Key Words
cleft palate, Furlow palatoplasty, double opposing Z-plasty, velopharyngeal insufficiency, levator veli palatini, oronasal fistula
Synopsis
A cleft palate represents a developmental failure in separating the oral and the nasal cavities. The communication allows for uncontrolled passage of air, liquid, and food between the two cavities, thus significantly impairing feeding and normal speech development. Anatomically, the levator veli palatine (LVP) muscular sling is disrupted, which is characterized by an aberrant orientation and insertion of the LVP onto the posterior edge of the hard palate, with additional abnormal attachments to the aponeurosis of the tensor veli palatini, and the superior constrictor laterally. Pre-operative genetic screening and evaluation for feeding and airway should be performed and optimized. The goals of palatoplasty are to restore separation of the oral and nasal cavity and to restore the proper anatomical orientation and configuration of the levator muscle, allowing for normal function of the velopharyngeal (VP) port. The Furlow double opposing Z-plasty is the author’s preferred method of palatoplasty and allows proper reorientation of the LVP, lengthening of the palate, and narrowing of the VP port in a single operation. This procedure can be safely performed throughout the world, including in developing countries. Significant post-operative complications include airway compromise, oronasal fistulas (ONFs), and persistent VP insufficiency. The risks of these complications can be significantly reduced intraoperatively with placement of a nasopharyngeal airway, careful and complete dissection of the levator muscle, and preservation of palatal blood supply.
Clinical Problem
Cleft palates are one of the most frequent congenital anomalies, and palate repair carries significant implications for speech, feeding, and airway. Anatomically, a cleft palate is a defect between the oral and nasal cavities, resulting in velopharyngeal incompetence (VPI). Feeding is compromised because negative pressure in the oral cavity cannot be maintained, and feeds are often regurgitated through the nostrils. The disrupted soft palate (velum) precludes separating the oropharynx and the nasopharynx, leading to poorly intelligible speech or VPI. Speech is the outcome measure in palatoplasty.
Overall, the etiology of cleft palates is a combination of genetic and environmental factors, such as maternal smoking, alcohol, corticosteroids, anticonvulsants, high altitude, and advanced parental age. Embryologically, the palate can be divided into the primary and secondary palate. Primary palate refers to the lip, nasal sill, alveolus, and hard palate anterior to the incisive foramen, whereas the secondary palate refers to the hard palate posterior to the incisive foramen and soft palate. The medial and lateral nasal prominences fuse with the maxillary prominences at 4 to 7 weeks of gestation to form the primary palate. The lateral palatal processes of the maxillary prominence rotate and fuse at 8 weeks of gestation to form the secondary palate. Disruption of the migration, rotation, or fusion of these processes results in a cleft palate.
Oral clefts can occur as cleft lip with or without cleft palate (CL/P) or as cleft palate in isolation (CPO). CL/P and CPO are pathogenetically and epidemiologically distinct anomalies. Failure of mesodermal penetration is thought to result in CL/P, whereas CPO occurs from failure of epithelial fusion. CPO has an equal racial distribution, 2 : 1 female/male distribution, and overall incidence of 0.5 : 1000 births. Conversely, CL/P has predilection for Asians (Asian 2 : 1000, White 1 : 1000, Black 0.5/1000) and a 1 : 2 female/male distribution. Both CL/P and CPO can be associated with other congenital anomalies, which can be considered non-syndromic or syndromic. Non-syndromic cleft palates represent an anomaly resulting from a single initiating event or malformation, whereas syndromic clefts involve multiple malformations in multiple developmental fields, frequently occurring together. Pierre Robin sequence (PRS) is a commonly associated anomaly in non-syndromic cleft palate. The triad of micrognathia, glossoptosis, and airway obstruction is a core finding; however, cleft palate is commonly seen but not necessary for diagnosis. In comparison, there are over 300 syndromes that are associated with a cleft palate, of which Stickler syndrome, velocardiofacial syndrome, and Van der Woude syndrome are the most common. Hence patients with a cleft palate should have a genetic screening and consultation.
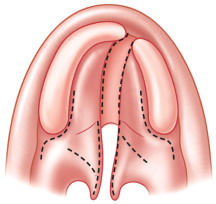
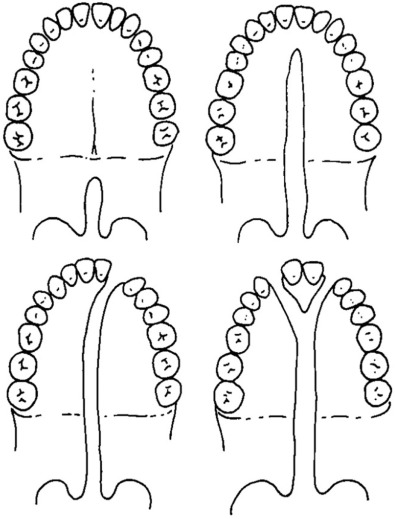
Currently, there are several classification systems (diagrammatic vs symbolic) used to describe oral clefts. The Veau Classification, described in 1931, is diagrammatic and still frequently used when describing cleft palates ( Fig. 3.4.1 ). There are four groups in the classification: (1) clefts isolated to soft palate, (2) clefts of soft palate and hard palate posterior to the incisive foramen, (3) complete unilateral palatal clefts, usually associated with cleft lip and palate, and (4) complete bilateral palatal clefts, usually associated with cleft lip and palate. Submucous cleft palates are not included in the Veau Classification, but represent clefts of the velar musculature with intact mucosa ( Fig. 3.4.2 ).

The goals of primary palatoplasty are (1) complete separation of the oral and nasal cavity, (2) restoration of the anatomy of the velar musculature, and (3) normal speech or VP competence. Feeding is significantly improved with oral-nasal separation, which prevents nasal regurgitation of food/liquid and allows adequate negative pressure to be generated in the oral cavity. Achieving VP competence requires both anatomical and functional correction of the velar anatomy. Restoring velar anatomy can also improve eustachian tube function, which reduces recurrent otitis media and supports improvement in hearing.
Pre-Operative Evaluation and Management
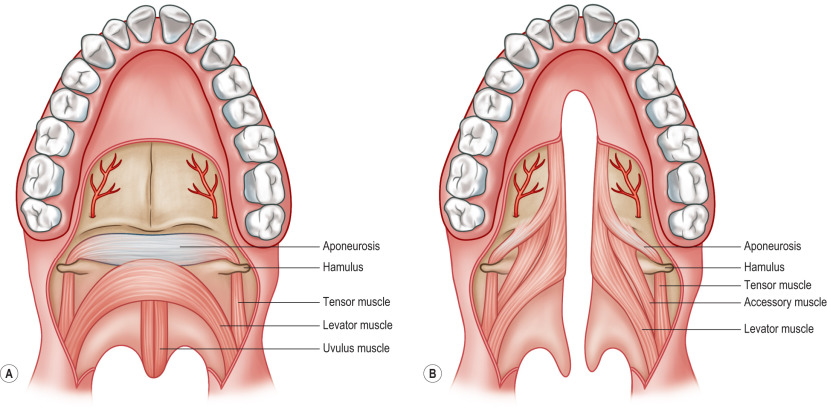
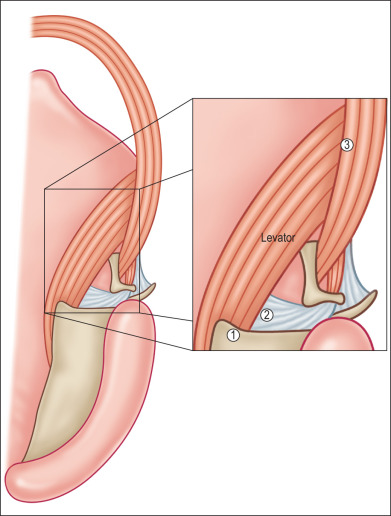
The palate can be functionally divided between the hard and the soft palate. Static structural support and growth via the maxilla are provided by the hard palate, whereas the soft palate (velum) is dynamic and provides VP competence. Normally, the vomer joins the hard palate in the midline, and the LVP muscle, the motor of the velum, forms a sling in the soft palate ( Fig. 3.4.3A ). The LVP muscle originates at the cranial base and courses downward, anterior, and medially to join the contralateral LVP. The LVP sling is situated in the coronal plane within the middle 50% of the soft palate, and acts to pull the velum in a cranial, posterior, and lateral vector to achieve VP competence. Clefts involving the hard palate demonstrate a midline deficiency of bone, resulting in separation of the vomer from the hard palate. Clefts of the velum (including submucous cleft palates) are characterized by disruption of the LVP sling with the muscles coursing in the sagittal plane from posterior to anterior ( Fig. 3.4.3B ). The LVP muscle also has several abnormal attachments in the cleft palate: (1) posterior edge of the hard palate, (2) aponeurosis of the tensor veli palatini, and (3) superior pharyngeal constrictors ( Fig. 3.4.4 ). Adequate palatoplasty must address correcting these anatomical anomalies.
Normal feeding is often disrupted in patients with a cleft palate. The loss of separation of the oral and nasal cavity precludes creating an intraoral vacuum, making bottle- or breast-feeding poor. Patients with concomitant cleft lips have even greater difficulties creating an oral seal during feeding. Several feeding modifications can be used to optimize the process. By reclining the patient from 45 to 60 degrees, gravity can be used to facilitate the delivery of feeds. Delivery of feeds to the posterior aspect of the oral cavity can help reduce the intraoral negative pressure required. Additionally, specialized nipples (Haberman, Mead-Johnson) can allow feeds to be actively delivered, further reducing the need for an intraoral vacuum ( Fig. 3.4.5 ). Before palatoplasty, the patient should be weaned from breast- and bottle-feeding and onto a sippy cup.

Post-operative airway compromise is a significant concern when evaluating a cleft patient for palatoplasty. Palatoplasty acts to narrow the VP port, and with tongue/soft tissue swelling, airway obstruction can readily occur. Patients with cleft palate in the setting of PRS are of particular airway concern given the preexisting small, retro-positioned mandible and glossoptosis. Determining which patients are pre-operatively a high risk is critical in indicating further airway evaluation and optimization. For example, patients who demonstrate breathing difficulties and desaturations when feeding or sleeping may have multi-level airway compromise and should be evaluated by an otolaryngologist; they may require a polysomnography or even an airway intervention before palate repair.
Timing of palatoplasty is relatively controversial. Surgery involving the developing craniofacial skeleton can potentially cause growth disturbances with periosteal devascularization of bone and increased scar restriction. However, prolonging palatoplasty can compromise normal speech development that may then not be surgically correctable. Two-stage palatoplasties have been described wherein the soft palate is repaired “early” and the hard palate is repaired “late.” In theory, the speech advantages of an early repair and the growth advantages of a later repair can be achieved, albeit committing the patient to a second palate procedure. A balance needs to be made between potential maxillary growth restriction with potential abnormal speech development when considering primary palatoplasty. The current literature does not definitively demonstrate that maxillary growth restriction is caused by early palatoplasty. However, any midface deficiency that does occur could be addressed later on with orthognathic procedures, whereas disruption of normal speech development may be more difficult to correct. In this regard, the authors advocate for a one-stage primary palatoplasty at 10 to 12 months of age. In resource-limited settings, this is certainly more feasible compared with staged repair.
Operative Technique
Soft Palate
The velum is the dynamic component of the secondary palate, and its ability to change the VP port contributes significantly to proper speech. Therefore a proper repair must correct the orientation and attachments of the LVP muscles. Currently, there are two general techniques that focus on restoring palatal dynamics: (1) intravelar veloplasty (IVVP), which is the surgical technique of re-creating the anatomical LVP sling, and (2) the Furlow double opposing Z-plasty. The authors strongly advocate the double opposing Z-plasty for its ability to simultaneously (1) reorient the LVP muscles (IVVP) with functional tension, (2) lengthen the soft palate, and (3) narrow the VP port ( ![]() ).
).
The Furlow technique utilizes two pairs of opposing flaps: two oral flaps and two nasal flaps. To reorient the LVP muscles, the design of the flaps must include an oral myomucosal flap and a nasal myomucosal flap on opposite sides of the cleft. Furthermore, because the LVP originates from the skull base posteriorly and abnormally inserts into the bony palate anteriorly, both myomucosal flaps must be posteriorly based to preserve muscle function after elevation. The transposition of these flaps will now result in overlap, reconstructing the normal levator sling (IVVP) in a retro-positioned orientation to provide a better mechanical advantage in closing the VP port.
By convention for a right-handed surgeon, the Furlow design is marked with the posteriorly based oral myomucosal flap on the left side of the cleft ( Fig. 3.4.6 ). Markings are performed with a surgical marking pen after the patient has been prepped and draped with a Dingman retractor in place. The hamuli, uvular bases, and junction of the hard and soft palate at the level of the maxillary tuberosities are initially marked. Relaxing incisions are then marked, starting at the posterior aspect of the maxillary tuberosities, extending posteriorly straight to the retromolar trigone, and curving anteriorly onto the hard palate along the attached gingiva. The cleft margin is marked, connecting the uvular base markings. Of note, this marking is positioned more on the oral side of the oral-nasal mucosal junction to provide more nasal mucosa during flap inset. Next, the lateral limb of the posteriorly based (left side) oral myomucosal flap is marked by connecting the junction of the hard and soft palates at the medial cleft margin to the hamulus laterally. In contrast, the lateral limb of the anteriorly based (right side) oral mucosal flap is marked by connecting the uvular base medially with a point slightly posterior to the hamulus laterally. The lateral extent of the lateral limbs should not connect with the relaxing incisions, preserving a bridge of a mucosa. Furthermore, the angles of the flaps should be slightly asymmetrical, with the left-sided flap approximating 60 degrees and the right-sided flap closer to 60 to 90 degrees. This facilitates insetting the oral flaps. The palate is then injected with bupivacaine and epinephrine.