Rhinoplasty is inherently a difficult procedure given the complexity of its structure and the functional and aesthetic impact of this anatomy. This report explores some of the remaining questions regarding the use of spreader grafts and autospreader flaps in the management of the middle vault in rhinoplasty, the performance of the open approach versus the endonasal rhinoplasty approach, corrective rhinoplasty in the younger patient, the use of the rib and other cartilage donor sites for grafting in rhinoplasty, and the use of filler materials in rhinoplasty.
Key points
- •
Spreader grafts and other proven methods to manage middle vault deficiencies should be prudently applied in patients at risk of middle vault insufficiency.
- •
The open and endonasal approaches should both be part of the rhinoplasty surgeon’s armamentarium.
- •
Corrective nasal surgery should be performed even in the very young patient to restore form and function.
- •
The costal cartilage donor site should be considered when it presents as the optimal donor site in rhinoplasty.
- •
Fillers can be judiciously used to temporarily correct limited deficiencies in rhinoplasty. Sound principles of application should be followed to limit the risk of complications.
Introduction
Rhinoplasty is among the most frequently performed cosmetic and elective procedures. This phenomenon is documented in the results of various professional societies’ surveys. Along with this frequency, significant advancements have been made in rhinoplasty over the last few decades in the realms of diagnosis, analysis, the development of new surgical technique, and refinements in execution.
Although there are some widely shared and universally recognized aspects of this craft, there are many differences in technique and philosophy regarding rhinoplasty surgery that are reflected in presentations and in print. In this report, several of these current controversies and differences of opinion are examined in an effort to understand and to lend clarity. In many instances, there remains no right or wrong position, and the written opinion expressed on a particular topic is the working opinion of the author based on personal experience and consideration of the viewpoint of other surgeons.
The topics that will be addressed here are the performance of the open approach versus the endonasal rhinoplasty approach, the use of spreader grafts and autospreader flaps in the management of the middle vault in rhinoplasty, corrective rhinoplasty in the younger patient, the use of the rib and other cartilage donor sites for grafting in rhinoplasty, and the use of filler materials in rhinoplasty.
Introduction
Rhinoplasty is among the most frequently performed cosmetic and elective procedures. This phenomenon is documented in the results of various professional societies’ surveys. Along with this frequency, significant advancements have been made in rhinoplasty over the last few decades in the realms of diagnosis, analysis, the development of new surgical technique, and refinements in execution.
Although there are some widely shared and universally recognized aspects of this craft, there are many differences in technique and philosophy regarding rhinoplasty surgery that are reflected in presentations and in print. In this report, several of these current controversies and differences of opinion are examined in an effort to understand and to lend clarity. In many instances, there remains no right or wrong position, and the written opinion expressed on a particular topic is the working opinion of the author based on personal experience and consideration of the viewpoint of other surgeons.
The topics that will be addressed here are the performance of the open approach versus the endonasal rhinoplasty approach, the use of spreader grafts and autospreader flaps in the management of the middle vault in rhinoplasty, corrective rhinoplasty in the younger patient, the use of the rib and other cartilage donor sites for grafting in rhinoplasty, and the use of filler materials in rhinoplasty.
The open approach and the endonasal approach in rhinoplasty
In considering this topic, several questions might be entertained, for instance:
- 1.
Is the endonasal approach “outdated?”
- 2.
Is the open approach “better?”
- 3.
When should one consider doing an endonasal approach? When should one consider doing an open approach?
- 4.
Is the endonasal approach still being taught at an adequate level?
The open rhinoplasty technique has become exceedingly popular. Advantages to this technique include the direct visualization and direct access to structures when executing rhinoplasty maneuvers. Alternatively, others note the disadvantages of the open approach to include the resultant increased swelling of the nose, the transcolumellar scar, possible vascular compromise of the skin, and the unnecessary dissection of much of the nasal anatomy.
Passionate discussions between individuals who use the open approach versus those who prefer the endonasal approach are long past in most professional circles; the validity of each approach has been shown. Surgeons commonly practice in a manner consistent with their early training as modified by their additive experience. As in many similar surgical matters, the surgical approach used by an experienced surgeon is the result of these factors in addition to the influence of the tasks at hand and the complexity of a particular operation.
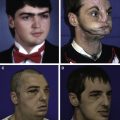
For instance, when the rhinoplasty situation is simple, as when minimal changes are desired, an endonasal approach may be most efficient and appropriate ( Fig. 1 ). In another example in which several challenges exist, but the nose is generally symmetric and straight, an endonasal approach again would be appropriate ( Fig. 2 ). When the task at hand is more complex because the patient’s nose was previously traumatized, is markedly asymmetric, is crooked, or has a congenital deformity, an open approach may be the most appropriate choice ( Fig. 3 ). Through the open approach, the surgeon can usually exert more control over the anatomy as it is altered in rhinoplasty. These observations above are reflected in numerous presentations and articles.
The most pertinent factor in the endonasal versus the open approach dynamic may be the potential negative impact any bias might have on teaching. Optimal teaching may be adversely influenced if the mentor is an ardent advocate for only one of the approaches. Ideally, facial plastic surgeons should be taught both approaches. The student will then have the requisite surgical acumen to decide on whether an open or endonasal approach is to be used by the consideration of the goals and challenges of each particular case, rather than a limiting prejudice of a teacher.
The use of spreader grafts and the management of the middle vault
The nasal sidewall must maintain adequate dimensions to support the airway and the anatomic contour of the nose. This integrity of the middle vault depends on several factors, including the actual dimensions and relationships of the lateral nasal wall anatomic structures, the intrinsic resilience and strength of the structures, and the stabilization of the structures afforded by the overlying nasal musculature. The anatomy and physiology of the nasal valve portion of the middle vault have been recognized for several decades. The negative consequences resulting from the disruption of the relationships between the septum and the upper lateral cartilages are recognized and caution is expressed.
Middle vault collapse manifests itself as airway obstruction, an aesthetic deficiency in which there is a noticeable disruption in a pleasant contour of the patient’s nasal sidewall or both. Patients may present with an inverted V-like deformity that is similar to that seen in saddle nose deformity.
It has been noted in rhinoplasty that there are benefits to recognizing middle vault insufficiency preoperatively and to preventing the iatrogenic creation of a middle vault problem during surgery. Several clinical situations exist in which middle vault insufficiency is commonly seen. The first case is a developmental insufficiency in which a patient has a nasal middle vault that is overly too narrow or has cartilages that are intrinsically too thin or weak to maintain an adequate shape of the middle vault at rest and during inspiration. Another instance is insufficient support of the middle vault after trauma when there has been an avulsion or scarring of the upper lateral cartilage and an iatrogenic collapse of the cartilaginous nasal sidewall. Finally, nasal vault insufficiency may result after nasal surgery in which there has been a disruption of the cartilaginous support of the nasal sidewall or a failure to adequately preserve support in a nose that has anatomic features that might contribute to a tendency to develop middle vault insufficiency.
There is a recognized benefit to stabilizing the middle vault by one of several methods. The management of the middle vault is recommended when there will be a significant surgical manipulation of the nasal dorsum or lateral nasal walls such as with osteotomies or hump reduction. Spreader grafts are found to be a reliable method of addressing both the aesthetic and the functional sequelae of middle vault collapse. Since their introduction, the use of spreader grafts has become exceedingly popular in both aesthetic and functional surgery of the nose. Opinions differ, however, about whether the placement of spreader grafts serve primarily an aesthetic or functional role.
Several points of significant controversy surround the use of spreader grafts. These are unresolved in the literature and are instead more of a topic of individual discussion among surgeons.
Question that remain are:
- 1.
When should spreader grafts be used in primary rhinoplasty?
- 2.
When may it be unnecessary to use spreader grafts in primary rhinoplasty?
- 3.
Does the use of spreader grafts necessitate an open approach?
- 4.
What are reasonable and equivalent alternatives to the use of spreader grafts?
When should spreader grafts be used in primary rhinoplasty? There is a diversity of opinion on this matter. Some experienced surgeons essentially never use them, whereas other experienced surgeons use them in almost every case.
The management of the middle vault of the nose should be considered whenever there is a preexisting deficiency in the integrity of the lateral nasal wall or when it is anticipated that the integrity of the lateral base will be compromised by a surgical maneuver. When a deficiency is detected preoperatively in primary rhinoplasty, spreader grafts are used to correct the deficiency in nasal contour or in the nasal airway ( Fig. 4 ). When it is anticipated that the integrity of the lateral nasal wall will be compromised through the rhinoplasty operation, some management technique should probably be entertained. Typical surgical maneuvers that compromise the integrity of the middle vault include the taking down of a dorsal convexity or the separation of the upper lateral cartridges from the septum as might be performed to straighten a crooked nose. When one takes down a dorsal convexity, there is not only a disruption of the attachments between the central cartilaginous septum and the upper level cartilages but also a reduction in the height of the upper lateral cartridges that form the nasal sidewall ( Fig. 5 ).
The question about when to use or not to use spreader grafts revolves around 2 different axes. The first axis is diagnostic in which one needs the clinical acumen to judge when the middle vault is stable and will remain stable. Clinically, the concept of short nasal bones has been repeatedly mentioned in presentations and in the literature as a characteristic of a patient that the rhinoplasty surgeon should recognize to be at increased risk for middle vault collapse. Alternatively, patients who are judged to have longer nasal bones will hypothetically have more lateral wall support and be less prone to acquire middle vault collapse. These patients, therefore, may not need spreader grafts to stabilize the middle vault. The concept of short versus long nasal bones has been an arbitrary clinical indicator without an established benchmark of what the normal length of the adult nasal bones are. The study by Setabutr and colleagues, resulted in normative data about the length of normal adult nasal bones in cadavers. There remains, however, little objective evidence to further guide the judgment of the surgeon during surgery.
The other axis that this question revolves around is a surgical/anatomic axis. If there are no dorsolateral nasal wall or osteotomy maneuvers performed, the likelihood of needing some form of middle vault management is lessened. If the relationship between the upper lateral cartilages and the septum is not disrupted, then the middle vault should remain stable, and spreader grafts may not be necessary. Thus, the patient who only has tip maneuvers performed during rhinoplasty may not need spreader grafts or other middle vault maneuvers performed. This statement is made with the caveat that there cannot be a preexisting deficiency, and none of the surgical maneuvers will disrupt the natural relationship between the lateral nasal sidewall and the septum. Primary rhinoplasty in which possibly only a minimal amount of tip procedures are to be performed is an example.
Does the use of spreader grafts necessitate an open approach? It is technically easier to place spreader grafts via an open approach. Alternatively, several investigators found that spreader grafts can be predictably performed through an endonasal approach.
What are reasonable alternatives to the use of spreader grafts? Spreader grafts are generally described as being paired cartilage grafts that are approximately 4 mm wide by ≥15 mm long. These grafts are sutured on either side of the dorsal midline septum, and in turn, the bilateral upper lateral cartilages are sutured against the spreader grafts. The entire complex can be sutured together with one pair of horizontal mattress sutures. An alternative method is to first suture the spreader grafts to the upper border of the central septum and then secondarily suture the upper lateral cartilages to the spreader grafts. A reasonable alternative method to the use of spreader grafts seems to be the use of autospreader flaps. The creation and utilization of autospreader flaps requires that there is an excess of upper lateral cartilage to contour and suture to the dorsal central septum. These flaps seem to serve similar purposes as the use of spreader grafts. The major difference, however, is that in the case of the use of autospreader flaps, the middle vault is stabilized by an excess of bilateral upper lateral cartilage that is recontoured and sutured to the septum. The use of autospreader flaps, by definition, requires that there be an excess of upper lateral cartilage remaining, such as after the reduction of a dorsal hump ( Fig. 6 ).