This article presents a thorough review for evaluation of the upper eyelid and brow preceding rejuvenation surgery. It is emphasized that surgical and nonsurgical rejuvenation is directed toward modifying the anatomic causes of facial aging. Relevant anatomy of the lid and brow area is delineated. The discussion includes surgical notes that highlight cautions or tips related to the anatomic area concerned.
Key points
- •
Neither the eyelid nor the eyebrow can be evaluated in isolation, and should be assessed as a unit: the brow-lid continuum.
- •
Recognition and documentation of preexisting functional and cosmetic deficits are paramount to creating a surgical plan and setting realistic expectations for surgical outcome.
- •
Failure to recognize preoperative brow asymmetry in an eyelid procedure may limit the attainment of eyelid symmetry after surgery.
- •
Preoperative recognition of eyelid ptosis and its impact on the position of the eyelid fold and brow assists the surgeon in surgical planning, and enhances the potential for postoperative symmetry.
- •
If the superior sulcus is relatively deep preoperatively, excision of orbital fat is contraindicated.
Videos of complete preoperative evaluation of a [CR] and [CR] accompany this article.
Introduction
The periorbital region is often the first facial area to show signs of aging, and patient desires for aesthetic rejuvenation in this area are extremely common in a facial aesthetic surgery practice. Periorbital aging commonly manifests as brow ptosis, dermatochalasis, rhytids, prolapsed orbital fat, and the associated contour irregularities (hollows). To plan appropriate surgical rejuvenation, one must have a thorough understanding of periorbital anatomy and the tissue changes that lead to the perception of aging.
Surgical and nonsurgical rejuvenation is directed toward modification of the anatomic causes of facial aging. The component parts of the upper third of the face, the forehead, brow, and upper eyelid, are all intimately related and have been referred to as a continuum. When evaluating this region, it is important to avoid assessment of structures in isolation. When examining a patient with dermatochalasis, the eyebrow position must also be evaluated to assess its role in the redundancy of upper eyelid tissue. Similarly, any rejuvenative planning must take into account all the anatomic structures (fat, lacrimal gland, and so forth) that may comprise the brow-lid continuum. Failure to do so can result in undesirable outcomes for both surgeon and patient alike. For example, unrecognized upper eyelid ptosis may be the driver for activation of the frontalis muscle, resulting in chronic elevation of the brow. In this set of circumstances, correction of upper lid dermatochalasis or ptosis may unmask latent brow ptosis when the drive to elevate the brow is diminished after upper eyelid surgery.
The majority of perceived facial cosmetic deficiencies are multifactorial in nature; thus, rarely will a single procedure provide maximal improvement. There are multiple purported causes of facial aging, but contemporary thought focuses on 3 primary mechanisms:
- 1.
Changes related to volume loss or deflation, including loss of bone (remodeling) and fat atrophy
- 2.
Tissue descent
- 3.
Skin changes including rhytids, solar damage, thinning and laxity, and loss of dermal collagen
This context is especially true in relation to the brow and upper eyelid, where combined procedures addressing all 3 factors leading to periorbital aging are often needed.
There are multiple options for repositioning and modifying the shape of the brow, including:
- •
Neuromodulators
- •
Fillers
- •
Fat grafting
- •
Internal or external browpexy
- •
Direct browplasty
- •
Forehead plasty
- •
Endoscopic brow lift
Neuromodulators can be used to selectively treat opposing muscle groups to elevate the brow. Fillers and grafts add volume to the brow, particularly laterally, giving a fuller appearance while causing a mild contour elevation. Surgical brow lift techniques are used to elevate and reshape the forehead and eyebrow while also repositioning the soft tissue of the brow superiorly out of the upper eyelid sulcus. Initial assessment of the brow includes evaluation of height, contour, and the relationship of the brow fat pad to the upper lids. The function of the forehead and brow muscles and their contribution to wrinkling or unevenness of the skin is noted. The underlying structure of the frontal bone, which also contributes to the aesthetic assessment of the brow, is documented.
Blepharoplasty surgery is indicated when the eyelids require recontouring. Blepharoplasty techniques may be used to excise redundant skin and redistribute or remove orbital fat. The assessment of the eyelids includes a layered evaluation of the skin, orbicularis muscle, prolapsed fat, the position of the lacrimal gland, the function of the elevator muscles of the eyelid, and the position of the upper eyelid relative to the globe.
It is necessary to select the appropriate procedure(s) that will provide the optimal results for each individual patient. This process involves not only a clear understanding of the etiology of each patient’s cosmetic deficit(s) but also requires the surgeon to have experience in a variety of different surgical and nonsurgical techniques to enhance the outcome. Also, realizing the effect of any procedure(s) on the brow-lid continuum can reduce the need to perform further corrective procedures.
Introduction
The periorbital region is often the first facial area to show signs of aging, and patient desires for aesthetic rejuvenation in this area are extremely common in a facial aesthetic surgery practice. Periorbital aging commonly manifests as brow ptosis, dermatochalasis, rhytids, prolapsed orbital fat, and the associated contour irregularities (hollows). To plan appropriate surgical rejuvenation, one must have a thorough understanding of periorbital anatomy and the tissue changes that lead to the perception of aging.
Surgical and nonsurgical rejuvenation is directed toward modification of the anatomic causes of facial aging. The component parts of the upper third of the face, the forehead, brow, and upper eyelid, are all intimately related and have been referred to as a continuum. When evaluating this region, it is important to avoid assessment of structures in isolation. When examining a patient with dermatochalasis, the eyebrow position must also be evaluated to assess its role in the redundancy of upper eyelid tissue. Similarly, any rejuvenative planning must take into account all the anatomic structures (fat, lacrimal gland, and so forth) that may comprise the brow-lid continuum. Failure to do so can result in undesirable outcomes for both surgeon and patient alike. For example, unrecognized upper eyelid ptosis may be the driver for activation of the frontalis muscle, resulting in chronic elevation of the brow. In this set of circumstances, correction of upper lid dermatochalasis or ptosis may unmask latent brow ptosis when the drive to elevate the brow is diminished after upper eyelid surgery.
The majority of perceived facial cosmetic deficiencies are multifactorial in nature; thus, rarely will a single procedure provide maximal improvement. There are multiple purported causes of facial aging, but contemporary thought focuses on 3 primary mechanisms:
- 1.
Changes related to volume loss or deflation, including loss of bone (remodeling) and fat atrophy
- 2.
Tissue descent
- 3.
Skin changes including rhytids, solar damage, thinning and laxity, and loss of dermal collagen
This context is especially true in relation to the brow and upper eyelid, where combined procedures addressing all 3 factors leading to periorbital aging are often needed.
There are multiple options for repositioning and modifying the shape of the brow, including:
- •
Neuromodulators
- •
Fillers
- •
Fat grafting
- •
Internal or external browpexy
- •
Direct browplasty
- •
Forehead plasty
- •
Endoscopic brow lift
Neuromodulators can be used to selectively treat opposing muscle groups to elevate the brow. Fillers and grafts add volume to the brow, particularly laterally, giving a fuller appearance while causing a mild contour elevation. Surgical brow lift techniques are used to elevate and reshape the forehead and eyebrow while also repositioning the soft tissue of the brow superiorly out of the upper eyelid sulcus. Initial assessment of the brow includes evaluation of height, contour, and the relationship of the brow fat pad to the upper lids. The function of the forehead and brow muscles and their contribution to wrinkling or unevenness of the skin is noted. The underlying structure of the frontal bone, which also contributes to the aesthetic assessment of the brow, is documented.
Blepharoplasty surgery is indicated when the eyelids require recontouring. Blepharoplasty techniques may be used to excise redundant skin and redistribute or remove orbital fat. The assessment of the eyelids includes a layered evaluation of the skin, orbicularis muscle, prolapsed fat, the position of the lacrimal gland, the function of the elevator muscles of the eyelid, and the position of the upper eyelid relative to the globe.
It is necessary to select the appropriate procedure(s) that will provide the optimal results for each individual patient. This process involves not only a clear understanding of the etiology of each patient’s cosmetic deficit(s) but also requires the surgeon to have experience in a variety of different surgical and nonsurgical techniques to enhance the outcome. Also, realizing the effect of any procedure(s) on the brow-lid continuum can reduce the need to perform further corrective procedures.
Clinical anatomy relevant to evaluation of brow-lid continuum
Forehead and Eyebrows
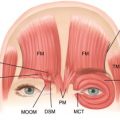
The forehead possesses certain anatomic features that are intimately associated the eyebrow and eyelid Fig. 1 A. The forehead encompasses the area between the hairline and brows, with the horizontal boundaries being the tail of the brows. The position of the hairline varies between individuals, but is usually higher in men than women. Contraction of the underlying frontalis muscles (the paired eyebrow elevator muscles) causes horizontal rhytids of the forehead. The relative distance ratios between the hairline, temporal tuft, and brow can be manipulated with brow and face-lifting surgery. The surgeon must account for these structures when creating a surgical plan.
Eyebrow contour and height
The eyebrow is made up of a head, body, and tail. It generally has an upward contour at the head and a downward contour at the tail. The brow skin has a full complement of layers and appendages that blend gradually into the single layer skin of the upper eyelid. The male and female eyebrows differ in vertical location and contour. In general, the male brow is lower than the female brow, usually at the level of the superior orbital rim. The female brow is slightly higher and has more of a temporal arch. These subtle distinctions are important to recognize, especially during surgical planning for browplasty. With respect to cosmetic outcome, the resultant contour of the eyebrow is just as important as the height. Preoperative assessment will include whether the brow will be lifted symmetrically, or if an attempt to overcome relative medial or lateral brow ptosis will be attempted.
The vertical height of the eyebrow shows more natural variability than the eyelid. For documentation of the original position of the eyebrow, one can assess the margin-brow distance (MBD) from the nasal canthus to the middle of the brow cilia, from the center of the pupil to the middle of the brow cilia, and from the lateral canthus to the middle of the brow cilia ( Fig. 1 B). Although sometimes helpful for research or to objectively document eyebrow position, these measurements are relatively too time-consuming to be practical in a clinical practice. However, for the novice surgeon they may be of benefit until more experience is attained with surgery.
Frontalis muscle
The frontalis muscle is the elevator of the brow and extends from the brow to the forehead, where it merges with the galea aponeurosis. The frontalis muscle is innervated by the frontal branch of the facial nerve.
SURGICAL NOTE: Familiarity with the course of the frontal (temporal) branch of the facial nerve is essential to performing formal brow-lifting surgery, because damage to the nerve can lead to significant morbidity. See the article on anatomy by Lam and colleagues elsewhere in this issue for full a description and depiction of facial nerves.
Because the width of the frontalis stops short of the tail of the brow, the temporal brow lacks a primary elevator. This factor, in association with gravity, squinting, and involutional volume loss, predisposes to the typical brow ptosis of aging. As a consequence of these changes, there is accentuation of the skin fold in the temporal portion of the upper lid, which is commonly misinterpreted by the patient as redundant eyelid skin. Aggressive attempts to remove this skin can cause worsening temporal brow ptosis.
The depressors of the brow include the orbicularis, procerus, and the corrugator muscles.
- •
The orbicularis muscle closes the eyelid and pulls the eyebrow inferiorly.
- •
The procerus muscle has vertical fibers, and contraction causes horizontal rhytids in the glabellar area when depressing the medial head of the eyebrow.
- •
The corrugator muscle pulls the head of the brow medially and inferiorly, causing vertical rhytids in the glabella.
These rhytids are a common concern for patients and are often amenable to neuromodulation, filler treatment, and/or surgical intervention.
In patients in whom the contraction of the muscles is causing bothersome wrinkling, one may consider weakening these muscles by teasing them away from the skin during forehead/brow surgery.
SURGICAL NOTE: Glabellar muscle modification—interrupting the muscle fibers from their skin attachments—helps to diminish rhytid formation. Complete removal of the muscles may be associated with a variety of contour issues, splaying of the brows, and neurosensory deficits. As such, it is best to treat these muscles with a combination of less aggressive surgical muscle modification and neuromodulators.
Rhytid threading or grafting using superficial musculoaponeurotic system (SMAS) tissue harvested during a facelift can aid in softening deep, static rhytids. For patients in whom SMAS grafting is not an option, fillers can be used. Caution should be used with filler selection for this area, as recent studies have shown the potential for severe complications.
Eyelids
Eyelid skin has no subcutaneous fat and is the thinnest of all body skin. Laxity of the upper eyelid skin is due in part to involutional and extrinsic aging and mechanical factors (the constant movement of the upper eyelids and skin tension). The upper eyelids have potential spaces within their architecture, related to the firm attachment of pretarsal skin to the underlying soft tissue, and the loose attachment of similar preseptal tissue. These potential spaces are susceptible to fluid accumulation from involutional changes, sleep position, and/or other insults. The resulting repetitive and chronic skin stretching eventually leads to loss of elasticity, apparent skin redundancy, and a “puffy” eyelid appearance.
SURGICAL NOTE: Whereas the eyelid skin is thin, the eyebrow skin is not. This difference in skin thickness becomes apparent if the upper limb of the blepharoplasty incision is too close to the eyebrow. The subsequent closure will result in thick eyebrow skin annealed to the thin skin of the eyelid, creating a “stepping-off defect” at the incision. This anomaly should be avoided by not placing the upper limb of the incision too close to the brow.
Eyelid crease
The position and symmetry of the upper eyelid crease and fold are important aesthetic features of the appearance of the upper eyelid. The upper eyelid crease is created by the anterior insertion of the levator aponeurosis to the orbicularis muscle and dermis. These attachments prevent the descent of the orbital fat and project tissue anteriorly as the eyelid fold above the crease. The crease is usually 9 to 12 mm above the central lid margin in adult occidental females, and 8 to 10 mm above the lid margin in adult occidental males. The upper lid crease in Asian individuals is lower, usually in the range of 2 to 5 mm from the eyelid margin. In this population, the orbital septum and the orbital fat extend further inferiorly in the eyelid, creating the appearance of a fuller upper eyelid fold than that of the Occidental eyelid. There are additional anatomic differences between Asian and Occidental eyelids, which are important for the surgeon to evaluate and understand when performing eyelid surgery on Asian patients. The review on Asian blepharoplasty by Lee and Ahn elsewhere in this issue details these differences in depth.
Eyelid fold
The lid fold represents the skin, orbicularis muscle, and fat that together drape over and obscure the lid crease when the eye is in primary position. Excessive folding or hooding may result from dermatochalasis, steatoblepharon, brow ptosis, or a combination of all 3 ( Fig. 2 ). Affected individuals may perceive a sensation of lid “heaviness,” early fatigue with reading or watching television, and even loss of superior and/or peripheral vision. To determine an objective measure of the impact of the upper eyelid position on vision, the visual field defect may be demonstrated with automated (Humphrey) or manual (Goldmann) visual field testing. This documentation is required if insurance coverage is sought to cover the expenses associated with upper blepharoplasty.