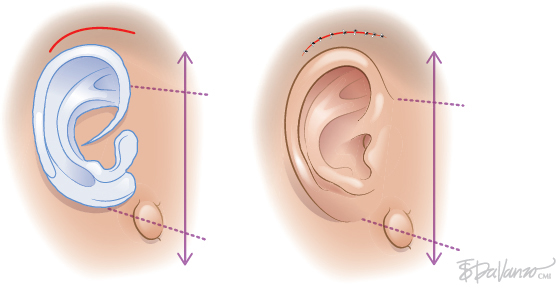
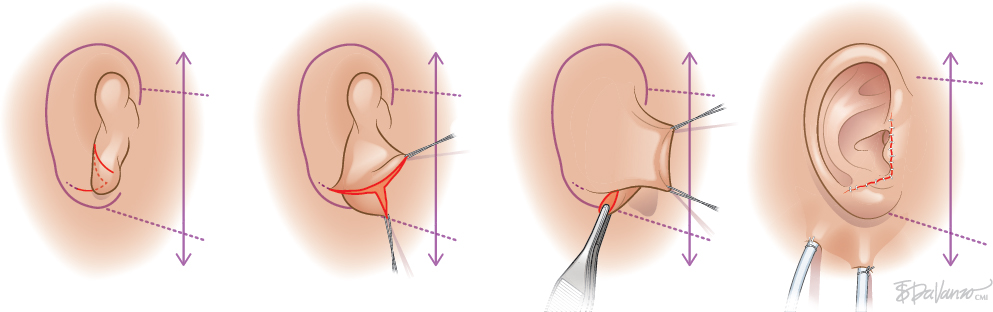
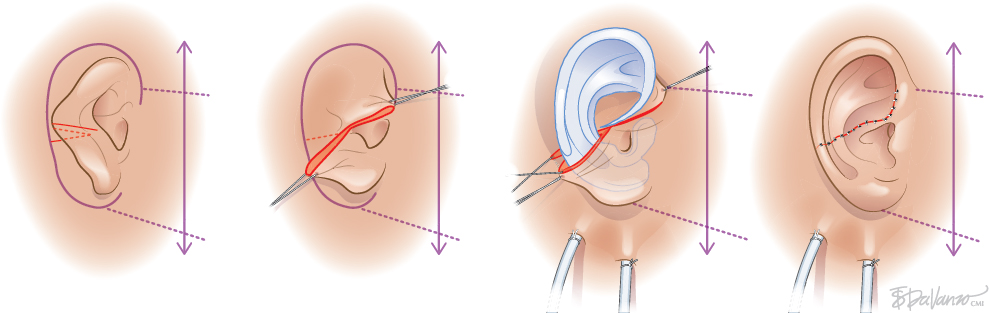
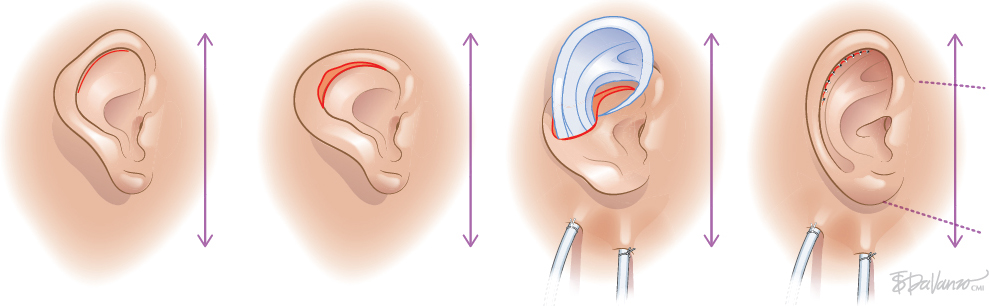
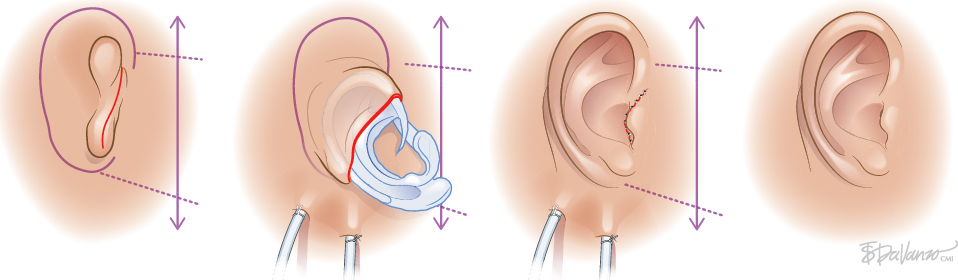
CHAPTER 1 To reconstruct total or subtotal defects of the ear, whatever the circumstances, is to reproduce the missing contours using a support. The result of any reconstruction will be directly dependent on the quality of the framework reproducing these contours and the quality of the skin covering it. The skin will adapt to the underlying support, reproducing the harmonious curves and shapes of the ear, which may then be elevated by creating a sulcus. Our goal should be that our patients no longer hide their ears. Fig. 1-1 This 6-year-old boy had bilateral microtia. He used to hide his ear anomalies with his long hair. When he returned 1 year after having both ears reconstructed, he was no longer hiding them. Ear Reconstruction Principles: The 10 Commandments 1. When analyzing an auricular defect, the first step is always to make a model of the normal ear and place it in the ideal position on the affected side. 2. The auricular skin is the best for reconstructing an ear; fascial flaps should only be used when auricular skin is not available. 3. Skin-only flaps without support cannot reproduce the complex contours of an ear, and the best support currently is autologous cartilage. 4. Conchal cartilage can only be used when the size of the defect is no more than a quarter of the ear and involves no more than two planes; otherwise, costal cartilage must be used. 5. When harvesting conchal cartilage, the entire floor of the conchal bowl must be harvested leaving intact the root of the helix, to prevent a visible ear deformity. 6. Once the three-dimensional contours of the ear are understood and after training, sculpting should become the routine part of the surgery and management of the skin the difficult part. 7. Everything will be visible under the very thin auricular skin; therefore no compromise with the shape of the framework is acceptable. 8. In choosing a skin approach, surgeons should always consider the existing scars and the position of the remnants. 9. Never elevate an ear whose contours are unsatisfactory after the first stage. 10. For consistent results, surgeons must perform ear reconstruction procedures frequently. The first stage of ear reconstruction consists of harvesting the cartilage, sculpting it, and placing it under the skin. The principles are similar for microtia and trauma. Particular problems encountered in different situations will be discussed in later chapters. The second stage is the reconstruction of a retroauricular sulcus, which is discussed in Chapter 3. Where to make the incision is one of the most frequently asked questions in auricular reconstruction. Particularly in patients with microtia, who have such a vast array of congenital malformations, this decision can vex even the most experienced plastic surgeons. Historically, many different approaches have been used for managing the skin envelope, and numerous techniques have been described to improve its vascularity. In our experience, regardless of the cause, size, shape, or position of the ear deformity, only three types of skin approach should be considered (type 1, type 2, and type 3). The only decision to make is to select the most appropriate technique to provide sufficient coverage to the sculpted framework safely. Once these three categories of skin approach are well understood, it will become evident that our surgical classification can be used to determine an optimal surgical approach in every case. COMMANDMENT 6: Once the three-dimensional contours of the ear are understood and after training, sculpting should become the routine part of the surgery and management of the skin the difficult part. Our classification system is a surgical classification; that is, the stratification of different skin incisions will dictate different surgical approaches. We will describe the three types of possible skin approaches and how to select the most appropriate one in different circumstances. This classification system was designed to assist with incision planning for microtia patients but is also highly useful for treating patients requiring posttraumatic ear reconstruction (see Chapters 4 and 6). Fig. 1-2 The type 1 incision involves the exchange of two flaps, one of which includes the lobule and the other the mastoid skin. This approach allows transposition of the lobule from a vertical orientation into its correct position. We no longer use this approach. It is included in the classification, because it is still routinely used by some surgeons. We think the Z-plasty technique is inferior to other skin approaches, because only the anterior surface of the lobule is transposed. As a result, the entire base, including the lobule, must be elevated during the second stage. It should not be used when the implantation of the lobule is not in the ideal position, which is frequent. It is almost always preferable to perform a type 2 or type 3b approach when a type 1 approach might be possible. Fig. 1-3 The type 2 skin approach involves a transfixion incision with a backcut to allow adhesion of part of the remnants to the retroauricular skin. This is our routine skin approach when tissue is sufficient for placement in the correct position. This technique preserves both the anterior and posterior surfaces of the lobule. The position of the transfixion incision and the backcut are evaluated by pulling the remnant posteriorly until it reaches the ideal position. Landmarks from the normal ear are used to establish the ideal position on the side with the defect. Type 3 is a skin-only incision used to create the auricular skin pocket. This type has two subtypes: type 3a, which is used when the skin pocket is large enough for single-stage reconstruction, and type 3b, which is used when the skin pocket is not large enough for this purpose, and a two-stage reconstruction is required. Fig. 1-4 The type 3a skin approach is relatively rare but very useful when the local conditions are suitable. The requirement for performing a type 3a skin approach is that the ear is close to normal size (enough skin), but the fibrocartilage is deformed. Care is required when choosing this skin approach, because if it is attempted when skin laxity is inadequate, then skin necrosis and framework exposure may result. The skin incision should be placed to facilitate dissection of the fibrocartilage remnant. After the fibrocartilage is removed, the framework is inserted into the pocket, and the retroauricular sulcus is maintained. Reconstruction is completed in only one stage. Fig. 1-5 The type 3b skin approach is routinely used to create a skin incision facilitating dissection of a skin pocket of uniform thickness. A second stage will be required to create the retroauricular sulcus. The skin-only approach does not dictate the precise location of the incision. Usually, this is placed where auricular skin pits must be excised or to facilitate access to the remnant fibrocartilage.
Principles of Two-Stage
Autologous Ear Reconstruction

SKIN APPROACH CLASSIFICATION
Type 1: Z-plasty
Type 2: Transfixion Incision With Adhesion
Type 3: Skin-only Incision
Type 3a: Skin-only Incision (One Stage)
Type 3b: Skin-only Incision (Two Stages)
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine