Key Words
cleft lip, unilateral cleft lip repair, rotation advancement repair, technique, primary cleft rhinoplasty
Synopsis
Caring for the unilateral cleft lip patient extends far beyond primary cleft lip repair. The complex needs of the cleft patient and family evolve as the child ages; therefore, a longitudinal multidisciplinary team approach is obligatory for proper care. In this chapter we present our preferred technique for repair of the unilateral complete and incomplete cleft lip deformity.
Clinical Problem
Unilateral cleft lip is the congenital separation of the upper lip that, to varying degrees, also affects the nose and underlying alveolus. Cleft lip with or without cleft palate is the most common congenital facial defect, affecting 1 : 690 U.S.-born children. Males and people of Asian and Native American descent are more commonly affected. Unilateral cleft lip can be classified as:
- •
microform (i.e., forme fruste ): discontinuity of the vermilion cutaneous junction with a less than 3-mm difference in the subnasale to Cupid’s bow peak distance between sides, variable deficiency of vermilion medial to cleft, variable muscular depression along the philtral line, subtle nasal asymmetry, and variable alveolar defect.
- •
minor form: greater than 3-mm difference in the subnasale to Cupid’s bow peak distance between sides, discontinuity of the orbicularis oris with more prominent depression of the philtral line, increased nasal asymmetry with posteroinferior displacement of the cleft side piriform aperture, and alveolar cleft.
- •
incomplete: full-thickness separation of the upper lip with a continuous, though depressed, nasal sill and floor ( Fig. 3.1.1 ).

FIG. 3.1.1
A 3-month-old male with a right-sided incomplete cleft lip. (A) There is marked distortion and flattening of the right alar base. “Simonart’s band” in the cleft nasal sill is composed of skin but is lacking muscle. (B) Lesser segment maxillary retroposition, outward greater segment alveolar rotation, and nasal deformities are more apparent in the worm’s-eye view.
- •
complete: full-thickness separation of the lip extending into the nasal cavity and discontinuity of the alveolus ( Fig. 3.1.2 ).

FIG. 3.1.2
A 3-month-old female with a left-sided complete cleft lip. (A) Nasal distortion is more severe than in the infant in Fig. 3.1.1 , and there is greater discrepancy in lip vertical height. (B) Retroposition of the lesser maxillary segment and outward rotation of the greater alveolar segment are more severe and apparent in the worm’s-eye view.
This chapter focuses on surgical repair of the incomplete and complete unilateral cleft lip deformity.
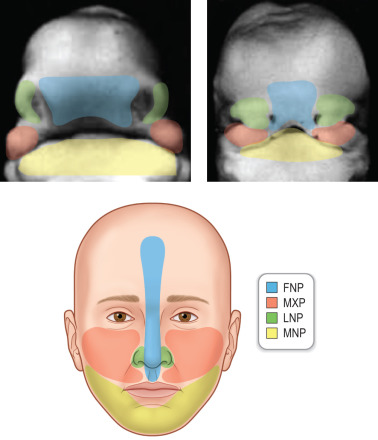
Unilateral cleft lip results from failure, or partial fusion, of the frontonasal and maxillary prominence between 4 and 7 weeks of gestation ( Fig. 3.1.3 ). Several teratogens including phenytoin and maternal smoking have been associated. Van der Woude syndrome is the most commonly associated syndrome; however, incompletely understood non-syndromic genetic associations are far more common.
Pre-Operative Management
Evaluation and Timing of Surgery
A multidisciplinary cleft team including a plastic surgeon, otolaryngologist, orthodontist, speech pathologist, audiologist, social worker, and photographer evaluates the patient and family. Programs in developing countries should strive to use this team approach. A thorough history and physical examination is performed. Clinical findings help determine whether there is a need for pre-operative nasoalveolar molding (NAM). Surgical repair is typically performed at 3 months of age; however, this may be delayed as a result of pending completion of NAM or need for medical optimization in patients with comorbid conditions. The “rule of 10’s” is a frequently quoted minimum safety cutoff of age (10 weeks), weight (10 kilograms), hemoglobin (greater than 10) before undergoing lip repair. This is not substantiated by recent evidence, and repair may proceed despite failure to meet all criteria if a full preoperative evaluation has been performed.
Relevant Anatomy
Unilateral incomplete and complete cleft lip anatomical derangements are complex ( Fig. 3.1.1 and 3.1.2 ) and involve the skin, muscle, nasal cartilage, and bony maxilla. The relevant anatomy includes the following:
- •
There is deficient vertical height of the cleft side lip—this involves both the external skin and intraoral mucosa.
- •
The orbicularis oris is in discontinuity, with abnormal insertion of the greater (i.e., medial) segment pars peripheralis into the anterior nasal spine and abnormal insertion of the columellar base and lesser (i.e., lateral) segment into the alar base and piriform aperture periosteum.
- •
The lesser alveolar segment is retropositioned, and the greater alveolar segment is anteriorly rotated. Extrinsic forces of the tongue and cheek and abnormal insertions of the orbicularis oris likely contribute to this.
- •
The cleft-side piriform aperture is posteroinferiorly displaced with decreased projection of the midface on the cleft side.
- •
The columella is asymmetrically shortened (cleft side shorter than non-cleft side) with deviation of the columellar base toward the non-cleft side.
- •
The nasal tip is rotated toward the cleft side.
- •
The caudal septum is displaced out of the vomerine groove into the non-cleft side.
- •
The septum is convex on the cleft side, projecting into the cleft nasal vestibule.
- •
The cleft side lower lateral cartilage has a shortened medial crus resulting in retroposition of the cleft-side nostril dome, an elongated and flattened lateral crus resulting in widening and posterior displacement of the cleft nostril sill, and an obtuse angle of the cleft side nostril dome.
- •
There is deficient cleft nostril vestibular lining.
- •
There is vestibular webbing of the lateral cleft nostril.
- •
Finally, there is an ill-defined cleft-side alar-facial groove.
Nasoalveolar Molding
NAM as described by Grayson and Garfinkle and Grayson et al. is used in patients with a wide complete nasal cleft or significant nasal deformity. NAM helps expand the significantly shortened columella and nasal vestibular tissues. NAM also improves convexity of the cleft-side lower lateral cartilage, approximates the alveolar segments, and improves the outward rotation and posterolateral rotation of the greater and lesser alveolar segments, respectively. This greatly facilitates primary cleft lip repair, reduces tension at the incision line, and improves the long-term cosmetic appearance of the primary cleft rhinoplasty. NAM is started within the first 2 weeks of birth and takes 2 to 3 months to complete. Of note, NAM requires dedicated and compliant parents because orthodontic adjustments are needed every 1 to 2 weeks. Although this standard of care is ideal, meeting it may be challenging in resource-limited settings in developing countries.
Pre-Operative Testing
A pre-operative complete blood count is obtained. Otherwise, no further imaging or tests are required unless the infant has other concurrent abnormalities.
Anesthetic Considerations
There are few intraoperative anesthetic concerns; however, every attempt is made to minimize the number of procedures. Evidence suggests that there are dose-dependent neurological sequelae related to the exposure of infants less than 1 year of age to general anesthesia. Syndromic patients are more likely to have airway anomalies that may delay repair.
Supplies Needed
- •
Fine-tip marking pen
- •
Methylene blue and 25G needle for tattooing
- •
15c blade
- •
15 blade
- •
Webster needle holder
- •
Medium-length delicate needle holder
- •
Adson forceps with teeth
- •
Adson-Brown forceps
- •
Castroviejo forceps with teeth
- •
Curved Iris scissors
- •
Curved black-handled tenotomy scissors
- •
Mosquito hemostats ×2
- •
Freer periosteal elevator
- •
Single-hook retractors ×2
- •
Ragnell retractor
- •
Non-penetrating towel clamp
- •
Bipolar cautery
- •
10-French Frasier tip suction
- •
Porex nasal stent and sizers (Stryker Corp., Kalamazoo, MI)
- •
6-0 black nylon suture
- •
4-0 undyed vicryl suture (Ethicon Inc., Somerville, NJ)
- •
5-0 undyed vicryl suture
- •
5-0 PDS (polydioxanone) suture (Ethicon Inc., Somerville, NJ)
- •
4-0 Prolene suture (Ethicon Inc., Somerville, NJ)
Surgery
Positioning and Surgical Site Preparation
- •
Supine with gentle neck extension using a gel shoulder roll.
- •
Foam doughnut to secure head position.
- •
Warm air circulator to prevent hypothermia.
- •
Oral cavity is prepped with 10% betadine using an oral swab.
- •
Entire face is prepped with 5% betadine.
- •
Sterile towel head drape placed, secured with non-penetrating clamp.
- •
Split drape placed.
- •
Eyes are irrigated with balanced salt solution, and lids are closed with Steri-Strips to prevent corneal irritation.
Anesthesia
- •
General endotracheal anesthesia.
- •
Critical that the endotracheal tube is midline and directed directly inferior to prevent upper lip distortion. Extension tubing is placed to prevent surgical field impingement.
Approach
A myriad of techniques exist to repair the unilateral cleft lip deformity, each with its individual advantages and disadvantages. Here we present our preferred method of repair, which is similar to the modification of the extended Mohler repair by Cutting and Dayan with several key differences:
- 1.
The back cut is made at or just below the base of the columella, not onto the columella. The back cut is initially made three-fourths of the way across and can be extended up to, but not beyond, the non-cleft philtral column if greater lip lengthening is necessary.
- 2.
A triangular skin flap from the lateral lip just above the white roll is preserved. This is inset into a back cut just above the white roll of the medial lip. It is our experience that this extra tissue is often needed to adequately lengthen the lip and to help prevent secondary scar contracture.
Step-by-Step Technique
Markings ( Fig. 3.1.4 , Fig. 3.1.5 , and ):
- 1.
The nadir of Cupid’s bow (point 1) and the peak of the non-cleft bow (point 2) are marked at the white roll. The distance between these points is transposed with a caliper to mark the Cupid’s bow peak on the cleft side (point 3).
- 2.
A point is marked on the cephalad non-cleft philtral column at or just below the columellar base (point 4). Using the same methodology, a point is marked on the cleft side (point 5).
- 3.
The non-cleft philtral column is marked, point 2–4.
- 4.
The cleft side philtral column is marked, point 3–5.
- 5.
The back cut is drawn as a line three-fourths of the way along point 5 to point 4. This back cut can later be extended up to, but not beyond, the non-cleft philtral column should greater lip lengthening be needed.
- 6.
The alar base is marked on the non-cleft (point 6) and cleft nostril (point 7). Although this point is relatively subjective, great care must be taken to mirror this on each side.
- 7.
The columellar base is marked on the non-cleft (point 8) and cleft (point 9) nostril.
- 8.
A caliper is used to measure the non-cleft lip height (point 2–6).
- 9.
The non-cleft lip height (point 2–6) is transposed to the corresponding point on the lateral lip white roll (point 3′) to establish the cleft side lip height (point 3′–7). Of note, the wider the cleft—i.e., the shorter the height of the lateral lip element—the more lateral point 3′ will be to Noordhoff’s point. This concept is critical. Establishing correct lip height trumps shorter horizontal lip length of the lateral element; any discrepancy in the former will be strikingly apparent, resulting in poor cosmetic appearance.
- 10.
The width of the non-cleft nostril sill (point 6–8) and cleft nostril sill (point 7–9) are measured. Excess cleft nostril sill width (point 10–10′) is marked. Therefore [7–10′] + [10–9] = [6–8], so that the final width of both nostril sills are equal.
- a.
Incomplete cleft: tissue between 10–10′ is excised; it is critical that this area corresponds to the area of “least fullness” of the cleft nostril sill. Furthermore, one must be mindful not to mark this area too medially because this will narrow the C-flap.
OR
- b.
Complete cleft: point 10 and 10′ mark the anterosuperior border of the M- and L-flap, respectively, which are used for mucosal nasal floor lining. Furthermore, the L-flap base is marked intranasally with the cephalad vestibular incision marked as a lateral marginal incision and the caudal vestibular incision marked at the border of the lateral nasal wall with the nasal floor.
- a.
- 11.
The cleft nostril hemitransfixion incision is drawn and connected to point 10, thus defining the superolateral aspect of the C-flap.
- 12.
The wet–dry vermilion border is marked on the medial (point 11) and lateral (point 11′) lip element.
- 13.
Two lines are drawn; one connects points 10, 3, and 11, and the other connects points 10′, 3′, and 11′. This defines the area of tissue excision in the incomplete cleft. It is critical that lines 3–11 and 3′–11′ are angled laterally and medially, respectively. This angle will straighten with downward rotation of the lip.
- a.
Incomplete cleft: tissue between lines 10–3–11 and 10′–3′–11′ defines the area of tissue excision
OR
- b.
Complete cleft: lines 10–3–11 and 10′–3′–11′ define the anterior margins of the M- and L-flap, respectively.
- a.
- 14.
A triangular skin flap with a 2-mm base is drawn just above the white roll of the lateral lip element medial to line 3′–10′.
- 15.
A 2-mm back cut is drawn just above the white roll of the medial lip element. This completes the extra oral markings ( Fig. 3.1.6 ).










