, Shimin Chang2, Jian Lin3 and Dajiang Song1
(1)
Department of Orthopedic Surgery, Changzheng Hospital Second Military Medical University, Shanghai, China
(2)
Department of Orthopedic Surgery, Yangpu Hospital Tongji University School of Medicine, Shanghai, China
(3)
Department of Microsurgery, Xinhu Hospital Shanghai Jiao Tong University, Shanghai, China
The posterior interosseous artery flap was firstly introduced by Zancolli and Angrigiani [1] and Penteado et al. [2].
The reverse pedicle posterior interosseous artery perforator (PIOAP) flap is an extremely useful tool for hand coverage.
12.1 Vascular Anatomy
The posterior interosseous artery courses distally in the septum between the extensor digiti minimi and extensor carpi ulnaris muscles and gives off interstitial arteries (usually 3–8 septocutaneous perforators) that run perpendicular to the skin on the dorso-ulnar aspect of the forearm [3].
The distally based posterior interosseous artery pedicle flap is based on a direct communication to the dorsal branches of the anterior interosseous artery, which is 2.5 cm above the wrist level. This direct anastomosis is a very consistent finding that was confirmed in 97.1–100 % of cadaveric limbs [2, 4–8]. The distal-most perforator, located 2–3 cm above the ulnar styloid process, is usually selected as the pivot point for distal PIA perforator-based flap for hand reconstruction (Fig. 12.1).
Fig. 12.1
Vascular anatomy of the posterior interosseous artery
12.2 Illustrative Case
A 39-year-old man suffered a heat-press injury over his dorsum of the hand. The wound was extensive after debridement of the full-thickness eschar, measuring 11.0 × 7.0 cm (Fig. 12.2).

Fig. 12.2
Preoperative view
Flap Design
The flap was designed along the axis line between the extensor condyle of the humerus and the radial side of the ulnar head (Fig. 12.3) and centered around the perforating site preoperatively examined with a Doppler probe, usually 2.5 cm above the ulnar head (Fig. 12.4).
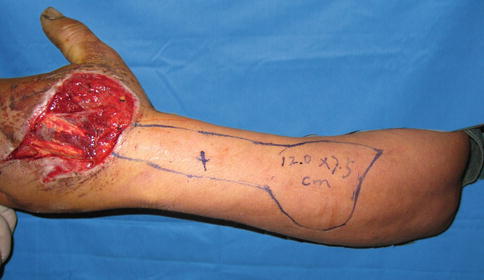
Fig. 12.3
Flap design
Fig. 12.4
Schematic drawing of flap design
Flap Elevation
Firstly, the ulnar subcutaneous tissue of the flap was incised to the deep fascial surface, the flap was then raised above the deep fascia, then the perforator was identified and preserved. The whole flap was raised, keeping the interosseous artery intact in the deep septum. The cephalic vein was protected carefully in the radial side; the forearm posterior cutaneous nerve was exposed and kept intact (Fig. 12.5).

Fig. 12.5
Flap elevation
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


