Cleft lip and palate is one of the most common congenital anomalies. For many years, surgeons have been attempting to reduce the severity of the deformity before the surgical repair to achieve a better outcome. The nasoalveolar molding technique uses acrylic nasal stents attached to the vestibular shield of an oral molding plate to mold the nasal alar cartilages into a more normal form and position during the presurgical period. Proponents of nasoalveolar molding claim several benefits, including improved aesthetic outcome, reduced overall costs, and a psychosocial benefit to the family. Research on these outcomes is not conclusive.
Key points
- •
Nasoalveolar molding (NAM) is a form of presurgical infant orthopedics (PSIO) whose goal is to reduce the severity of the cleft deformity and improve surgical outcomes. The data on efficacy and benefit of NAM are mixed.
- •
Those in favor of NAM report improved nasal symmetry and appearance, reduced overall costs, psychosocial benefit to family, and decreased need for early nasal revision.
- •
Those in opposition to NAM argue NAM causes increased caregiver burden, poor patient compliance, increased costs in the short term, relapse of nasal symmetry in the first year, and no conclusive data of improved outcomes.
Introduction
Cleft lip and palate is one of the most common congenital craniofacial disorders. Patients born with a cleft deformity might experience problems with feeding, speech, and hearing, as well psychological stresses and issues with social well-being secondary to their aesthetic deformity. To fully address the needs of the cleft patient, a multidisciplinary team approach is required. Complete care of the cleft patient is a challenging task, with new techniques and technologies developing all the time. This article focuses on the new developments in the management of cleft lip and palate patients and the controversies surrounding such technique.
Introduction
Cleft lip and palate is one of the most common congenital craniofacial disorders. Patients born with a cleft deformity might experience problems with feeding, speech, and hearing, as well psychological stresses and issues with social well-being secondary to their aesthetic deformity. To fully address the needs of the cleft patient, a multidisciplinary team approach is required. Complete care of the cleft patient is a challenging task, with new techniques and technologies developing all the time. This article focuses on the new developments in the management of cleft lip and palate patients and the controversies surrounding such technique.
Presurgical infant orthopedics
For many years, surgeons have been attempting to reduce the severity of the deformity before the surgical repair to achieve a better outcome. The field of PSIO emerged based on this need. Reports of attempts to retract the premaxilla in bilateral cleft cases date back to the sixteenth century. Since then, multiple treatments have been developed in an attempt to reduce the deformity before definitive primary lip surgery, including maxillary plates, the Latham appliance, lip taping, elastic bands, lip adhesion, and NAM ( Figs. 1 and 2 ). Infant orthopedics (IO) was first introduced by McNeil in the 1950s and further developed over the following decades. A device that was screwed into the lateral arch segments and activated with pins through the premaxilla was developed by Georgiade and colleagues in the 1960s. The Latham device, developed in the 1980s, is another device that expanded the lateral alveolar cleft segments and deprojected the maxilla by activating a screw mechanism.


Nasoalveolar molding
In the late 1990s, Grayson and Cutting described a presurgical appliance that added additional nasal molding prongs. The NAM technique uses acrylic nasal stents attached to the vestibular shield of an oral molding plate to mold the nasal alar cartilages into more normal form and position during the presurgical period. This technique is based on the technique of molding auricular deformities in the neonate described by Matsuo and colleagues. This technique nonsurgically improves congenital deformities by taking advantage of the plasticity of infant cartilage thought to be the result of increased levels of circulating maternal estrogen during the first 6 months of life. In addition, NAM attempts to lengthen the columella through the application of tissue expansion principles. The columellar improvement is achieved by gradual elongation of the nasal stents and application of tissue-expanding elastic forces applied to the prolabium. The process begins as soon as possible after birth; a custom-made alveolar mold is worn full time with weekly or biweekly adjustments until the alveolar cleft is narrowed to 5 mm or less, achieving the goals of bringing the lip segments together, reducing the alar base width, and relaxing tension on the splayed alar rim. A nasal stent extending from the intraoral plate to the cleft nostril is then added to elevate the alar rim into a more symmetric and convex position.
A recent survey of all surgeons in the American Cleft Palate-Craniofacial Association and the Canadian Society of Plastic Surgeons revealed that 71% of cleft surgeons use some form of presurgical orthopedics at least occasionally and that NAM is used at least occasionally by 38% and greater than half the time by 25% of surgeons. This increase in use in the past 20 years raises the question, Is NAM effective? The purpose of this article is to review the data for and against the use of NAM.
Benefits of nasoalveolar molding
Psychosocial Benefit to Caregivers
Proponents of NAM claim several benefits, including improved aesthetic outcome, reduced overall costs, and a psychosocial benefit to the family. To evaluate the psychosocial effects of NAM, a prospective, multicenter longitudinal study was performed examining 118 caregivers at 6 different cleft treatment centers in the United States. The patients were in 2 groups: those who underwent NAM plus traditional care and those who underwent traditional care only. Although the first year was demanding for all caregivers, NAM onset and the child’s lip surgery were particularly stressful times. Qualitative and quantitative results, however, indicated caregivers of NAM-treated infants experienced more rapid declines in anxiety and depressive symptoms and better coping skills over time than caregivers whose infants had traditional care. This is believed to be because the frequent visits for NAM adjustments reduce caregiver anxiety and lead to a sense of empowerment. These changes arise as a caregiver develops increased skill in managing the NAM appliance, observes improvement in the baby’s appearance, and receives support and counseling from weekly visits to the cleft team.
Clinical Benefits of Nasoalveolar Molding
When evaluating the clinical effects of NAM, they can be broken down into maxillary growth, dentition and occlusion, facial appearance, nasal symmetry, nasal growth, and speech. It has been shown in a randomized controlled clinical trial that non-NAM forms of PSIO offer no measurable advantage or disadvantage in terms of facial growth, facial appearance, maxillary arch dimensions, or occlusion relative to infants treated without PSIO. NAM was not studied, however, in these trials. Proponents of NAM argue that it does have a significant effect on maxillary arch and occlusion. Keçik and Enacar evaluated the effects of presurgical NAM (PNAM) therapy on nasal and alveolar tissues in patients with unilateral cleft lip and palate. They examined the impressions of 22 patients before and after NAM therapy and found a decrease in cleft width and arch length and a significant increase in arch circumference on the affected side. A study from India by Sabarinath and colleagues examined pre-NAM and post-NAM study models of 10 unilateral cleft lip-palate infants. Results from this study showed that NAM was effective in reducing the severity of the initial cleft deformity mainly at the anterior portion of the maxillary arch, because it increased the arch perimeter and intertuberosity distance while decreasing the width of the alveolar cleft and anterior arch length and width.
It is suggested that the primary shortfall of all PSIO techniques other than NAM is that they neglect to address the nasal cartilage deformity during the period of cartilage plasticity. The main difference of NAM from traditional PSIO is the reshaping of the nasal cartilage and providing aesthetic benefits in terms of nasal tip and alar symmetry.
Effect of Nasoalveolar Molding on Nasal Appearance in Unilateral Cleft Lip-Palate
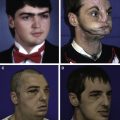
The effect of NAM on nasal appearance is the focus of multiple studies. The few studies with the longest follow-up and evidence level II and level III are described. Barillas and colleagues retrospectively reviewed the results of patients 9 years after NAM and measured nasal symmetry using nasal impressions in stone cast; 15 patients with unilateral cleft lip and palate who had NAM were compared with a group of 10 unilateral cleft lip and palate patients who had not undergone NAM either because of age of presentation or parental preference ( Fig. 3 ). They found that nasal symmetry, including ala projection, dome height, alar groove position, and nasal bridge deviation, was improved by NAM but that columellar deviation was equivalent to non-NAM treatment.

Bennun and colleagues performed a prospective controlled trial of unilateral cleft lip and palate patients. They compared 44 patients managed with an occlusal prosthesis plus NAM to 47 patients who had an occlusal prosthesis alone as well as 48 noncleft controls. The results at 6 years showed the nasoalveolar group exhibited greater nasal tip protrusion, columellar length, and columellar width compared with the non-NAM group, and tip protrusion was similar to that of noncleft controls. Both the NAM and non-NAM groups had greater nasal width than the noncleft controls.
Liou and colleagues examined the progressive changes of NAM by evaluating 25 patients with unilateral cleft lip-palate. They photographically compared preoperative and postoperative and cleft and noncleft nostril appearance. They found an improvement in the ratio of cleft to noncleft nostril height, dome height, columellar length, nasal base width, and nostril width. This improvement was seen after NAM and further improved by cheiloplasty. This improvement partially relapsed after 1 year but remained greater than baseline and then remained stable at 2-year and 3-year evaluations.
Another retrospective study on unilateral cleft lip-palate by Chang and colleagues compared primary rhinoplasty alone, NAM alone, NAM plus primary rhinoplasty, and NAM plus primary rhinoplasty with overcorrection. Photography taken 5 years after surgery showed no difference in nostril height, nostril width, nostril area, or nostril height–to–nostril width ratio. There was a significant difference seen in the NAM groups showing improved symmetry in the medial nostril height and nasal sill height.
Effect of Nasoalveolar Molding on Nasal Appearance in Bilateral Cleft Lip-Palate
These studies all focus on unilateral cleft lip-palate. Fewer studies have been done evaluating bilateral cleft lip-palate. Bilateral cleft lip-palate has a lower incidence compared with unilateral cleft lip-palate ( Fig. 4 ). The incidence of cleft lip-palate is 1 to 2 per 1000 live births, depending on ethnicity, and bilateral clefts are only 15% to 36% of those. The bilateral cleft presents a different set of challenges, although the same presurgical appliance is used. In the bilateral cleft, the alar cartilages have failed to migrate up to the nasal tip and elongate the columella. The alar cartilages are positioned along the alar margins and are stretched over the cleft as flaring alae. In addition, the premaxilla is suspended from the tip of the nasal septum and is often protruded and widely separate from the lateral alveolar segments. The first goal of NAM in these cases must be to move the premaxillary segment posteriorly and medially while preparing the lateral alveolar segments to come in contact with the premaxilla. Several months of appliance adjustments are often required. Delaying repair until 5 months is not uncommon. In addition to orthopedic retraction of premaxilla and molding of the posterior lateral alveolar ridges to an appropriate width to accept the premaxilla, the other goal of NAM in bilateral clefts is columella elongation.

The few studies that focus specifically on bilateral cleft lip-palate show similar trends to the studies of NAM in unilateral clefts: improved nasal symmetry and facial appearance. But long-term studies and controlled trials are lacking. Suri and colleagues compared 29 bilateral cleft lip-palate patients who underwent NAM with 17 patients who had IO only and found significant improvement in columellar length and alignment of alveolar segments compared with those who underwent IO only. Measurements were taken at the time of primary lip repair, but there was no long-term follow-up. Spengler and colleagues found that NAM created a statistically significant reduction of premaxillary protrusion and deviation. Extraoral measurements revealed that there was a significant increase in the bialar width and nostril height as well as increase in the columellar length, width, and deviation. This study included 9 patients, and measurements were compared before and after NAM treatment with no control group.
Garfinkle and colleagues studied 77 nonsyndromic patients with bilateral cleft lip-cleft palate, all of whom underwent NAM and compared them with age-matched controls. Nasal tip protrusion, alar base width, alar width, columella length, and columella width were measured at 5 time points spanning 12.5 years. The nasal tip protrusion, alar base width, alar width, columella length, and columella width were not statistically different from those of the noncleft, age-matched control group at age 12.5 years.
Two long-term studies have evaluated the efficacy of NAM. Liou and colleagues examined basilar photographs of 22 bilateral cleft lip-cleft palate infants before and after NAM, 1 week after cheiloplasty, and yearly for 3 years. The results revealed that the columella was significantly lengthened after NAM and was further improved after primary cheiloplasty. There was a relative relapse in columella length, however, because of the differential growth between the columella and the rest of the nose in the first and second years postoperatively. Again there was no control group in this study. Lee and colleagues performed a retrospective review of 26 consecutive patients with bilateral cleft lip-cleft palate, comparing 13 patients who had a cleft lip repair and nasal correction with banked fork flaps to 13 patients who had nonsurgical columellar elongation with NAM followed by cleft lip closure and primary nasal correction. There was also a group of 13 age-matched controls. Columellar length was measured at presentation and at 3 years of age. The number of nasal operations was recorded to 9 years. The Kruskal-Wallis and Tukey-Kramer tests were used for statistical analysis. The NAM group had significantly greater columellar length than that of the forked flap group and was similar to age-matched controls at 3 years. Furthermore, the NAM group had a significantly reduced the need for secondary nasal surgery.
Effect of Nasoalveolar Molding on Speech Development
The effect of presurgical orthopedics on speech development has shown inconclusive results. Suzuki and colleagues evaluated 17 patients with unilateral and bilateral cleft lip-palate. Analysis of tongue movements was by ultrasound and speech therapist analyzed articulation approximately 4 years after palate repair. They found that infants with cleft palate could not create negative pressure in the oral cavity, even with the presurgical orthopedics. Continuous use of the orthopedics up to the time of palatoplasty seemed effective for the postoperative articulatory, inhibiting irregular movements of the tongue, and possibly preventing “palatalized articulation.”
Karling and colleagues studied 84 patients with unilateral cleft lip and 19 patients with bilateral cleft lip, divided into those treated with presurgical orthopedics and those who were not, and compared them to a group of 40 noncleft controls. All subjects were recorded and judged by professional listeners. No significant differences in articulation or resonance were found between the subgroups of unilateral cleft patients; however, the mean ages at time of evaluation varied from 10.6 for the group who had PSIO and 17.6 years for the group who did not. The results also indicated that the bilateral cleft patients had poorer speech and needed more speech therapy than the unilateral cleft patients. All cleft patients were found to have poorer speech than the noncleft subjects despite considerable speech therapy and complementary surgical treatment.
In a prospective randomized clinical trial (Dutchcleft), patients with complete unilateral cleft lip-palate were followed-up longitudinally at 2 years, 2.5 years, 3 years, and 6 years. One group of 6 infants was treated with IO in the first year of life; the other group of 6 did not receive this treatment. Phonological skills, such as number of acquired consonants, order of phonological development, use of phonological processes, and occurrence of nasal escape, were evaluated. At age 3, the children in the IO group had acquired more initial consonants, suggesting children treated with IO during their first year of life followed a more normal path of phonological development between 2 years and 3 years of age. The trial also examined receptive language skills and expressive language skills. Children treated with IO during their first year of life produced longer sentences than non-IO children at the ages of 2.5 and 3 years. At 6 years of age, however, both groups presented similar expressive language skills. Hence, IO treatment did not have long-lasting effects on language development.
Possible Reduced Overall Costs with Nasoalveolar Molding
Another argument for using NAM is that it reduces overall costs, because the patients have less need for alveolar bone graft and fewer revision nasal surgeries later in life Two studies have looked at the cost of NAM plus surgery versus surgery alone and the likelihood of needing an alveolar bone graft later in life. One found that patients treated with NAM and gingivoperiosteoplasty reduced the need for bone grafting later in life, and the overall cost was therefore reduced. The same conclusion was found when examining exclusively bilateral cleft lip and palate patients. When comparing the rate of revision nasal surgery in patients treated with NAM plus surgery and surgery alone, they found that NAM significantly reduced the risk of undergoing revision surgery. Based on the risk reduction, they concluded that NAM can reduce the number of early secondary nasal revision surgeries and, therefore, reduce the overall cost of care.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


