, Shimin Chang2, Jian Lin3 and Dajiang Song1
(1)
Department of Orthopedic Surgery, Changzheng Hospital Second Military Medical University, Shanghai, China
(2)
Department of Orthopedic Surgery, Yangpu Hospital Tongji University School of Medicine, Shanghai, China
(3)
Department of Microsurgery, Xinhu Hospital Shanghai Jiao Tong University, Shanghai, China
The reverse-flow radial forearm (Chinese) island flap is based on a distal vascular pedicle consisting of the radial artery and its venae comitantes. The advantages of using this pedicled flap for hand reconstruction are numerous. However, two major disadvantages of the donor site restrict the flap’s clinical applications. First, the sacrifice of a major artery may possibly jeopardize hand viability. Second, a displeasing scar deformity may occur if split-skin grafts are used for closure. Surgeons have made efforts to overcome these drawbacks. The distally based radial forearm perforator flap—a new flap based on the tiny perforators around the radial styloid process and the longitudinal chain-linked vascular plexuses—was invented.
The radial artery perforator (RAP) flap with preservation of the radial artery was firstly reported by Zhang [1] for hand reconstruction. Chang [2] performed an anatomic study in 1990 to show that the pivot point of the pedicle was located 1.5 cm proximal to the radial styloid process.
10.1 Vascular Anatomy
Along its course down the forearm, the radial artery gives off approximately 12 perforators to the skin along the fascial septum [3].
These perforators arise between the brachioradialis and pronator teres muscles in the proximal third of the forearm and between the brachioradialis and flexor carpi radialis muscles in the distal two-thirds. Distally, one or two of these perforators may be between the tendons of the flexor carpi radialis and flexor digitorum superficialis muscles. These forearm perforators within the fascial plexus are oriented predominantly along the longitudinal axis in the forearm and transversely in the carpal [4, 5]. The distal radial artery issued about ten small branches (0.3–0.8 mm in diameter) extending from 1.5 cm above the radial styloid process to the bifurcation of the radial artery. These perforators pass through the septum, fan out on both surfaces of the deep fascia, and form a rich, chain-linked longitudinal plexus of the integument along the course of the main artery, the septum, the fiber of the deep fascia, and the superficial vein. The venous system of the deep fascia drains blood to the profunda venae comitantes directly through the concomitant perforating veins. The distal pivot point of the pedicle was located 1.0–1.5 cm proximal to the radial styloid process (Fig. 10.1).
Fig. 10.1
Vascular anatomy of the radial artery
10.2 Illustrative Case
Case 1: Proximal Perforator-Based Flap
A 29-year-old man was involved in an industrial accident that resulted in an injury to the distal third of his dorsal forearm, with tendon and skin loss (Fig. 10.2).

Fig. 10.2
Preoperative view

A distally based radial forearm fasciocutaneous flap, from the radial aspect of the middle-third forearm and nourished by a perforator from the middle radial artery, was designed to cover the defect. The flap size was 12 by 8 cm (Fig. 10.4).
Fig. 10.4
Schematic drawing of the flap design
The flap was elevated and visualized the perforator vessels (Figs. 10.5 and 10.6).
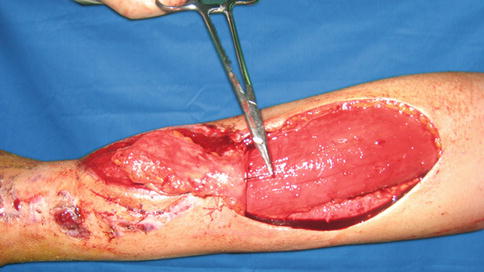
Fig. 10.5
Flap elevation
Fig. 10.6
Schematic drawing of the flap elevation
Flap Transfer
The flap was transferred to cover the defect. The donor-site wound was resurfaced with a split-thickness graft (Fig. 10.7).

Fig. 10.7
Flap transfer
Follow-Up

Case 2: Radial Styloid Perforator-Based Flap
An injury to this 27-year-old man’s hand resulted in soft tissue defects on the dorsum of the thumb (Fig. 10.9).

Fig. 10.9
Preoperative view

A 10 × 3 cm radial forearm perforator flap without radial artery was designed in the distal two-thirds of the forearm. The distal perforator pedicle was located 2 cm proximal to the radial styloid process (Fig. 10.11).
Fig. 10.11
Schematic drawing of flap design
Flap Elevation
After identifying the distal perforator, a 3 cm wide adipofascial was kept around the tiny vessel to prevent it from stretching. It is a perforator-plus flap (Fig. 10.12).

Fig. 10.12
Flap elevation
Flap Transfer and Insetting
The flap was rotated 180° to cover the defect. The donor site was closed with skin grafts (Fig. 10.13).

Fig. 10.13
Flap transfer and insetting
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


