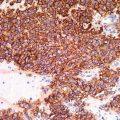
Fig. 17.1
Primary cutaneous adenoid cystic carcinoma. There are nests and islands of cytologically monotonous cells with cribriform architecture
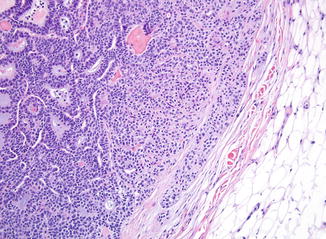
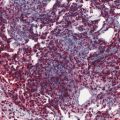
Fig. 17.2
Primary cutaneous adenoid cystic carcinoma. In areas, the growth pattern is more solid. Basement membrane material is focally present and provides a clue to diagnosis. This tumor has invaded the subcutis
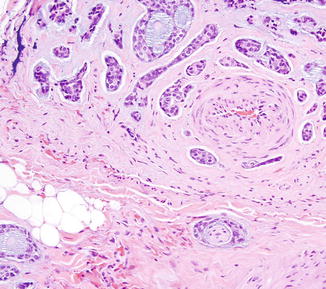
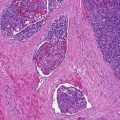
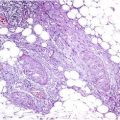
Fig. 17.3
Primary cutaneous adenoid cystic carcinoma. Perineural invasion is seen in a majority of cases and should be searched for diligently
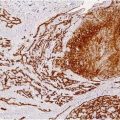
Immunohistochemical staining of these tumors will reveal cytokeratin positivity, with epithelial membrane antigen (EMA), and less consistently carcinoembryonic antigen (CEA) expression in areas of ductal differentiation. Myoepithelial differentiation is noted at least focally in these tumors, as seen with smooth muscle actin, calponin, and/or S100 protein staining in the cells surrounding the pseudoglandular spaces. Expression of p63 in the myoepithelial component is also reported. As in the salivary gland counterpart, CD117 (c-kit protein) is frequently expressed diffusely in tumor cells. The basophilic mucinous material within the pseudocystic tumor spaces stains with Alcian blue.
Differential Diagnosis
Metastasis or direct extension of adenoid cystic carcinoma from salivary gland or other site can be histologically identical and should be excluded clinically. Primary cutaneous cribriform apocrine carcinoma is likely the closest histological mimic to primary cutaneous adenoid cystic carcinoma. This low-grade malignancy arises more commonly on the extremities in a slightly younger age group. It is characterized histologically by exclusively cribriform architecture, variation in the sizes of pseudoglandular spaces, more cytologic pleomorphism, an absence of perineural invasion, and a lack of staining for myoepithelial markers. Primary cutaneous cribriform apocrine carcinoma has an indolent course with lower rates of local recurrence and negligible rates of metastasis than cutaneous adenoid cystic carcinoma, and thus the distinction between these two entities is important. Basal cell carcinoma with an adenoid pattern can be distinguished from adenoid cystic carcinoma by the presence of peripheral palisading and a connection to the epidermis. Additional entities within the differential diagnosis can include mucinous carcinoma, which will lack myoepithelial differentiation but will typically express hormonal receptors, and metastatic adenocarcinoma, particularly of breast origin, which will lack deposition of basement membrane-like material. Adenoid cystic-like patterns have been reported within spiradenomas and spiradenocylindromas and represent a potential pitfall in diagnosis if a lesion is only partially sampled.
Prognosis
In general, primary adenoid cystic carcinoma behaves more indolently than its salivary gland counterpart. A retrospective study based on SEER data estimated a 96 % five-year survival rate. However, local recurrence is not uncommon, occurring in approximately 50 % of cases, although metastatic spread is unusual. More aggressive behavior has been documented in primary adenoid cystic carcinoma arising from the Bartholin glands of the vulva, with high rates of perineural invasion, local recurrence, and an increased propensity for distant metastases to the lung. These adverse effects have been theorized to be related to the high density of nerves in this body site. Unlike salivary gland adenoid cystic carcinoma, histological grading of tumor based on the amount of solid-pattern morphology and mitotic activity did not correlate with recurrence rate or survival in a small series of cases of cutaneous adenoid cystic carcinoma for which outcome data were available.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


