| Forehead rhytids |
| Brow ptosis below superior orbital rim |
| Heavy brows with thick brow cilia |
| Pre-existing supraciliary rhytids |
| Paralytic eyebrow ptosis (CN VII palsy) |
| High forehead with hair to conceal incision |
| Magnitude of brow ptosis |
| Age and gender of patient |
| Frontalis function |
| Location of hairline and hairstyle (bangs/fringe are best) |
| Quality and quantity of eyebrow cilia |
| Prior eyelid, facial surgery or trauma |
| Presence of concurrent upper dermatochalasis and/or eyelid ptosis |
Introduction
Pretrichial browplasty can be performed for both cosmetic and functional purposes to treat severe brow ptosis. This technique is similar to the coronal browplasty in which a horizontal strip of the forehead is excised, effectively tightening the forehead and raising the brows. Compared to the coronal technique, the pretrichial incision is made just below the hairline, sparing the loss of any cilia. By excising forehead tissue, the brows are raised while the hairline is lowered and, as such, the pretrichial technique is well suited for patients with a high hairline and enough hair to conceal the incision.
With significant lateral brow ptosis, the incision can be extended temporally along the hairline to achieve a satisfactory elevation. The dissection can be extended inferiorly to the level of the forehead depressors where the corrugator, procerus and depressor supercilii can be weakened; however, we rarely perform dissection to this level. Horizontal forehead rhytids can be very effectively treated with pretrichial skin excision similar to the endoscopic technique ( Chapter 22 ). Patients with unilateral or asymmetric brow ptosis can undergo unilateral or more relative forehead excision on one side to address differences in brow position. A midforehead lift can be considered in unilateral facial nerve palsy where dense brow ptosis is present on the ptotic side with no rhytids and severe forehead rhytids from compensatory brow elevation on the normal side. The midforehead incision can be blended into an existing forehead rhytid but the risk of a cosmetically noticeable scar should be discussed with the patient.
If a concurrent upper blepharoplasty is to be performed, the brow ptosis should be corrected first. After establishing the new brow position, the excess skin is then marked for excision. Patients should also be counseled about the risk of hypesthesia, but this typically resolves spontaneously. Although the plane of dissection is subcutaneous and pregaleal, caution should still be given with lateral dissection near the course of the frontal branch of the facial nerve. The pretrichial incision typically heals well but may be noticeable in some patients and this should be appropriately discussed.
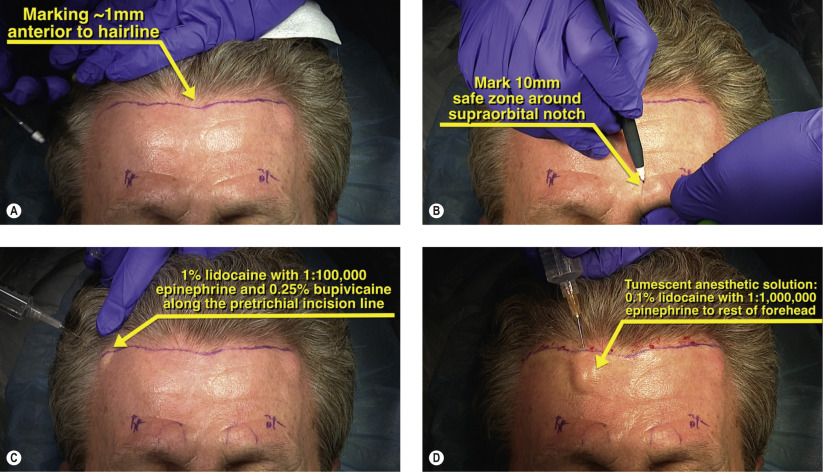
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


