Fig. 7.1
Prurigo nodules. Courtesy of Julia R. Nunley, M.D.

Fig. 7.2
Excoriations in various stages of healing. Courtesy of Julia R. Nunley, M.D.

Fig. 7.3
Extensive excoriations. Courtesy of Julia R. Nunley, M.D.
Despite potentially severe itch, there is often a marked absence of clinically apparent inflammation within the skin. Skin changes in patients with CKD may simply reflect the mechanical damage from continuous scratching including excoriations, altered skin pigmentation, secondary prurigo nodularis, and lichenification or thickening of the skin. In some cases patients may also have eczematous changes or superimposed infections such as impetigo which results from barrier disruption [52].
Differential Diagnosis
Given the high prevalence of renal itch in patients undergoing HD, this diagnosis must be considered in any CKD patient presenting with pruritus. As many patients with CKD suffer from other medical comorbidities or primary cutaneous diseases, a thorough evaluation must be undertaken for each patient to identify the cause of itch on an individual basis.
Xerosis is a very common condition observed in CKD patients and may contribute to symptoms despite not being the primary cause of renal itch [51, 53, 54] in more severe cases. Xerosis alone is the cause of mild itch in the occasional CKD patient. In such cases, the itch may respond well to emollients [55].
Acquired perforating disorders such as perforating folliculitis, Kyrle disease (KD), and reactive perforating collagenosis occur in 4.5–10 % of CKD patients [56–58] and may often be confused by nondermatologists for prurigo nodularis.
Arteriovenous (AV) shunt dermatitis, which results from venous flow obstruction or flow reversal, causes hyperpigmentation and thickening of skin resembling chronic venous stasis changes. AV shunt dermatitis occurs in up to 8 % of patients on chronic dialysis (58–60) and must be distinguished from lichenification or other secondary skin changes due to renal itch as well as allergic contact dermatitis due to materials used during dialysis sessions.
Infections, infestations, and underlying systemic disorders must also be considered in the differential diagnosis of CKD patients with itch, in part due to an impaired cellular immunity that predisposes this population to such conditions [53, 59]. For example, scabies causes intractable pruritus and may often go undiagnosed or inadequately treated in CKD patients [60]. Viral infections such as hepatitis C virus (HCV) and human immunodeficiency virus (HIV) may be associated with chronic itch and should be considered in the differential of renal itch. Systemic causes of pruritus such as lymphoma, cholestasis, or hypersensitivity reactions to medications must be ruled out in CKD patients with chronic itch.
The following criteria [51] have been proposed to help in making the diagnosis of renal itch: (1) Pruritus appears shortly before the onset of dialysis, or at any time, without evidence of any other active disease that could explain the itch. (2) Patients experience episodes of itch three or more times during a period of less than 2 weeks, with the symptom appearing several times a day, lasting a minimum of a few minutes, and causing distress to the patient. (3) Appearance of an itch in a regular pattern during a period of 6 months, but less frequently than listed above.
Diagnostic Evaluation
A standard work-up to evaluate a patient with chronic itch includes basic laboratory examination to screen for systemic disorders that may be associated with itch, e.g. lymphoma and other malignancies, polycythemia vera, cholestasis, thyroid disease, diabetes, or HIV. Tests include a complete blood count with differential, serum creatinine and blood urea nitrogen values, serum bilirubin (direct and indirect), serum aminotransferases and alkaline phosphatase, thyroid-stimulating hormone and thyroxin, fasting glucose value, HIV antibody test (in high risk individuals), HCV screening and evaluation of iron stores, stool for occult blood, and serum protein electrophoresis and immunofixation. Assessment of patients in which there is a high suspicion of a diagnosis of renal itch should also include laboratory evaluation of calcium, phosphorus, and parathyroid hormone, as these values are frequently abnormal in patients with severe renal itch.
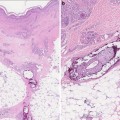
A chest X-ray may also be considered to screen for malignancy or infectious etiologies. A skin biopsy may be performed to distinguish between primary inflammatory and secondary skin changes, although is usually nondiagnostic in cases of renal itch.
Treatment (Table 7.1)
Table 7.1
Therapeutic approaches to the itch of chronic kidney disease
Treatment | Comments/recommendations |
|---|---|
Optimize dialysate | Correct electrolyte imbalances Target KtV ≥1.5 |
Emollients | Creams or bland ointments 10 % urea plus dexpanthenol lotion Sericin cream |
Topical analgesics | Pramoxine 1 % lotion twice daily |
Antihistamines | Hydroxyzine 10–25 mg PO 2–4 times daily |
Mast cell stabilizers | Cromonlyn sodium 4 % cream or 135 mg PO three times daily |
Anticonvulsants | Gabapentin 100–400 mg up to three times weekly after dialysis |
Antidepressants | Mirtazapine 7.5–30 mg PO daily |
Opioid antagonists/antagonists | Nalfurafine 5 μg IV after dialysis |
Phototherapy | Narrowband UVB phototherapy three times weekly |
Renal transplant | Usually curative |
At present, other than transplantation, no therapy has proven widely effective in the management of renal itch. Most treatment recommendations for this condition are based on case series or small, uncontrolled clinical trials; therefore an individualized, stepwise approach based on response to therapy should be undertaken. Reduced itch has been reported following increases in the daily dialysate volume, time, and frequency of dialysis [20, 61], treating underlying hyperparathyroidism, hyperphosphatemia and lowering calcium phosphate levels [16, 17]. A recent 5 year prospective cohort study of HD patients found that HD with the target of Kt/V ≥ 1.5 and the use of high flux dialyzer was effective in reducing the intensity of renal itch [62]. Despite some controversy surrounding the role of these measures in renal itch, optimizing dialysis conditions and correction of electrolyte imbalance should be considered initially.
Patients with CKD, and in particular renal itch, often suffer from xerosis which may exacerbate their symptoms. Regular use of emollients is thus recommended to preserve the integrity of the skin barrier and to reduce water loss and exposure to environmental irritants [54]. While there are no specific studies that compare the efficacy of different types of emollients in patients with renal itch, application of a high water content emollient and an emollient containing structured lipids with endocannabinoids have been demonstrated to be beneficial in two separate small studies [55, 63]. A pilot trial performed on 15 HD patients with topical application of a lotion containing urea plus dexpanthenolim proved both skin dryness (evaluated by scoring scaling roughness, redness, and cracks on the skin) and itch. A recent double-blind trialin 50 HD patients found that application of a cream containing sericin, a water-soluble, high molecular weight biopolymer derived from silk worms, to effectively decrease skin irritation, hyperpigmentation, and itch compared to placebo [64]. Sericin contains 32 % serine, the primary aminoacid of natural moisture factor in human skin [65]. Sericin also has anti-inflammatory properties and decreases levels of tumor necrosis factor alpha (TNF-α) and IL-1β [66]. Emollients with higher lipid content such as ointments and creams are generally preferred over lotions or gels, as they provide superior occlusion and corneocyte hydration, promoting improved skin barrier function.
Topical analgesic agents, including pramoxine and capsaicin, have been used with some success in renal itch. A lotion containing 1 % pramoxine has been shown to be effective in renal itch [67]. In one study, 28 HD patients with moderate to severe renal itch applied 1 % pramoxine lotion twice daily for 4 weeks and a significant reduction in itch intensity was observed in the treatment group (61 %) compared to controls (12 %). Topical capsaicin has been reported to be successful in some patients with renal itch, but studies regarding its efficacy are conflicting. It is frequently discontinued by patients due to a burning sensation following initial applications such that it is not recommended as a first line topical agent, especially in patients with generalized itch or involvement of large skin areas [68–72].
Studies regarding the use of immunomodulators are not conclusive. Topical tacrolimus has been studied but the results are controversial and show limited benefit [39, 40]. It is not recommended for prolonged use in renal itch patients. While frequently attempted in the treatment of renal itch, no studies have formally evaluated the effectiveness of steroids for this condition.
Oral antihistamines have been classically used for the treatment of all types of chronic itch. Mast cell stabilizing effects of antihistamines have been implicated as their potential beneficial mechanism in renal itch. Both oral (135 mg three times daily) and topical (4 % cream) cromolyn sodium (CS) have been shown to effectively reduce itch in HD patients [73, 74]. It is not clear that decreased levels of specific mast cell mediators are responsible for the beneficial effects of these agents. As CS poses minimal harm and has only rare side effects, some studies recommend using it before initiating other antihistamines or neuroleptic agents for the treatment of renal itch [73]. As evidence that renal itch is histamine-mediated is lacking, the sedative properties of most antihistamines are probably responsible for itch relief in the limited number of patients responding to these agents. A trial of sedating antihistamines such as hydroxyzine (10–25 mg, 2–4 times daily by mouth) may be tried in CKD patients considering their low side effect profile.
Most patients suffer from persistent itch despite optimizing dialysis conditions and initiating regular antihistamine therapy. For these patients, low dose treatment with gabapentin and pregablin should be considered as the next therapeutic step. Although their exact mechanism in decreasing itch is unknown, these neuroleptic agents, analogs of the major inhibitory neurotransmitter γ-aminobutyric acid (GABA), are postulated to inhibit itch pathways in both the peripheral and central nervous systems, similar to their action in treating chronic pain and sensory neuropathies [75]. Different treatment regimens for gabapentin, including 300 mg after each dialysis session [76] and 400 mg twice weekly [77] have been reported to be effective. Caution is advised when starting these agents, as dizziness and somnolence are frequently encountered side effects.
Selective serotonin reuptake inhibitors (SSRIs) and selective norepinephrine reuptake inhibitors (SNRIs) have been used in the treatment of systemic itch. They are postulated to decrease itch by reducing central sensitization through alterations of both serotonin and α2 noradrenergic receptors [75]. Mirtazapine has been shown to reduce nocturnal itch and is favored by some clinicians for the treatment of renal itch [78, 79].
Systemic therapy with opioid modulators has been used in the treatment of renal itch. There are conflicting data regarding effectiveness of μ-opioid antagonists such as naltrexone in renal itch. A study performed in 15 HD patients suggested short-term efficacy of naltrexone in ameliorating renal itch [48], while a subsequent study in 23 patients did not find any statistically significant difference between naltrexone and placebo in alleviating renal itch [49]. μ-opioid antagonists must also be used with caution, as they may worsen pain caused by comorbid conditions in CKD patients. A meta-analysis of two multicenter, randomized, double-blind, placebo-controlled trials showed decreased itch and sleep disturbance in HD patients after intravenous postdialysis administration of 5 μg of nalfurafine, a selective κ-opioid agonist, compared with placebo (36 versus 14 % respectively) [50]. Butorphanol, a κ-opioid agonist and partial μ-antagonist, has shown some benefit in treating some cases of intractable itch, although not specifically renal itch [80].
UVB phototherapy has been demonstrated to be effective for renal itch and is probably vastly underutilized. Potential limitations include access to an office that provides this therapy in which case use of home phototherapy units should be considered. UVB irradiation appears to alter skin sensitivity to pruritogens and decrease the level of proinflammatory cytokines [81, 82]. In an open pilot study of 20 patients with renal itch, narrowband UVB phototherapy was performed (maximum daily dose of 1,500 mJ/cm2) over a 6-week duration [83]. Eight of ten patients who completed the treatment duration experienced reduction in itch. Symptoms recurred in four of the eight responders after cessation of UVB treatment. UVB has a minimal risk of carcinogenesis in the therapeutic treatment of inflammatory skin conditions such as psoriasis but this risk in the CKD population has not been evaluated.
Renal transplant is the only definitive treatment for patients with refractory itch not responding to these therapeutic options [6]. Relaxation techniques and behavioral therapies may be considered as adjunctive options in patients with psychogenic itch components.
Prognosis
Renal itch has a major negative impact on the quality of life of CKD patients. Patients with moderate to severe pruritus had a 13 % higher mortality risk compared to those not affected by renal itch, in DOPPS I and a 21 % higher risk in DOPPS II and an overall higher mortality risk of 17 % [1]. The exact underlying mechanism of renal itch is still unknown and no drug specifically targets this type of itch. Several compounds, including additional κ-opioid agonists, are being evaluated for the treatment of CKD itch. Combined with advances in understanding itch signaling pathways and dysregulation of the neuro-immune axis, better treatments for patients with CKD or renal itch are on the horizon.
Acknowledgments
This work has been supported by grants from the NIH, R01AR057744 and Leo Pharma to EAL and by the Dermatology Foundation to SBE.
References
1.
2.
Mathur VS, Lindberg J, Germain M, Block G, Tumlin J, Smith M, et al. A longitudinal study of uremic pruritus in hemodialysis patients. Clin J Am Soc Nephrol. 2010;5(8):1410–9 [Comparative Study Multicenter Study].PubMedCentralPubMedCrossRef
3.
4.
Wang H, Yosipovitch G. New insights into the pathophysiology and treatment of chronic itch in patients with end-stage renal disease, chronic liver disease, and lymphoma. Int J Dermatol. 2010;49(1):1–11 [Research Support, N.I.H., Extramural Review].PubMedCentralPubMedCrossRef
5.
Chen HY, Chiu YL, Hsu SP, Pai MF, Lai CF, Yang JY, et al. Elevated C-reactive protein level in hemodialysis patients with moderate/severe uremic pruritus: a potential mediator of high overall mortality. Q J Assoc Phys. 2010;103(11):837–46 [Research Support, Non-U.S. Gov’t].
6.
Altmeyer P, Kachel HG, Schafer G, Fassbinder W. Normalization of uremic skin changes following kidney transplantation. Hautarzt. 1986;37(4):217–21.PubMed
7.
Dhand A, Aminoff MJ. The neurology of itch. Brain. 2013;22.
8.
Schmelz M, Schmidt R, Bickel A, Handwerker HO, Torebjork HE. Specific C-receptors for itch in human skin. J Neurosci. 1997;17(20):8003–8 [Research Support, Non-U.S. Gov’t].PubMed