Breast Deformities and Mastopexy
Maurice Y. Nahabedian, M.D.
Washington, D.C.
From the Department of Plastic Surgery, Georgetown University Hospital.
Received for publication April 27, 2010; accepted September 14, 2010.
Copyright ©2011 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31820a7fa7
Disclosure: The author has no financial interest to declare in relation to the content of this article.
Related Video content is available for this article. The videos can be found under the “Related Videos” section of the full-text article, or, for Ovid users, using the URL citations printed in the article.
Learning Objections: After reviewing this article, the participant should be able to: 1. Appreciate the diversity of approaches for the correction of breast deformities and mastopexy. 2. Review the salient literature. 3. Understand patient selection criteria and indications.
Summary: Breast deformities and mastopexy continue to challenge plastic surgeons. Deformities such as Poland syndrome, tuberous breast, gynecomastia, and other congenital conditions are uncommon; therefore, management experience is often limited. Various techniques have been described, with no general consensus regarding optimal management. Mastopexy has become more common and is performed both with and without augmentation mam-maplasty. However, a variety of techniques are available, and a thorough understanding of the indications, patient selection criteria, and techniques is important to optimize outcomes. This article will review these and other conditions to provide a better understanding of the current available data and evidence for these operations. (Plast. Reconstr. Surg. 127: 91e, 2011.)
When considering all types of breast surgery, the category of breast deformity is perhaps the least prevalent and in some ways the most challenging. The conditions that make up this category include tuberous breast, Poland syndrome, and gynecomastia, as well as congenital and developmental breast asymmetries. Many of these anomalies have embryologic origins and manifest during puberty.1 These conditions have all been described in variable detail both in textbooks and in the scientific literature; however, because these conditions are less common, associated with variable degrees of complexity, and are sometimes difficult to treat, there is a lack of consensus on optimal management. This section will focus on and emphasize the various evaluation and management strategies that have been described.
A separate topic in this category is mastopexy. Although mastopexy is used to correct an overly ptotic breast and may be unrelated to the correction of a classic breast deformity, the principles and concepts of repair are best suited for this section, as there is some degree of overlap with the correction of breast deformities. The subcategory of augmentation mastopexy will also be covered in this section.
Tuberous Breast Deformity
There are several features of the tuberous breast that are important to identify before management. These include a constricted base, contraction of the skin envelope, relative micromastia, enlarged diameter of the nipple-areola complex, and herniation of breast parenchyma through the nipple-areola complex2 (Fig. 1). Although the exact etiology has not been elucidated, it is generally accepted that this disorder has an embryologic origin.3 Most reports have speculated that the superficial investing fascia of the breast is abnormal and constricted at the base of the breast. This constriction at the base and deficiency at the are-ola is responsible for the reduced base diameter and areolar herniation.3 A competing theory states that there is no constrictive band at the base of the breast and that the only abnormality is a deficiency of areolar support, giving rise to the herniation.4
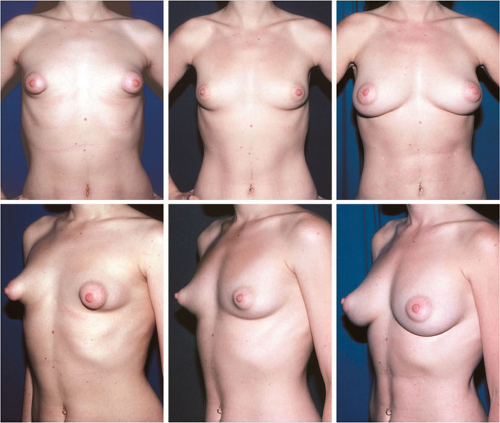 Fig. 1. Preoperative and postoperative views of a patient with tuberous breast deformity. (Left) The nipple-areola complex is enlarged with a herniated appearance, and the base diameter of the breast is constricted. In this case, the breast was corrected with autologous fat grafting. (Center) Results following first session of fat grafting. (Right) Results following second session of fat grafting. (Reprinted from Coleman SR, Saboeiro AP. Fat grafting to the breast revisited: Safety and efficacy. Plast Reconstr Surg. 2007;119: 775–785.) |
Several surgical approaches have been described to correct the tuberous breast deformity.2–11 Rees and Aston first described the correction of the tuberous breast in 1976 and advocated expanding the base diameter of the breast with radial scoring.2 Dinner and Dowden believed that the constriction was the result of a cutaneous band and advocated a skin incision.5 Ribeiro et al. identified a constrictive ring and advocated dividing it horizontally.6,7 Mandrekas et al. have performed a similar operation to Ribeiro, except that the constrictive band was divided vertically3 (Fig. 2). Pa-cifico and Kang have described an alternative approach in which areola reduction, subdermal undermining, and subglandular implant placement are used.4 Their belief is that the deformity is due solely to an areolar abnormality and not to a constrictive band at the base. Coleman and Saboeiro have reported on the benefits of lipoaug-mentation by injecting autologous fat into the subcutaneous tissues and pectoral muscle.8 In a single patient, two sessions were required, with injection volumes of 370 cc on the right and 380 cc on the left. This was followed 4 years later with 300 cc on the left and 340 cc on the right (Fig. 1).
It is generally believed that correction of tuberous breast deformity requires attention to several salient points. The approach that is advocated
by most is to outline a circumareolar pattern around the perimeter of the desired nipple-areola complex. A donut-type mastopexy pattern is outlined. After skin excision, the circumference of the surrounding tissues is undermined; however, the inferior subcutaneous plane is undermined to the level of the inframammary fold and chest wall. The inferior breast parenchyma is undermined and ultimately divided centrally or scored to disrupt or divide the fibrous constrictive ring. The lower pole of the breast can be contoured by utilizing an inferiorly based flap or the medial and lateral lower breast pillars to provide the paren-chymal tissue needed to reconstruct the lower pole. A prosthetic device is usually inserted in the prepectoral plane and covered entirely by parenchymal tissue. In rare circumstances, a prosthetic device may not be necessary if there is enough parenchymal tissue to create a flap of tissue to enhance projection and contour.
by most is to outline a circumareolar pattern around the perimeter of the desired nipple-areola complex. A donut-type mastopexy pattern is outlined. After skin excision, the circumference of the surrounding tissues is undermined; however, the inferior subcutaneous plane is undermined to the level of the inframammary fold and chest wall. The inferior breast parenchyma is undermined and ultimately divided centrally or scored to disrupt or divide the fibrous constrictive ring. The lower pole of the breast can be contoured by utilizing an inferiorly based flap or the medial and lateral lower breast pillars to provide the paren-chymal tissue needed to reconstruct the lower pole. A prosthetic device is usually inserted in the prepectoral plane and covered entirely by parenchymal tissue. In rare circumstances, a prosthetic device may not be necessary if there is enough parenchymal tissue to create a flap of tissue to enhance projection and contour.
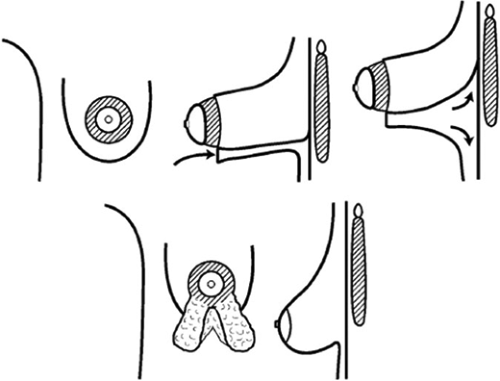 Fig. 2. The Mandrekas technique is illustrated. (Above, left) A periareolar approach is advocated. (Above, center) The dissection proceeds in the subcutaneous plane to the pectoral fascia. (Above, right) The dissection continues to the desired inframammary fold. (Below, left) The inferior pole of the breast is exteriorized, and the constrictive band is divided vertically. (Below, right) Finally, the areola is reduced, and the breast is recontoured. (Reprinted from Mandrekas AD, Zambacos GJ, Anastasopoulos A, etal. Aesthetic reconstruction of the tuberous breast deformity. Plast Reconstr Surg. 2003; 112:1099–1108.) |
Complications include recurrence, loss of sensation, asymmetry, scar, delayed healing, and implant-related complications. Mandrekas et al., in their review of 11 patients, and Pacifico and Kang, in their review of eight patients, reported no complications.3,4 Reported outcomes have ranged from good to excellent. Mandrekas et al. reported 100 percent patient satisfaction and 100 percent surgeon satisfaction.3 Pacifico and Kang reported outcomes on eight patients and 13 breasts following areola reduction and subglandular augmentation.4 An independent panel graded the outcomes as excellent in 75 percent and good in 25 percent; however, all patients reported that they were very satisfied with the outcome.
Mastopexy
See Video 1, in which Dr. Elizabeth Hall-Findlay shows the marking of the breast for mastopexy and reduction, available in the “Related Videos” section of the full-text article on PRSJournal.com. Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A309.
See Video 2, in which Dr. Hall-Findlay shows the dissection for mastopexy, including inferior flap rearrangement, the superior pedicle, and vertical skin resection, available in the “Related Videos” section of the full-text article on PRSJournal.com.
Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A310.
Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A310.
 Video 1. Video 1, in which Dr. Elizabeth Hall-Findlay shows the marking of the breast for mastopexy and reduction, is available in the “Related Videos” section of the full-text article on PRSJournal.com. Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A309. Presented with permission from Elizabeth Hall-Find-lay, M.D., and Tracker Productions, Banff, Alberta, Canada. |
 Video 2. Video 2, in which Dr. Hall-Findlay shows the dissection for mastopexy, including inferior flap rearrangement, the superior pedicle, and vertical skin resection, is available in the “Related Videos” section of the full-text article on PRSJournal.com. Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A310. Presented with permission from Elizabeth Hall-Findlay, M.D., and Tracker Productions, Banff, Alberta, Canada. |
See Video 3, in which Dr. Hall-Findlay shows the skin closure and liposuction for mastopexy, available in the “Related Videos” section of the full-text article on PRSJournal.com. Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A311.
 Video 3. Video 3, in which Dr. Hall-Findlay shows the skin closure and liposuction for mastopexy, is available in the “Related Videos” section of the full-text article on PRSJournal.com. Video for Ovid users is available at http://links.lww.com.easyaccess1.lib.cuhk.edu.hk/PRS/A311. Presented with permission from Elizabeth Hall-Findlay, M.D., and Tracker Productions, Banff, Alberta, Canada. |
Mastopexy is indicated in women who desire an improvement in breast contour without a volume change. Traditionally, mastopexy has been performed using primarily skin excision techniques; however, since the mid-1990s, there has been an emphasis on internal shaping of the pa-renchymal tissue as well. The classic skin excision patterns for mastopexy have included crescent, periareolar, circumvertical, and inverted-T designs. Internal shaping can be performed using various supportive materials or parenchymal pillars. This section will review the indications as well as various methods and techniques described.
The type of mastopexy performed will depend on the degree of breast ptosis. Breast ptosis is graded using Regnault’s classification (Table 1). An excellent review of the standard mastopexy techniques was compiled by Rohrich et al.12 A crescent mastopexy can be considered when the degree of nipple-areola complex elevation does not exceed 1 cm. A periareolar mastopexy can be
considered when the distance of nipple-areola complex elevation ranges from 1 to 2 cm, which would be classified as a Regnault I or II. After the skin excision, the outer perimeter of the dermis is scored, and the subcutaneous plane is undermined circumferentially to allow for adequate re-draping of the skin envelope over the parenchyma. The periareolar mastopexy can be performed as a “donut” and in an eccentric pattern (Fig. 3). A circumvertical mastopexy will lift the base of the breast as well as reposition the nipple-areola complex and is usually used for a Regnault II (Fig. 4). The inverted-T technique is useful for the moderate to severely ptotic breast classified as a Regnault II or III (Fig. 5). The horizontal incision will reduce the distance from the nipple-areola complex to the inframammary fold, while the vertical incision will reduce the base diameter. The L-shaped mastopexy will eliminate the medial portion of the inverted-T incision and is indicated for women with grade I to II breast ptosis (Fig. 6).
considered when the distance of nipple-areola complex elevation ranges from 1 to 2 cm, which would be classified as a Regnault I or II. After the skin excision, the outer perimeter of the dermis is scored, and the subcutaneous plane is undermined circumferentially to allow for adequate re-draping of the skin envelope over the parenchyma. The periareolar mastopexy can be performed as a “donut” and in an eccentric pattern (Fig. 3). A circumvertical mastopexy will lift the base of the breast as well as reposition the nipple-areola complex and is usually used for a Regnault II (Fig. 4). The inverted-T technique is useful for the moderate to severely ptotic breast classified as a Regnault II or III (Fig. 5). The horizontal incision will reduce the distance from the nipple-areola complex to the inframammary fold, while the vertical incision will reduce the base diameter. The L-shaped mastopexy will eliminate the medial portion of the inverted-T incision and is indicated for women with grade I to II breast ptosis (Fig. 6).
Table 1. Regnault’s Classification of Breast Ptosis Based on the Position of the Nipple-Areola Complex Relative to the Inframammary Fold | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
Recent innovations have expanded the options for traditional mastopexy. Traditional approaches for mastopexy have emphasized modification of the skin envelope only with minimal parenchymal manipulation. Goes was the first to demonstrate that skin-only excisions were not sufficient to maintain long-term benefits.13,14 He emphasized using a periareolar dermal flap in conjunction with mixed mesh to support the glandular structures. As these concepts have evolved, the benefits of internal parenchymal reshaping have been demonstrated. Foustanos and Zavrides have described the double-flap technique.15 The mastopexy outline utilizes the inverted-T pattern. An inferiorly based parenchymal flap based on chest wall perforating vessels is created, as well as a medial and lateral pillar. The upper breast is partially undermined off the pectoral fascia. The inferior parenchymal flap is sutured to the pectoral fascia, and the medial and lateral pillars are sutured together. Boehm et al. prefer the same operation, except that it is performed through a vertical incision.16 Ritz et al. have described the fascial suspension mastopexy in which a vertical or inverted-T pattern is delineated.17 The technique is similar to the Foustanos and Zavrides technique, except that the inferior parenchymal pedicle is tunneled under a 3 × 5-cm band of pectoralis fascia. The medial and lateral pillars are approximated. Graf and Biggs have popularized the pectoral loop technique in which the inferior paren-chymal flap is passed through a loop of pectoral muscle to maintain the position of the flap.18 This operation can be performed though various incisional patterns that include J, inverted-T, vertical, and horizontal patterns. The use of an interlocking Gore-Tex suture to maintain the diameter of the nipple-areola complex can be considered.
Related posts:
 One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients
One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients
 Dermal Suspension and Parenchymal Reshaping Mastopexy after Massive Weight Loss: Statistical Analysis with Concomitant Procedures from a Prospective Registry
Dermal Suspension and Parenchymal Reshaping Mastopexy after Massive Weight Loss: Statistical Analysis with Concomitant Procedures from a Prospective Registry
 Prospective Comparative Clinical Evaluation of 784 Consecutive Cases of Breast Augmentation and Vertical Mammaplasty, Performed Individually and in Combination
Prospective Comparative Clinical Evaluation of 784 Consecutive Cases of Breast Augmentation and Vertical Mammaplasty, Performed Individually and in Combination
 Mastopexy
Mastopexy
 In Pursuit of Perfection: The Art of Facial Restoration
In Pursuit of Perfection: The Art of Facial Restoration
 Correction of Secondary Bilateral Cleft Lip and Nose Deformities
Correction of Secondary Bilateral Cleft Lip and Nose Deformities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


