 3B) and Buck-Gramcko (Grade 3C). Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
I favour Müller’s concept of increasing hypoplasia of all thumb elements, of soft tissues, bones and joints, occurring concurrently, and Blauth’s distinction between Grades 2 and 3 according to the presence or absence of the proximal metacarpal. In its original form, the Blauth classification also provides logical guidelines for treatment by grade. In the main, Grade 2 thumbs are reconstructed; Grade 3 thumbs are removed and the index finger is pollicised. Manske and Buck-Gramcko moved these alternative treatment recommendations to within Grade 3, distinguishing between 3A and 3B.
Some who are classification “splitters” may choose to sub-classify Grade 2 according to which components of the thumb would be improved by surgical reconstruction and the techniques whereby this is achieved. Smith advised a Grade 2A or 2B on the basis of uniaxial or global MCP joint instability [12, 13]. This could be extended to specify differences in other aspects of Grade 2 hypoplasias. The classification “lumpers” may prefer to designate the classification of Grade 2 to all such thumbs, regardless of the reconstructive techniques utilised. However, as Buck-Gramcko states “the assessment of results is difficult, especially because the outcome depends on the preoperative condition in the severity of the deformity” [11]. It is clear that the surgical reconstruction of a thumb with uniaxial MCP joint instability, intrinsic hypoplasia and a mildly hypoplastic first web, when accompanied by minor extrinsic anomalies not requiring reconstruction, is quite different from the reconstruction of a thumb with global MCP joint instability, severe hypoplasia of the first web and intrinsic absence, in association with a pollex abductus anomaly and/or hypoplasia or aplasia of the extrinsic flexors and extensors and/or abnormal alignment and insertion of these.
The following classification is offered as one maintaining the integrity of Blauth’s skeletal classification and the teratological sequence of increasing severity of hypoplasia proposed by Müller, Blauth and others (Fig. 8.3). The subdivisions within grades do not create separate categories for each anatomical anomaly and its treatment, but allow the results of surgical reconstructions to be compared for “similar” thumbs:
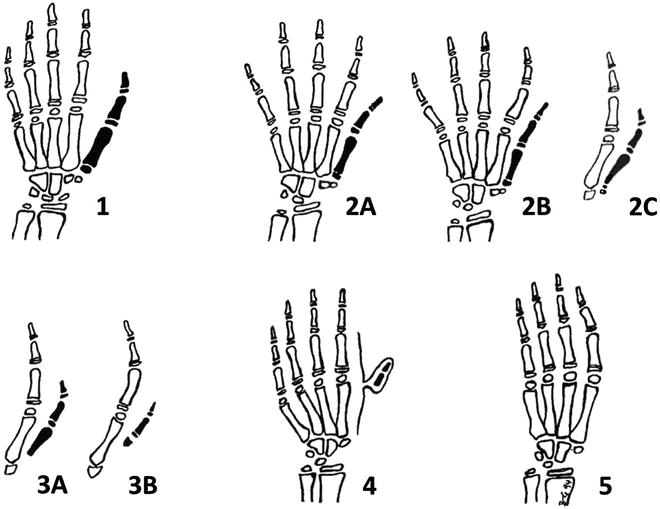
Fig. 8.3
Proposed modified Blauth classification. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Grade 1: The thumb is small, there is some hypoplasia of the thenar musculature and there may be mild extrinsic anomalies. However, the joints are stable and mobile. No surgery is indicated.
Grade 2: Thumb hypoplasia is more severe and would benefit from reconstruction. The CMC joint is present. Intrinsic and extrinsic anomalies are more significant and there is MCP joint instability and first web underdevelopment. An increasing severity of hypoplasia is recognised according to the clinical and radiological examinations:
2A: Mild. Hypoplasia of intrinsic muscles; uniaxial MCP joint instability; and adduction of the first metacarpal with first web deficiency. Management includes release of the first web, MCP joint ulnar collateral ligament (UCL) reconstruction and an opposition transfer as appropriate. Mild extrinsic anomalies do not demand attention.
2B: Moderate. The intrinsic hypoplasia and first web insufficiency are more severe. MCP joint instability is multiplanar, requiring reconstruction of soft tissues other than the UCL alone. Chondrodesis or formal fusion may be necessary in a minority. Extrinsic anomalies demand reconstruction for optimal thumb function and prevention of recurrence of deformity. CMC joint stability and mobility are adequate as indicated by radiological evidence of a proximal flare at the first metacarpal base (Fig. 8.4).

Fig. 8.4
Blauth Grade 2 (A, B) thumb hypoplasia with proximal metacarpal flare. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
2C: Severe. Increasing hypoplasia of all structures, with severe global MCP joint instability (“elephant’s trunk sign”), gross extrinsic hypoplasia, and an inadequate CMC joint—clinically unstable or immobile. These thumbs may also be identified by the radiological appearance of loss of the proximal metacarpal base flare, which tapers proximally (the “pencil sign”) (Fig. 8.5). The thumb requires a more significant first web release and skin transposition, an opposition transfer and extrinsic reconstruction. A chondrodesis or fusion of the MCP joint, and reconstruction of the CMC joint through stabilisation or mobilisation creates a satisfactory albeit compromised thumb ray. Rarely, pollicisation may be considered to provide a superior result for the most severe of these Grade 2C hypoplasias.

Fig. 8.5
Blauth Grade 2C thumb hypoplasia with an inadequate CMC joint. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Grade 3: Increasing hypoplasia of all structures. The CMC joint is absent (Fig. 8.6).

Fig. 8.6
Grade 3A—absent proximal metacarpal. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
3A: Absence of the proximal metacarpal.
3B: Distal metacarpal remnant is the only remaining metacarpal component.
Grade 4: Metacarpal absence. The floating thumb with phalanges is connected by a skin bridge to the index finger ray.
Grade 5: Thumb absence.
Pollicisation remains the optimal surgical reconstruction for Grades 3, 4 and 5. However, such a decision for children with Grade 3 and 4 thumbs may be complicated by concerns about the creation of a four-digit hand. More recently, alternative methods of construction of a CMC joint, through transfer of vascularised and non-vascularised joints and/or bone, have shown some encouraging results and may be indicated when the need to retain five digits is paramount [14–17]. The precise reconstructive procedure may be tailored to the degree of hypoplasia and the amount of bone available within the thumb to be retained. The surgical techniques are easier to perform and the results of such surgery are likely to be better for Grade 3A thumbs than for those of Grade 3B or 4. In Grade 5 hypoplasia, a vascularised toe transfer is perhaps the only feasible method of creating five digits.
Surgery
When the child is under anaesthesia, a further preoperative examination assists decision making. CMC joint stability and mobility, or the lack thereof, MCP joint instability and the passive range of IP joint motion can be confirmed at this time (Fig. 8.7a–c). Final decisions await the detail of anomalous anatomy revealed at surgical exploration.
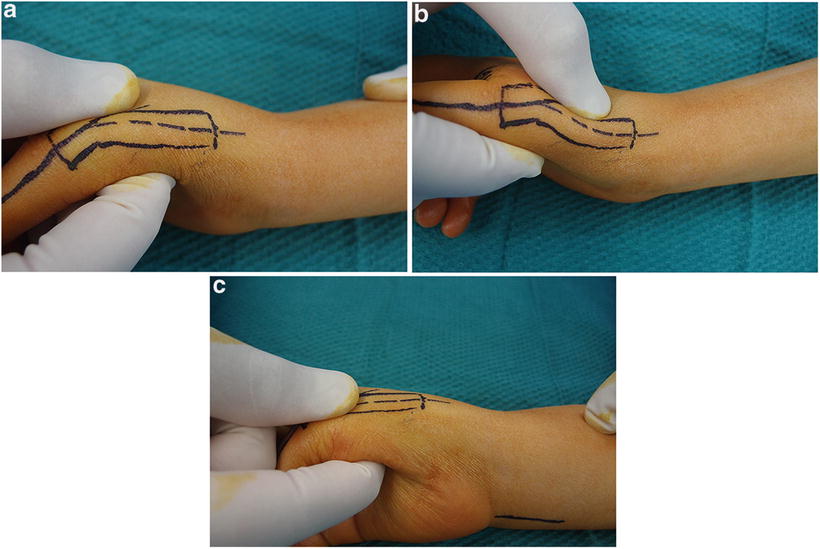
Fig. 8.7
(a–c) Assessment of CMC joint stability/motion at surgery. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Surgical Techniques
First Web Insufficiency
A four- or five-flap web-plasty are the most common techniques of first web deepening (Fig. 8.8a–d). Rotation and advancement of tissue from the dorsum of the hand may be indicated for more severe first web deficiency. It is very uncommon to require tissue from distant sources, such as a pedicled posterior interosseous artery flap or radial forearm flap, or even a free tissue transfer. They may be considered if reconstruction in Grades 3, 4 and 5 is undertaken.
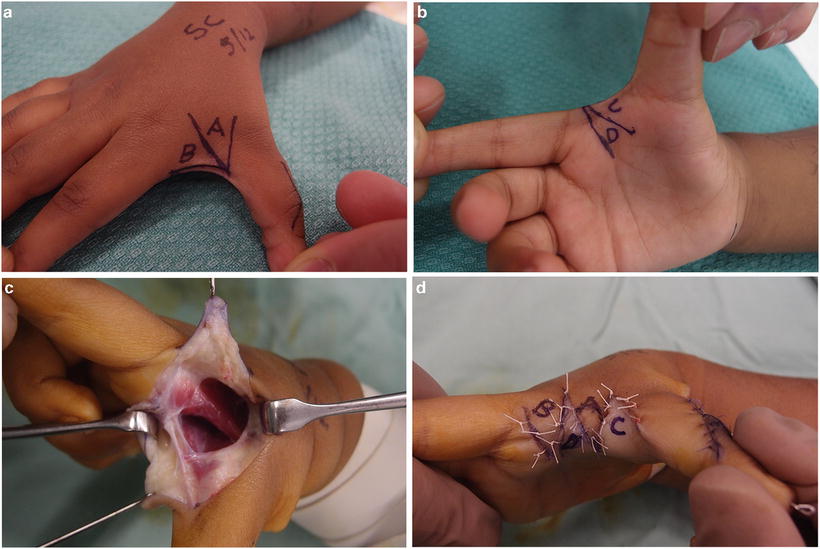
Fig. 8.8
(a–d) Four flap first web-plasty. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
The adductor pollicis and first dorsal interosseous muscles, both supplied by the ulnar nerve, are intact but play a role in the adduction of the first metacarpal and first web insufficiency. The thumb is weak and too aggressive a release of these muscles may position the thumb better but weaken it further. The fascia over each muscle should be divided (see Fig. 8.8c). Some gentle recession of the first dorsal interosseous from the thumb metacarpal or of the transverse component of the adductor pollicis may be indicated, but tenotomies should be avoided.
Metacarpophalangeal Joint Instability
In determining the optimal stabilisation procedure, consideration must be given as to whether the instability is predominantly a loss of UCL integrity (Grade 2A) or whether the instability is global (Grade 2B), requiring a more sophisticated reconstruction or even a chondrodesis or fusion of the joint (Fig. 8.9).

Fig. 8.9
Assessment of metacarpophalangeal (MCP) joint instability at surgery. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
There are two common methods of reconstruction of the UCL. One is to use available local tissue, imbricating capsule and ligamentous structures, such as they are, on the ulnar side of the joint. The other is to introduce tissue which is extrinsic to the joint to cater for the deficiencies of the local structures. The terminal part of a flexor digitorum superficialis (FDS) tendon used for an opposition transfer is a popular source.
Whichever reconstruction of the UCL is performed, it will fail if there is an abnormal abduction force crossing the MCP joint on its radial side, most commonly in association with a pollex abductus anomaly in which there is a flexor to extensor connection [18]. Attention must be directed to this if the joint forces are to be balanced and the UCL reconstruction protected.
My preference is to assess the calibre of the MCP joint ulnar soft tissues at the time of surgery. If they are satisfactory, I proceed to a double-breasting of these structures and protect the joint with a fine Kirschner-wire (K-wire). A strip of palmar plate can supplement this reconstruction. A 2- to 3-mm width may be mobilised, maintaining its insertion at the proximal phalanx base, transferring its proximal origin dorsally to the metacarpal head-neck junction. A similar technique may be applied for radial collateral ligament instability. If local tissue is adequate for collateral ligament reconstruction, the abductor digiti minimi (ADM) is used as an opposition transfer as described below. If the soft tissues are inadequate, then I will proceed to an FDS opposition transfer. One slip of the terminal part of the FDS is passed through a drill hole at the head-neck junction of the metacarpal, from radial to ulnar side, and is sutured to the base of the proximal phalanx and to soft tissues attached to this. Lister and subsequently Smith have advocated placing drill holes through the proximal phalanx, but I have tended to avoid this in the child because of the proximity of the growth plate and the small size of the bone.
One alternative for moderate global instability (Grade 2B) is to use two slips of FDS to reconstruct ulnar and radial collateral ligaments (Fig. 8.10). For MCP joint hyperextension instability, the whole of the palmar plate may be advanced proximally and fixed at the head-neck junction of the metacarpal, creating a check rein (Fig. 8.11a, b). I prefer this complex combination of soft tissue reconstructions to chondrodesis or fusion, unless the underdevelopment of articular surfaces is profound indeed. There is severe global instability. The “elephant’s trunk sign” is indicative (Fig. 8.12a, b). The condyles of the head of the metacarpal are severely underdeveloped on the palmar aspects, with the shape of the metacarpal head, viewed end-on, triangular in appearance, curving palmarwards in the manner of an elephant’s trunk. The base of the proximal phalanx is of small diameter and is planar with no concavity. A formal arthrodesis can be performed but this does shorten the thumb and is only possible if there is epiphyseal ossification. A chondrodesis, fixing the cartilaginous surfaces with one or two fine wires, will stabilise the joint, at least temporarily. This is necessary for the degree of underdevelopment present in Grade 2C thumbs.

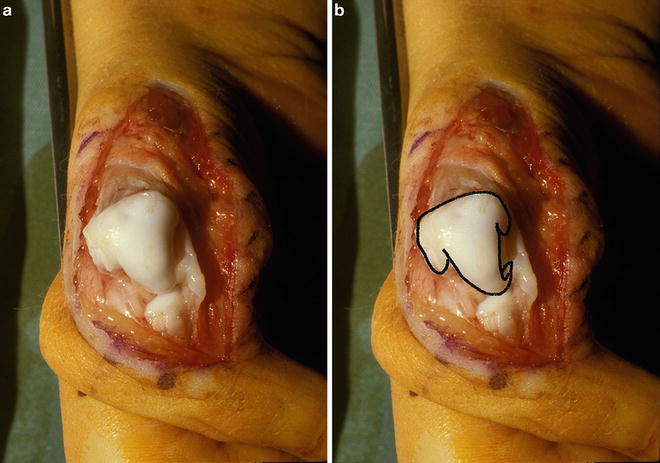
Fig. 8.10
Use of an FDS slip to create an MCP joint ulnar collateral ligament. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.11
(a, b) Advancement of the palmar plate proximally to prevent hyperextension instability of the MCP joint. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.12
(a, b) The “elephant’s trunk” sign of global MCP joint instability. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Correction of MCP joint instability is vital to the protection of the underdeveloped CMC joint. Radial deviation at the MCP joint results in adduction of the metacarpal and basal subluxation at the CMC joint, a zig-zag deformity. If an MCP joint fusion or chondrodesis is necessary, this lengthens the lever arm, which places increased stress across the CMC joint. An unstable CMC joint may be further compromised. In this instance, one must consider the necessity of a soft tissue stabilisation at the CMC joint level, a relatively difficult reconstruction using free tendon graft in a figure-of-eight fashion. A soft tissue release for an immobile CMC joint is possible but care must be taken for fear of instability. Rarely, in circumstances of severe MCP joint instability and significant proximal hypoplasia, in spite of the presence of a CMC joint, alternative methods of CMC joint reconstruction such as pollicisation may be considered.
Opposition Transfers
The main alternatives are an ADM (Huber) transfer and an FDS transfer. There are proponents of both but there is no clear indication of the superiority of one over the other. The use of the ADM diminishes the power of abduction of the little finger but provides some thenar bulk. It is a better pronator of the thumb ray. The FDS transfer removes a flexor from the usually more mobile ulnar digits (ring finger), perhaps decreasing grip strength, and fails to provide any bulk to the thenar eminence. The FDS is superior in providing palmar abduction but pronates less effectively. When additional tissue is needed to stabilise the MCP joint, the FDS can provide this as described above.
Abductor Digiti Minimi Transfer
The incisions are shown in Fig. 8.13. The ulnar incision at the junction of glabrous and dorsal skin provides a very pleasing cosmetic result (Fig. 8.14). Proximally, the incision should curve around the wrist crease at the level of the pisiform so that the origin of the ADM may be mobilised, if necessary, for length. Distally, the insertion of the abductor should be incised from the base of the proximal phalanx but the tendon contribution to the extensor mechanism dorsally should also be harvested to provide adequate length (Fig. 8.15). This tissue is not of adequate quality to be extended to the ulnar side of the joint for ligament construction. I do not transfer the origin of the ADM to the flexor retinaculum as suggested by some for fear of interference with the neurovascular pedicle. Its origin may be mobilised fairly aggressively, maintaining some attachment to both the flexor carpi ulnaris (FCU) and the pisiform proximally. Tunnelling of the muscle is a little more difficult with the ulnar incision than with a para-hypothenar incision. It is necessary to make certain that no retinacular fibres of the aponeurosis impede its passage and that the neurovascular bundle is not kinked during its transfer. Insertion at the thumb is into the abductor pollicis brevis (APB) remnant if it is present. Otherwise it is better to attach the transfer to the head-neck junction of the metacarpal rather than to the proximal phalanx, as the latter insertion tends to create a radial deviating force which may challenge the UCL reconstruction.



Fig. 8.13
Medial incision for abductor digiti minimi (ADM) transfer. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.14
Scar from medial incision following ADM transfer; note opposition and thenar bulk. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.15
Dissection for ADM transfer with distal extension to gain tendon length. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Flexor Digitorum Superficialis Transfer
Incisions are shown in Fig. 8.16. The FDS transfer is sutured to the periosteum at the head-neck junction with one slip passed through the metacarpal to be used for UCL reconstruction (see Fig. 8.10). The FDS transfer demands reconstruction of a pulley to allow an optimal direction of pull so that pronation of the thumb ray is possible. This is achieved with a distally based slip of FCU (Fig. 8.17). It is possible to also prolong a radial slip to assist in reconstruction of the radial collateral ligament for global instability, sometimes in association with a proximal advancement of the palmar plate, as described previously. This aggressive soft tissue reconstruction at the MCP joint reduces the necessity to consider a primary MCP joint chondrodesis or a fusion, or at least allows delay of such a procedure until a later stage if failure of the soft tissue reconstruction demands a more permanent solution.

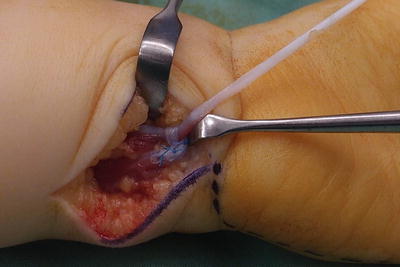
Fig. 8.16
Incisions for FDS transfer. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Fig. 8.17
 Anesthesia Concerns in Congenital Anomalies of the Upper Extremity
General Skeletal Disorders
Anesthesia Concerns in Congenital Anomalies of the Upper Extremity
General Skeletal Disorders
 Therapy Management of Children with Congenital Anomalies of the Upper Extremity
Therapy Management of Children with Congenital Anomalies of the Upper Extremity
 Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
 Ulnar Polydactyly and Ulnar Dimelia
Ulnar Polydactyly and Ulnar Dimelia
 Macrodactyly
Macrodactyly




FDS opposition transfer through an FCU pulley. Published with kind permission of Michael A. Tonkin ©2014. All rights reserved
Related posts:
Anesthesia Concerns in Congenital Anomalies of the Upper Extremity
General Skeletal Disorders
Therapy Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Ulnar Polydactyly and Ulnar Dimelia
Macrodactyly
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
