Prospective Comparative Clinical Evaluation of 784 Consecutive Cases of Breast Augmentation and Vertical Mammaplasty, Performed Individually and in Combination
Eric Swanson, M.D.
Leawood, Kans.
From the Swanson Center.
Received for publication December 11, 2012; accepted January 31, 2013.
Copyright © 2013 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3182910b2e
Disclosure: The author has no financial interests to disclose. This study received no outside funding.
Background: Despite the growing popularity of breast lift surgery, no published study prospectively evaluates mastopexy and augmentation/mastopexy. Several investigators suggest an inordinate risk in combining augmentation and mastopexy, and recommend staging the surgery in some patients. However, no existing study includes the necessary individual and combined treatment cohorts to allow reliable comparisons of safety and efficacy. This study investigates the clinical outcomes and safety of these cosmetic breast procedures, whether performed individually or in combination.
Methods: This 10-year prospective study evaluated 759 consecutive women undergoing 784 consecutive cases of breast augmentation (n = 522), mastopexy (n = 57), augmentation/mastopexy (n = 146), reduction (n = 48), and reduction plus implants (n = 11). All patients were treated by the author using submuscular implant placement and vertical parenchymal resection with a medial pedicle and intraoperative determination of nipple positioning. A power analysis confirmed adequacy of the sample sizes.
Results: The complication rate was 36.3 percent for augmentation/mastopexy, 33.3 percent for mastopexy alone, and 17.6 percent for breast augmentation alone. Mammaplasties were complicated by persistent ptosis in 9.5 percent of patients. The revision rate after augmentation/mastopexy was 20.5 percent, compared with 24.6 percent for mastopexy and 10.7 percent for breast augmentation.
Conclusions: Vertical mammaplasty may be used to correct ptosis in breasts of all sizes. Vertical augmentation/mastopexy provides complication and revision rates that are less than the calculated cumulative rates for the procedures performed separately. The combined procedure offers technical advantages and permits safe single-stage surgery using the vertical technique. (Plast. Reconstr. Surg. 132: 30e, 2013.)
CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, II.
Breast augmentation, mastopexy, augmentation/mastopexy, and reduction are all cosmetic procedures,1 notwithstanding the physical benefits of breast reduction and mastopexy.2 Mastopexy and augmentation/mastopexy merit close evaluation because these procedures have been a source of patient and physician dissatisfaction.3–5 Despite the growing popularity of breast-lift surgery,6 a large prospective study of mastopexy patients has not been published. This clinical
study is part of a comprehensive evaluation of cosmetic breast surgery that also includes a prospective measurement study7 and outcome analysis.2,8
study is part of a comprehensive evaluation of cosmetic breast surgery that also includes a prospective measurement study7 and outcome analysis.2,8
Patients and Methods
From January of 2002 to January of 2012, 759 women underwent 784 consecutive cosmetic breast procedures (Fig. 1 and Table 1). Breast reconstruction patients were excluded.
Surgery
All procedures were bilateral. In all cases, breast implants were placed submuscularly, using predominantly the inframammary approach (95.0 percent) and saline-filled implants (94.6 percent). Resections of 300 g or more from at least one breast were categorized as breast reductions. Eleven reduction patients were simultaneously treated with implants (Fig. 2). All mammaplasties were performed by the author using the vertical technique and medially based pedicle as described by Hall-Findlay,9 but without a mosque-dome pattern; the nipple position was determined intraoperatively (Figs. 3 and 4). Sequential compression devices were used. No patient received enoxaparin.
Statistical Analysis
Statistical analyses were performed using IBM SPSS for Windows version 20.0 (IBM Corp., Armonk, N.Y.). An independent t test was used to compare means of continuous variables for two groups of patients. A one-way analysis of variance was used for more than two groups. Scheffé post hoc tests were used. The Pearson chi-square test of independence was used to compare categorical variables. The “reduction plus implants” group was not included in group comparisons because of its small sample size (n = 11). Correlations were tested using Pearson correlations. A value of p < 0.01 was considered significant. An a priori power analysis was performed for the one-way analysis of variance. To achieve 80 percent power, with an alpha level of 0.01, sufficient to detect a medium-sized treatment effect (f = 0.25)10 comparing across four groups, 256 total subjects would be needed.11
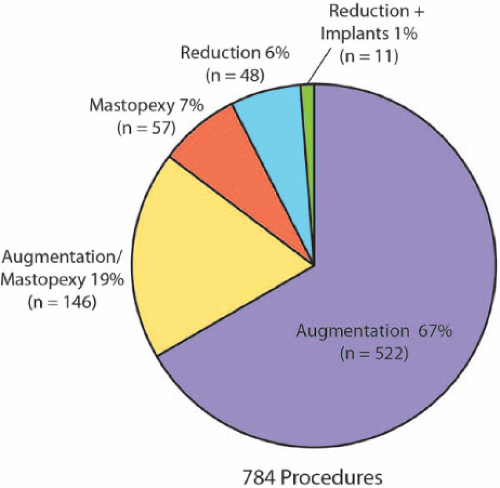 Fig. 1. Cosmetic breast surgery patients, by procedure. |
Results
Breast augmentation patients were younger, on average, than the other patients (p = 0.001). Breast augmentation patients had a lower mean body mass index and breast reduction patients had higher a mean body mass index than did the other procedure groups (p < 0.001). Mean implant volumes were significantly greater (p < 0.001) for breast augmentation (410 cc) than for augmentation/mastopexy (354 cc).
Complications
There were no major systemic complications, deep venous thromboses, or pulmonary emboli. No patient required a blood transfusion or hospital admission. Partial areola necrosis occurred in one reduction patient and healed spontaneously. There were no cases of nipple loss. The incidence of complications (Table 2) was 25.0 percent overall, and was significantly lower for breast augmentation (17.6 percent) than for vertical mastopexy (33.3 percent) and augmentation/mastopexy (36.3 percent) (p < 0.001). Based on the individual procedural risks, a cumulative complication rate of 45.0 percent was calculated for a theoretical patient treated with implants followed by mastopexy or vice versa [100 – (82.4 percent × 66.7 percent)]. There was a 20.5 percent revision rate after augmentation/mastopexy (Table 3), significantly more than after augmentation alone (10.7 percent, p = 0.001), but not as high as mastopexy alone (24.6 percent).
A significant positive correlation was detected between the incidence of complications and patient age, but this correlation was weak (r = 0.10, p < 0.01). No significant correlations were detected between the incidence of complications and body mass index, resection weights, or implant volumes. The chi-square test of independence revealed that the incidence of complications was associated with a smoking history in patients treated with augmentation/mastopexy (p < 0.01) and with secondary breast augmentations (p < 0.01), but not with secondary mastopexies.
Table 1. Patient Data* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
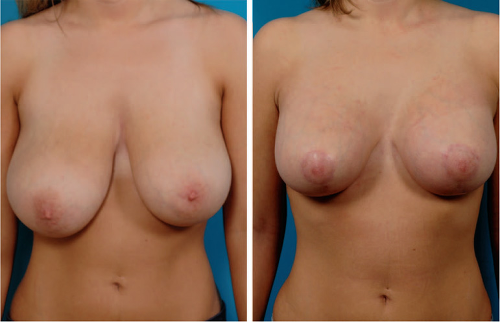 Fig. 2. Vertical breast reduction plus implants. Orientation-matched views of a 23-year-old woman (left) before and (right) 3 months after a vertical reduction using a medial pedicle and augmentation with submuscular Mentor Moderate Plus Profile saline-filled implants inflated to 240 cc. Her torso appears longer after surgery. Resection weights were as follows: right breast, 466 g; left breast, 314 g. |
Discussion
Study Design
Although breast augmentation and reduction have traditionally been considered individually, interprocedural comparisons can be useful.12 Today, we recognize an overlap in indications for these procedures and even in physical benefits.2 When a vertical technique is used, the mammaplasties are essentially the same, differentiated only by the resection weight.7
There are no published prospective clinical or outcome studies of mastopexy or augmentation/mastopexy. This deficiency is remarkable considering the popularity
of breast-lift surgery, which witnessed a 72 percent surge from 2000 to 2011,6 and by the increasing popularity of augmentation/mastopexy, an operation that is now performed more commonly than mastopexy alone in many practices.7,13 Existing studies of mastopexy14 and augmentation/mastopexy13,15–22 are all retrospective and often include multiple techniques13,15,17,18,22 and multiple surgeons.18,22 Prospective studies of consecutive patients are preferred, to avoid selection bias and confounding factors.23 A power analysis is recommended to determine the adequacy of sample sizes, to avoid type II statistical errors.24 A rigorous 0.01 alpha value reduces the risk of type I errors.
of breast-lift surgery, which witnessed a 72 percent surge from 2000 to 2011,6 and by the increasing popularity of augmentation/mastopexy, an operation that is now performed more commonly than mastopexy alone in many practices.7,13 Existing studies of mastopexy14 and augmentation/mastopexy13,15–22 are all retrospective and often include multiple techniques13,15,17,18,22 and multiple surgeons.18,22 Prospective studies of consecutive patients are preferred, to avoid selection bias and confounding factors.23 A power analysis is recommended to determine the adequacy of sample sizes, to avoid type II statistical errors.24 A rigorous 0.01 alpha value reduces the risk of type I errors.
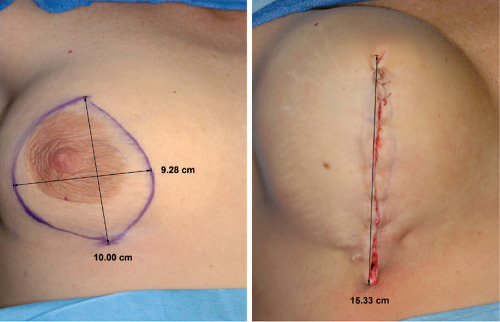 Fig. 3. Intraoperative photographs of vertical augmentation/mastopexy. (Left) Before and (right) after elliptical skin resection. With side-to-side tissue approximation, the vertical length increases from 10.00 cm to 15.33 cm. If the vertical and horizontal dimensions of the resection are the same (i.e., roughly a circle), an increase in vertical length to π/2 (+57 percent) is expected. |
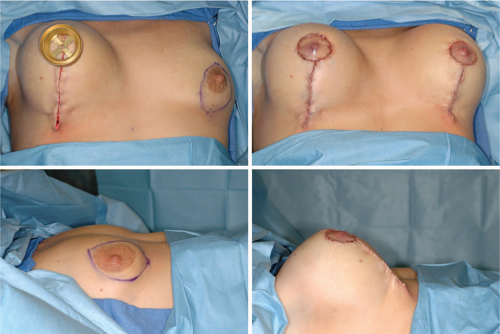 Fig. 4. Intraoperative photographs of augmentation/mastopexy. (Above, left) After the superior dog-ear is oversewn, a 39-mm areola marking ring is used to mark the circular resection at the new site for the nipple-areola. (Above, right) The left augmentation/mastopexy is complete. (Below, left) Preoperative and (below, right) immediate postoperative views show the increased breast projection provided by the implant and the position of the nipple-areola, slightly below the level of maximum breast projection. The implant takes up much of the slack in the lower pole, minimizing the need for skin gathering and keeping the vertical incision from extending onto the abdominal skin. |
All-Seasons Mammaplasty
A growing number of plastic surgeons have adopted the vertical technique as their procedure of choice for mastopexy and reduction.25 At a recent meeting of the American Society of Plastic Surgeons, 47 percent of audience members responding to a poll reported using the vertical technique for their augmentation/mastopexies, versus 38 percent who still favored the inverted-T design, and 10 percent who preferred a periareolar resection.26 Persistent ptosis is a frequent problem after a periareolar mastopexy.5,16,27 The shape deficiencies of the inverted-T, inferior pedicle technique have been recognized for decades.27 Although the idea of an “all-seasons” mammaplasty has been dismissed in the past,28 an increasing number of plastic surgeons use the vertical technique exclusively,7,29–34 including the author. Its versatility is demonstrated in Figures 5 through 8, which depict not typical cases but more challenging ones (i.e., very large breasts, tuberous breasts, asymmetrical breasts, and secondary surgery).
Commonly, a periareolar mastopexy is recommended for patients with minimal degrees of ptosis, a vertical technique for more moderate cases, and the inverted-T technique for cases of moderate or severe ptosis.35,36
However, a vertical technique is particularly advantageous in large resections because a long pedicle is unnecessary,7 improving safety for the nipple and areola,31–34 and avoiding the need for nipple grafting. The anatomical and geometrical advantages of the vertical technique27 do not change with breast size (Fig. 5). Elegant in its simplicity, this technique may be used for all cosmetic mammaplasties, with the only variables being implant size (if used) and the resection weight, making it truly an all-seasons mastopexy. Even small, ptotic breasts and
tuberous breasts, traditionally considered the domain of the periareolar technique,15 respond well to vertical mastopexy (Fig. 6).
However, a vertical technique is particularly advantageous in large resections because a long pedicle is unnecessary,7 improving safety for the nipple and areola,31–34 and avoiding the need for nipple grafting. The anatomical and geometrical advantages of the vertical technique27 do not change with breast size (Fig. 5). Elegant in its simplicity, this technique may be used for all cosmetic mammaplasties, with the only variables being implant size (if used) and the resection weight, making it truly an all-seasons mastopexy. Even small, ptotic breasts and
tuberous breasts, traditionally considered the domain of the periareolar technique,15 respond well to vertical mastopexy (Fig. 6).
Table 2. Complications* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients
One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients
 Breast Deformities and Mastopexy
Breast Deformities and Mastopexy
 Dermal Suspension and Parenchymal Reshaping Mastopexy after Massive Weight Loss: Statistical Analysis with Concomitant Procedures from a Prospective Registry
Dermal Suspension and Parenchymal Reshaping Mastopexy after Massive Weight Loss: Statistical Analysis with Concomitant Procedures from a Prospective Registry
 Mastopexy
Mastopexy
 Obstructive Sleep Apnea: Evaluation and Treatment
Obstructive Sleep Apnea: Evaluation and Treatment
 Posterior Tibial Artery Perforator Flap
Posterior Tibial Artery Perforator Flap
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


