| Functional ptosis affecting vision |
| Cosmetically displeasing ptosis |
| Amblyopia in visually maturing children |
| Ptosis affecting prosthesis function in the anophthalmic socket |
| Prior facial surgery or trauma |
| Dry eye symptoms/lagophthalmos present |
| Quality of Bell’s phenomenon |
| Prior refractive surgery |
| Co-existent dermatochalasis and/or eyebrow ptosis |
| Amount of levator function |
| Need to avoid posterior conjunctival ptosis repair (i.e., strabismus, glaucoma filtration surgery/drainage device, cicatricial conjunctival diseases, fornix shortening) |
| Degree of ptosis present |
| Rule out myasthenia gravis |
| Presence of Hering’s law/contralateral ptosis |
| Desire for upper eyelid crease (particularly with Asian patients) |
| Potential for revision/asymmetry |
Introduction
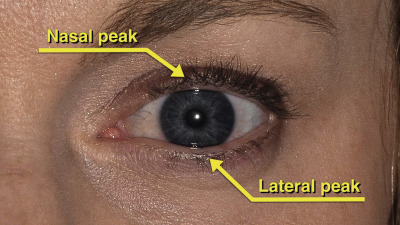
The normal position and contour of the eyelids must be recognized before undertaking ptosis repair. The position of the upper and lower eyelids is defined by the margin to reflex distance (MRD), which is the distance from the central corneal light reflex to the upper eyelid (MRD1) and the lower eyelid (MRD2). The definition of functional ptosis varies by source, but in general it is less than or equal to 2.5 mm. In the upper eyelid the contour of the lid is characterized by a peak that is nasal to the central corneal light reflex, while in the lower eyelid this peak is lateral ( Figure 11.1 ).
The evaluation of the ptosis patient begins with the classification of the specific subtype. Aponeurotic or involutional ptosis is the most common type and is caused by disinsertion of the levator aponeurosis. Myogenic ptosis is associated with a dysfunctional levator and can be seen with myasthenia gravis, chronic progressive external ophthalmoplegia (CPEO) and congenital ptosis. Neurogenic ptosis may be caused by cranial nerve III palsy or Horner’s syndrome. Mechanical ptosis is associated with an eyelid mass.
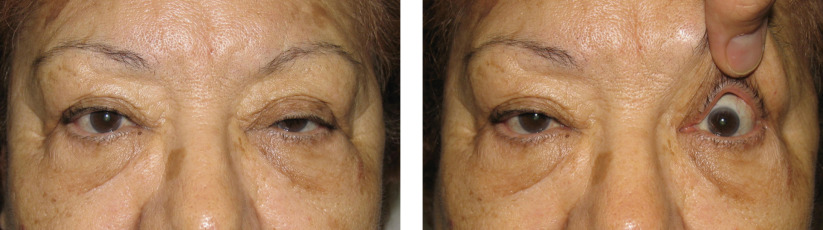
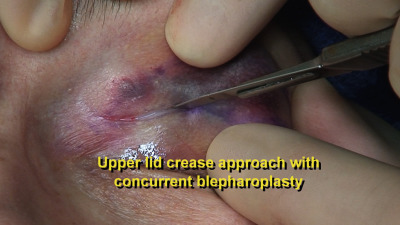
The MRD1, upper eyelid crease position and levator function are documented during the evaluation. Normal levator function is at least 12 mm of upper eyelid excursion. Hering’s law should be tested in cases of presumed unilateral ptosis. The ptotic eyelid is manually elevated and the MRD1 of the fellow eyelid is recorded. If the fellow eyelid falls after lifting of the ptotic eyelid, bilateral ptosis exists ( Figure 11.2 ). Failure to treat contralateral ptosis with a Hering’s response can result in a postoperative surprise. Ptosis associated with decreased levator function may be addressed by levator resection ( Chapter 14 ) or frontalis suspension ( Chapter 15 ) depending on the amount of levator function. The anterior approach, external levator advancement procedure, is ideal for patients with normal levator function and severe ptosis (MRD1 <1.5 mm). With the anterior approach, there is no conjunctival incision, which is relevant with patients who may need or have had glaucoma filtration surgery or strabismus surgery, or those with cicatricial conjunctival disease. The surgery does require patient cooperation to achieve optimal eyelid position and is not optimally performed under general anesthesia.
Preoperative Evaluation
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


