div class=”ChapterContextInformation”>
46. Penile Prosthesis Implantation in Complex and Previously Failed Settings
Keywords
Implant revisionCorporal fibrosisStenotic corporaPriapismImplant infectionHypermobile glansImpending erosionCavernotomes46.1 Introduction
Most prosthetic surgeons would agree that a patient’s first implantation surgery offers the highest likelihood of success. Dr. John Mulcahy opines that “The penis gets shorter with each operation and the patient unhappier.” Nevertheless, despite being the least likely to need a revision of all the medical devices implanted into humans [1], a distinct chance remains that a reoperation will be necessary. The most common reasons for revision surgery include mechanical failure, followed by patient dissatisfaction [2–5]. Long-term data regarding mechanical failure demonstrates 96% survival at 5 years, 80% survival at 10 years, and 70% survival at 15 years for inflatable penile prosthesis (IPP) implantation [1, 6]. It is important to review these figures when counseling patients preoperatively, particularly younger patients who will likely require a revision surgery for device failure within their lifetime. The most common cause of mechanical failure is a fluid leak from the device, while supersonic transport deformity, aneurysm of the cylinders, impending lateral extrusion, and desire for upsizing the cylinders are additional reasons for revision surgery [7].
While revisions for mechanical failure and patient dissatisfaction are relatively routine surgical procedures, penile prosthesis implantation in previously failed settings is daunting, even for the experienced implanter. The surgical planes are altered and obliterated by scar. To maximize success, specialized instruments, downsized implants and lots of experience are necessities. Even experienced implanters without these assets have only a 50% chance of success. Even if a surgical victory is achieved for the surgeon, the patient may be unhappy about his loss of length.
Our senior author has 45 years of experience with thousands of reoperations and reinsertions. Many of his recommendations outlined in this chapter have never been published. This chapter is meant as a guide to the focused implanter for navigating the tricky pathways of redo of multi component prosthetics. We hope to help the reader prevent mistakes and reward realistic patient expectations in this difficult surgery on discouraged patients. To facilitate your learning of essential caveats and previously unpublished ideas regarding this complex prosthetic surgery, we have used bold print to illuminate them.
46.2 Preoperative Evaluation
The initial consultation is an opportunity for the prosthetic surgeon to gather as much information as possible regarding the patient’s medical comorbidities, previous surgical history, physical exam, and expectations for their revision surgery. We would advocate a “plan for the worst, hope for the best” approach as many of the most common challenges can be anticipated upon preoperative work up.
46.2.1 Imaging

Pre-operative CT scan demonstrating intra-peritoneal IPP reservoir
46.2.2 Physical Exam
In addition to a thorough history, the physical exam provides invaluable information that can help in operative planning. We recommend the patient be examined in the supine position and in the frog leg position. Careful palpation at the level of the proximal corporal bodies after a recent explant for infection may reveal cement like fibrosis preparing the surgeon for the need for special instruments. Similarly, post priapism patients often will demonstrate very scarred distal corporal bodies that are easily palpable. Scars from previous surgeries are typically visible in the lower abdominal and scrotal areas, particularly if an infrapubic approach was used. The site of the exit tubing is also typically palpable in the infrapubic approach, especially in thin patients. In situations where either a horizontal infrapubic, or midline vertical lower abdominal incision is visible but exit tubing is not palpable, the incision may represent a counterincision used for reservoir placement rather than the cylinders themselves. Surprisingly enough, the patients are frequently no help in telling you where the incision was made! IPP revisions occur years after the original implantation and patients simply forget. Accessing the corporotomy site at the level of the exit tubing in an infrapubic IPP can be more challenging from a penoscrotal approach, therefore the surgeon may consider using the same approach used to place the original device to provide more direct access to remove all of the components. This may not be true in the setting of infection in which case it may be advisable to use a penoscrotal approach where there is less scar tissue from a previous implant placed using an infrapubic approach.
There is always the danger of damage to the dorsal nerve of the penis in reoperations done through an infrapubic incision. The anatomy is not so clear in return operations as it was in the virgin implantation. In our experience, the pump and cylinders of an infrapubic placed device can be completely extracted via scrotal incision, including the tubing boots on American Medical Systems (AMS) devices . The authors commonly make corporotomy distal to tubing exit and remove the cylinder, boots and tubing retrograde by a forceful pull of the cylinder body. If the reservoir must be removed e.g. infection, a separate abdominal incision must be made but there is no danger of dorsal nerve injury from this incision.
Attempts to cycle the device will generally provide useful information in all cases requiring revision. Fluid leak in the system is obvious as air causes turbulence as it cycles through the pump. “Sticky pump syndrome” is demonstrated by difficulty inflating or deflating the device [8]. If the indication for revision is patient dissatisfaction, cycling the device provides an opportunity to discuss the patient’s grievances and expectations including location of the pump, palpable exit tubing, device sizing, floppy glans, supersonic transporter (SST) deformity, and pain with inflation.
New onset urinary symptoms after IPP warrants evaluation with urinalysis, pressure-flow study, post void residual, and cystoscopy to rule out erosion. Cystoscopy usually demonstrates external compression of the bladder due to the reservoir, particularly in patients with large cylinders that require a larger volume reservoir. This is of no consequence to a knowledgeable implanter unless the surface of reservoir is visible. This distortion may also be noted on CT imaging where the bladder is displaced medially due to a large reservoir. CT should not be considered as a substitute for a cystoscopy to rule out erosion. Additional considerations include external compression by the exit tubing or pump relative to the urethra in cases of obstructive urinary complaints.
46.2.3 Patient Counseling
Setting realistic patient expectations is critical to patient satisfaction. Prosthetic surgeons should have a thorough discussion with the patient regarding what to expect in the perioperative course including post-operative recovery time, risk of infection, and penile length.
In our experience, patients typically report a shorter recovery time than their initial surgery, likely because less dissection is required as the corpora have previously been dilated. They should be counseled about the potential need for a counterincision to remove the old reservoir in the case that it cannot be retrieved through the primary incision or in the event that the reservoir had be placed in an abdominal wall location.
The risk of infection in revision surgery is an important discussion point during preoperative counseling, particularly in patients who are dissatisfied due to a minor imperfection, but in whom the device is functional. The decision to hastily proceed to the operating room for revision of a device due to pump location, palpable or visible tubing and other aesthetic considerations should be avoided as it is likely not worth the risk of an infection. Depending on the nature of the patient’s complaint, a trial period of 6–12 months should always be urged prior to scheduling the patient for revision surgery as the patient may be more willing to accept certain imperfections over time. Our senior author’s admonition is “never rush to revision.”
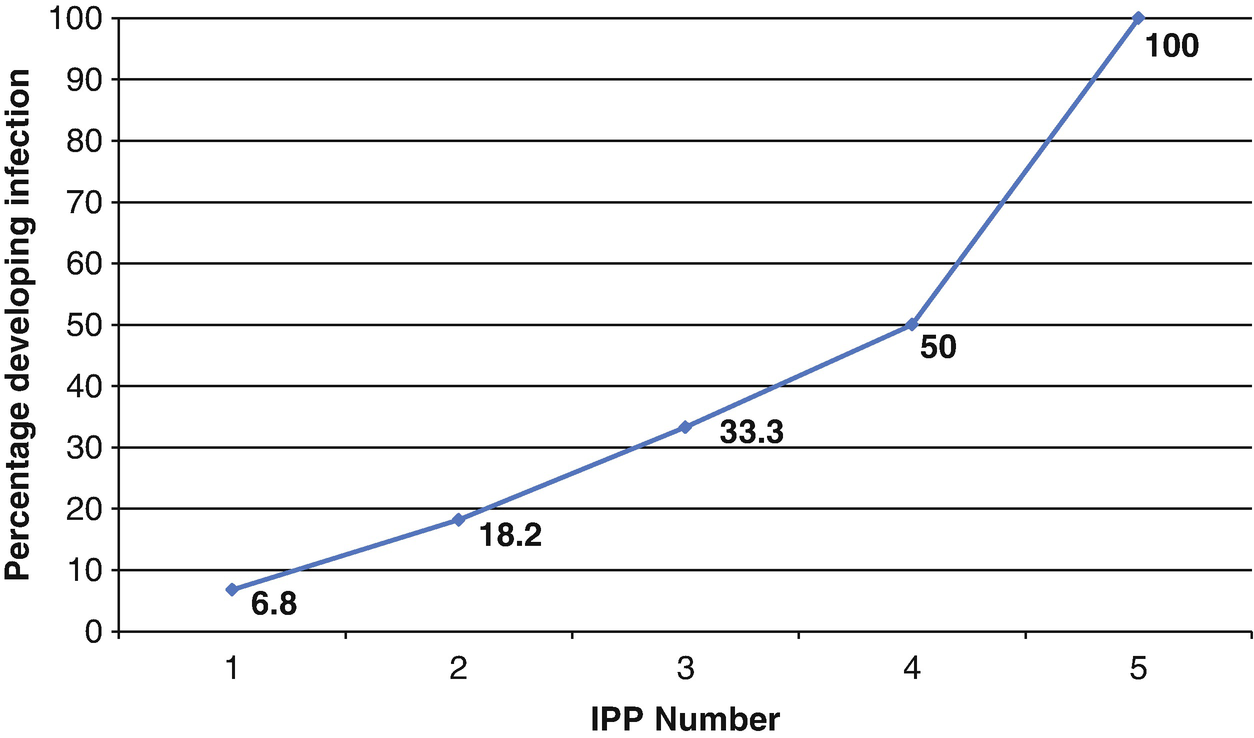
Percentage of patients developing an infection with most recent device based on the IPP device number (Pearson Correlation Coefficient R2 = 0.90, p = 0.01). As an example, 50% (4/8) of patients on their 4th IPP revision in this historical series developed infection. (Adapted from Ref. [15])
Penile length is a common concern in IPP surgery, both in the primary and revision settings. Patients who have an IPP that is correctly sized and in place at the time of revision, can expect at the very least to maintain their current penile length. Typically, the implant space within the corpora will accommodate a slightly larger device than their previous cylinder size, allowing for upsizing of the device at time of revision. However, despite longer cylinders, the patient typically does not note a clinical length difference but may notice an increased girth if the new device allows for greater lateral expansion. Appreciation of improved penile girth is noted commonly, if an AMS cylinder is removed and a Coloplast cylinder substituted.
Patients in whom the device was explanted due to infection or erosion no longer have an implant in place. They can expect loss of length, sometimes to a devastating degree. The corpora of these patients are typically fibrotic and may be difficult to dilate, particular in post-infection cases. Patients who are likely to have corporal fibrosis due to history of prolonged ischemic priapism, diabetes, Peyronie’s disease, trauma, or intracavernosal injection therapy for erectile dysfunction should also be identified and counseled accordingly in the preoperative setting [17, 18] …. “We will give you a functional device, but it will not look or perform like it did before you had the infection.” This discouraging news, however, can be tempered by these words. “After 8-12 months of a daily inflation protocol, the device will act as a tissue expander. The cylinders will be too short and too thin. Then we can go back in and place a longer and wider cylinder.”
Patients with a functional IPP in place, who are pending revision surgery for this upsizing, should be advised to inflate their device daily to the point of discomfort and leave it inflated for several hours. This regime will assist in maximizing penile length and girth [19]. Those who do not have a penile implant in place should be encouraged to use a vacuum erection device daily for at least 7 weeks preceding surgery in an effort to expand the improve tunical compliance, influence the intracavernosal space, possibly impact the fibrosis development, and facilitate easier dilation at the time of IPP surgery [20]. Penile stretching devices may also have a role in maximizing penile size pre-procedure.
46.3 Challenging Cases
46.3.1 Corporal Fibrosis
Corporal fibrosis is a process that involves excessive deposition of scar tissue in response to infection, trauma, or ischemia [21]. It does not occur merely as a result of previous IPP surgery. In other words, routine removal of an implant for reasons of mechanical problems, physician error or patient dissatisfaction does not result in the development of fibrotic scar tissue in the space previously occupied by erectile tissue. These scarred corporal bodies may result from disease processes such as diabetes, Peyronie’s disease and arterial insufficiency. The development of corporal fibrosis is certain after extraneous and disastrous events such as priapism or the development of a device infection.
46.3.1.1 Infection
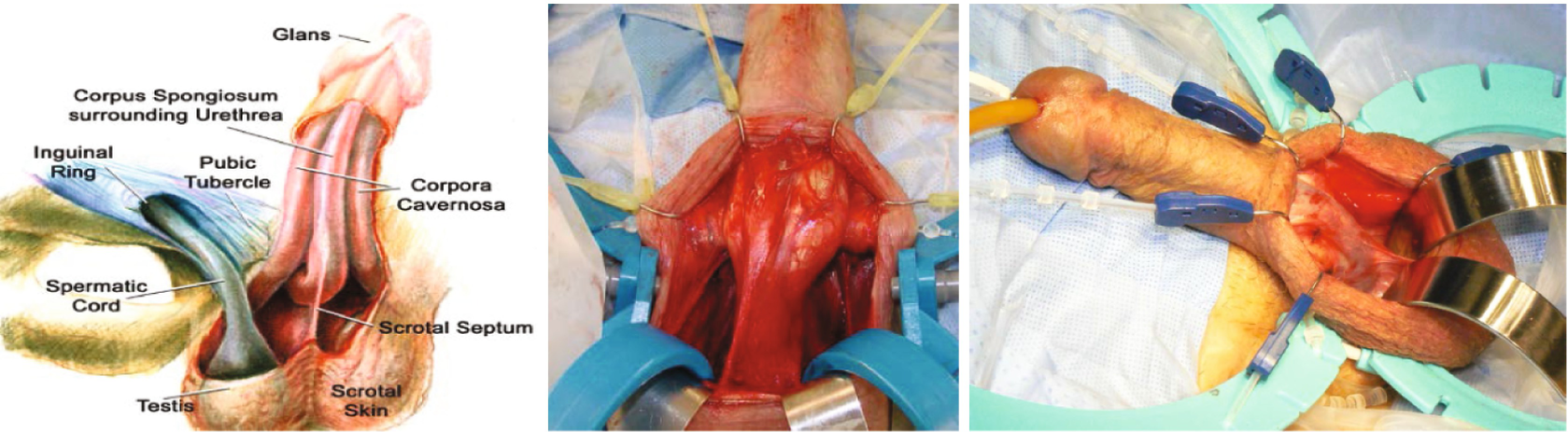
The most severe cases of corporal fibrosis occur after removal of an infected penile prosthesis, and are associated with significant penile shortening [22, 23]. Fibrosis secondary to infection is more common in the proximal corpora, making proximal dilation challenging. Dr. Karl Montague first advocated use of a transverse scrotal incision rather than vertical scrotal or infrapubic for allowing better access to the proximal corpora in difficult cases. We also recommend a generous transverse scrotal incision to maximize proximal exposure. Careful dissection to make the corpora “squeaky clean” where the lateral borders of the corpora are easily demonstrated should be undertaken. This sometimes requires clearing of tissue adherent to the corpora in the distal penis where a virgin plane is easily located. Pre-placed stay sutures both proximally and distally to the point of intended corporotomy facilitate finding the proper intracorporal space. Distal dilation should be undertaken first and is typically not too difficult. If any resistance is felt with distal dilation (more likely after priapism), extension of the existing incision or additional corporotomies should be placed. A distal counter incision is advisable in distal difficulty as the urethra is easily damaged by blind passage of small sharp instruments. Sometimes it is advisable to make the second corporotomy just under the glans so that this dilatation can be performed under direct vision (Fig. 46.3).
Never be afraid to make the second incision. The urethra is easy to lacerate when dilating distally from the proximal corporotomy. With the second incision, the dilatation is basically under direct vision
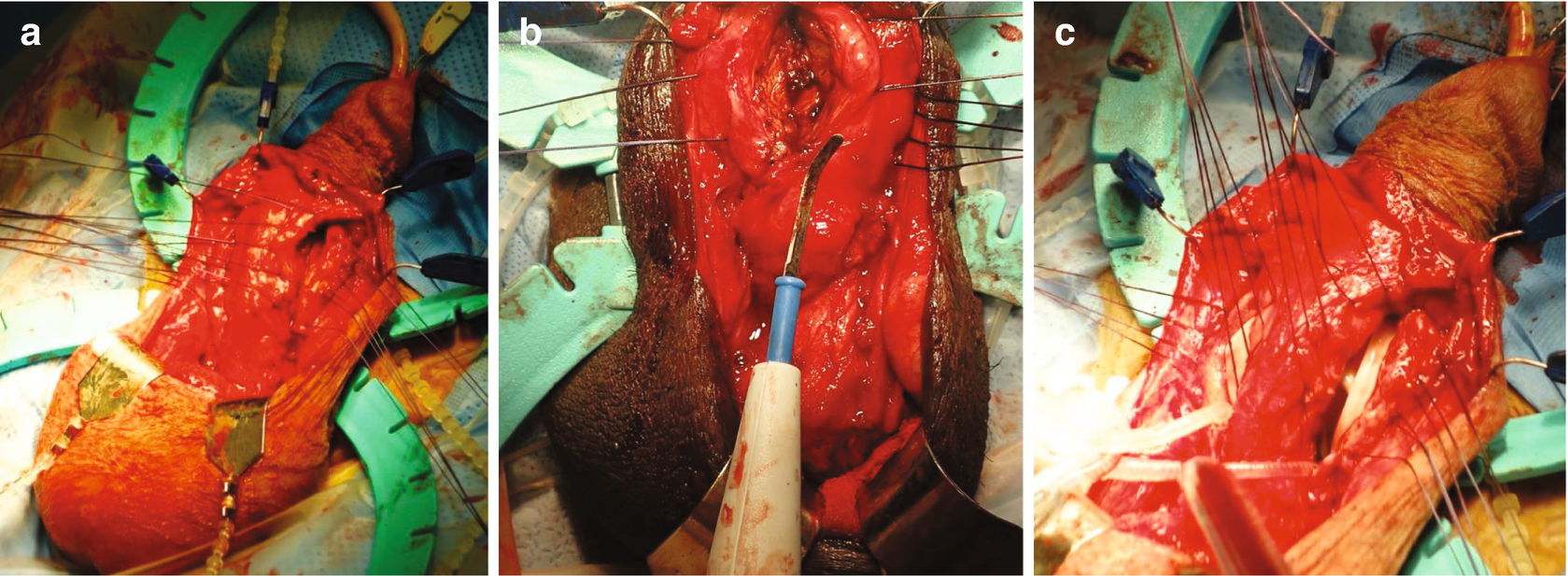
(a) Extensive corporotomy, like “the belly of a fish”. (b) Corporal excavation with electrosurgical pencil. (c) After excavation multiple stay sutures easily tied
Careful proximal serial dilation should be undertaken starting with a small dilator (6 Uramix or 8 Carrion Rossello) again erring laterally in an attempt to find the ischial tuberosity. The downside of using a small dilator is its propensity to perforate proximally where even experienced implanters have about a 50% proximal perforation rate. Suture slings as described by Wilson are commonly required (Fig. 46.5) [27]. Prior to making the initial corporotomy in a case with corporal fibrosis, the surgeon is miles ahead by first exposing the proximal corpora surface. This will facilitate proper instrument passage proximally as it will be under direct vision instead of blindly estimating the direction of the proximal corpora. Our senior author has excellent videos on the Video Journal of Prosthetic Urology web site showing how this maneuver is easily accomplished with sharp dissection and the insertion of two baby Deaver retractors (www.vjpu-issm.info) (Fig. 46.6).
This dissection and exposure of the entire proximal corpora reap benefit to help the surgeon locate the proper plane. Occasionally, one side is easily discovered and the other a challenge. Thus, if there is any doubt about the correct downward direction of the corpora on the first side, the other side should be attempted. Once the proper direction is found on one side, a dilator left in situ will help the surgeon find the other by comparison.
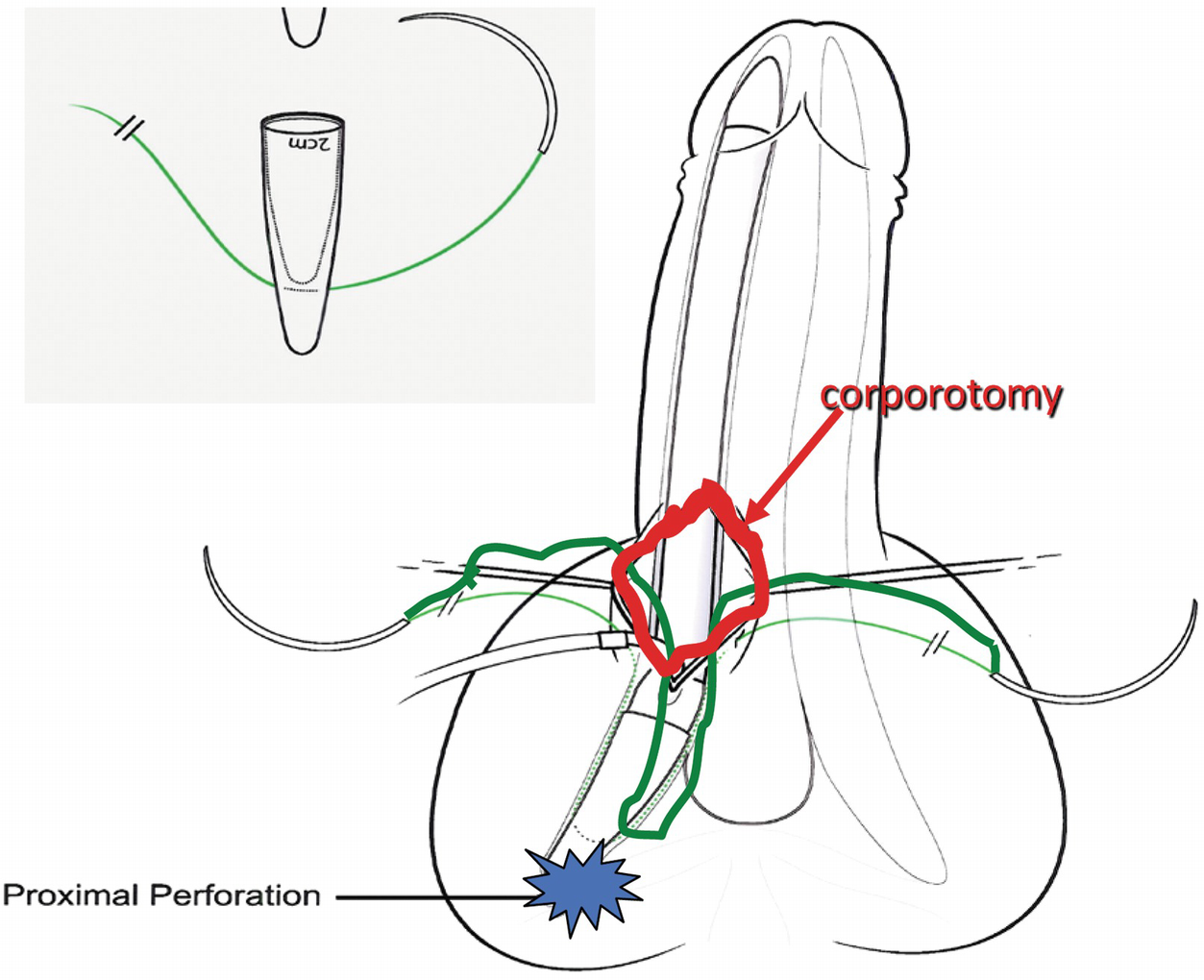
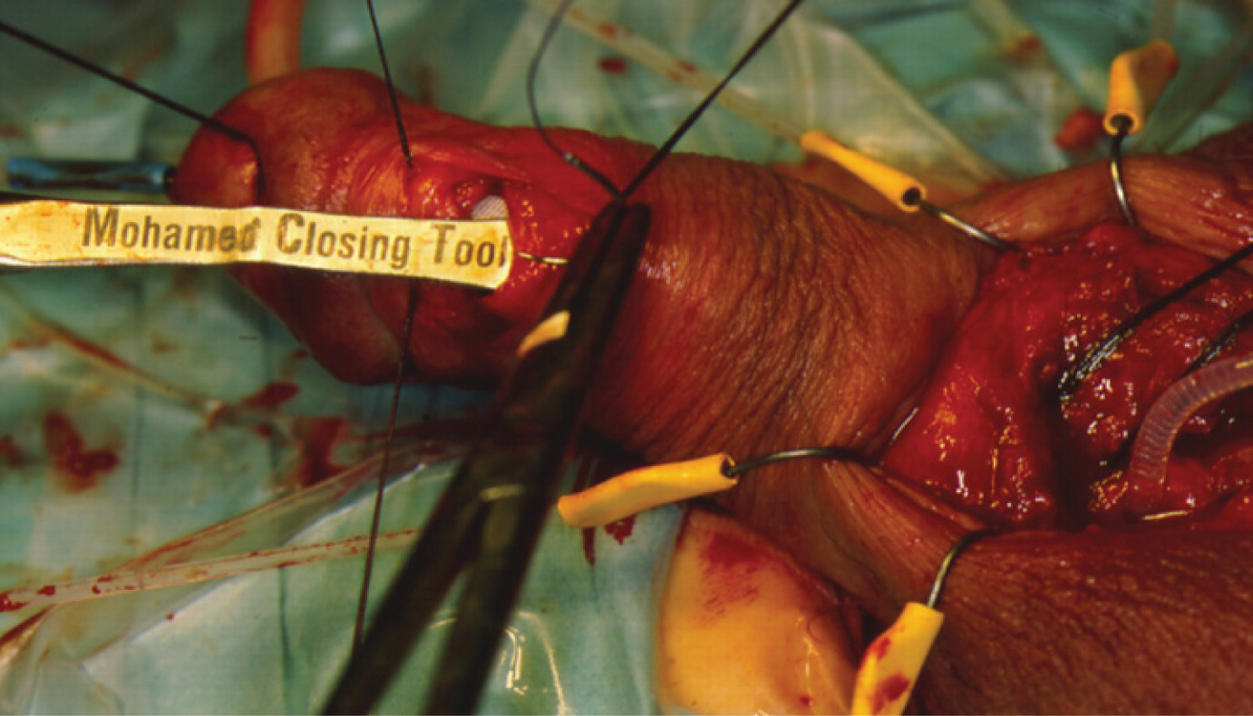
Illustration of Rear Tip Extender Sling of non absorbable suture for proximal perforation
We have needlessly struggled countless times when trying to place a standard device in this situation. It is not an admission of defeat to place a narrow cylinder. In our opinion, the best cylinder size for these difficult reinsertions is the Coloplast 16NB. This “downsized” cylinder when inflated is very close to the girth of a standard AMS 700 CX. The Coloplast 14NB and AMS 14, 16 CXR expand to a girth that is less generous. Clinical appearance of the penis is initially excellent even with narrows because of the stenotic corpora. With usage the device acts as a tissue expander lengthening and expanding girth of the scarred corpora. If the patient is dissatisfied, he can be assured that the downsized cylinders will accomplish preparation of the space for a standard size device for the next revision.
Timing to reimplantation is one of few modifiable factors to minimize the extent of fibrosis after infection. Reimplantation within 16 weeks allows sufficient time for the infection to be adequately treated, and it may be easier to identify the old corporal cavity before it becomes obliterated. A patient pending reimplantation after penile prosthesis infection should be advised to use a vacuum erection device for at least 10 minutes twice daily. Maximum stretching of the penis occurs typically by 7 weeks [20]. Figure 46.7 demonstrates a potential sequence following implant removal for infection.
46.3.2 Priapism
In contrast to corporal fibrosis associated with infection, the fibrosis encountered after priapism is most pronounced distally. While still challenging, IPP surgery in this setting is generally easier than in the post-infection cases. In contrast to the traditional transverse penoscrotal incision, a vertical midline incision is useful along the raphe with plans to extend the incision as far distally as needed for adequate exposure. Brooks dilators are preferred over Hegar dilators because instrument resistance is higher in response to narrowing. This is because the circumference of the dilator is the same over the entire length of the Hegar.
Demonstration of dissection of proximal corpora to facilitate proximal corporal dilatation. A video of this maneuver is available on www.vjpu-issm.info. Video is entitled “The Tunnel Technique”

(a) Small shrunken penis after removal of infected IPP. (b1) One year after Coloplast 11 + 5NB; SST has occurred (b2) pulling on shaft skin demonstrates cylinder too short. (c) Removal of downsized implant; note stacked RTE to facilitate insertion into proximal corpora. (d) Replacement result; 16 + 2 Standard Titan cylinder

Wilson reverse cutting scissors useful for establishing a space for cavernotome to operate within during implantation of cylinders into scarred corporal bodies. (Sontec Instruments® Centennial CO)
Related posts:
 Changing Scenario of Urethral Stricture Management
Changing Scenario of Urethral Stricture Management
 Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
Reconstruction of Penile Urethral Strictures: Single-Stage Procedures
 Reconstruction of the Lower Urinary Tract
Reconstruction of the Lower Urinary Tract
 Presentation and Diagnostic Evaluation of Male Urethral Stricture
Presentation and Diagnostic Evaluation of Male Urethral Stricture
 Urethrostomy: A Pearl in Failed Urethral Reconstruction
Urethrostomy: A Pearl in Failed Urethral Reconstruction
 Private: Reconstruction of Pelvic Fracture Urethral Injury
Private: Reconstruction of Pelvic Fracture Urethral Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


