Surgical rejuvenation of the upper eyelids cannot be performed without taking into consideration the complex aesthetic and anatomic relationships that exist in the upper third of the face. This article discusses the concept of evaluating this facial area as a unit, the brow-eyelid continuum. In addition, the ideal aesthetic goal, the clinical and surgical anatomy, and aging changes relevant to this region are discussed.
Key points
- •
Upper eyelid issues cannot always be addressed in isolation with upper blepharoplasty.
- •
Brow position and contour are integral components of eyelid appearance.
- •
Brows and eyelids should be considered as 1 aesthetic unit: the brow-eyelid continuum.
- •
The ideal distance from the eyelid crease to the central upper brow approximated at 2 times the vertical height of the eyelid crease is subjective, and should be based on the patient’s and surgeon’s aesthetic preferences.
- •
Ocular dominance and Hering law play a role in eyelid and brow position, and manipulation of one component often affects the position of other components.
- •
A multiprocedure approach involving ptosis repair, volumetric supplementation, and brow lifting in conjunction with conventional upper blepharoplasty is often necessary for ideal aesthetic improvement of the brow-eyelid continuum.
Introduction
Surgical rejuvenation of the upper eyelids cannot be performed without taking into consideration the complex aesthetic and anatomic relationships that exist in the upper third of the face. A surgeon who aims for successful eyelid rejuvenation with upper blepharoplasty in isolation may have difficulty attaining a personally satisfactory outcome, and, most importantly, may not meet the patient’s expectations. When evaluating a patient, the upper eyelids should be viewed in contiguity with the other structures forming the upper third of the face, including the eyebrows, forehead, and the location of the frontal hairline. The term brow-eyelid continuum may help guide the patient’s understanding that any or all of these structures may require treatment to obtain a harmonious and aesthetically pleasing rejuvenation.
Introduction
Surgical rejuvenation of the upper eyelids cannot be performed without taking into consideration the complex aesthetic and anatomic relationships that exist in the upper third of the face. A surgeon who aims for successful eyelid rejuvenation with upper blepharoplasty in isolation may have difficulty attaining a personally satisfactory outcome, and, most importantly, may not meet the patient’s expectations. When evaluating a patient, the upper eyelids should be viewed in contiguity with the other structures forming the upper third of the face, including the eyebrows, forehead, and the location of the frontal hairline. The term brow-eyelid continuum may help guide the patient’s understanding that any or all of these structures may require treatment to obtain a harmonious and aesthetically pleasing rejuvenation.
Clinical significance of the brow-eyelid continuum
The forehead-eyebrow complex is a critical aesthetic component of the upper facial third. The position and contour of the eyebrows play a role in the appearance of the eyelids. A ptotic brow, whether caused by gravitational changes or loss of three-dimensional volume in the brows and temples, can cause apparent increased skin redundancy and fullness in the upper sulcus and the temporal eyelid. These changes exacerbate the appearance of temporal eyelid hooding. The frontalis muscle, the prime elevator of the brow, contributes 2 mm of elevation to the upper eyelid, and thus overall resting frontalis tone can affect the position of the upper eyelid margin relative to the pupil. When assessing the upper eyelids, the brows should be placed in a position consistent with the patient’s appearance in youth. Old photographs are invaluable in customizing brow position to the patient.
Aging changes evidenced in the brow-eyelid continuum are related to complex alterations in the orbital rim (bone), fat compartments of the brow and lids, and skin. The traditional subtractive upper eyelid blepharoplasty addresses redundant skin, muscle, and fat, but usually does not fully address these complex alterations. Most patients benefit from additional procedures to address these associated periocular aging issues, such as volume augmentation, brow lifting, and skin resurfacing. When these senescent changes are addressed as a whole, a conservative blepharoplasty, often with only skin removal with minimal fat excision or preservation, can be performed to attain a more pleasing aesthetic result.
Excess Upper Eyelid Skin and Ptosis
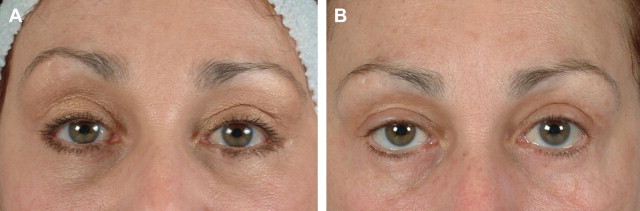
Dermatochalasis, defined as the appearance of excess skin in the upper eyelids, is a chronic condition that produces compensatory frontalis muscle overaction as the eyebrows raise to elevate excess skin off the eyelashes. Upper eyelid ptosis also produces similar compensatory frontalis contraction. Patients with these conditions often appear to have excellent brow position, but with significant horizontal forehead rhytids; however, when the frontalis is put at rest by the examiner’s finger, with gentle pressure downwards to eliminate the forehead rhytids, these patients often manifest significant brow ptosis.
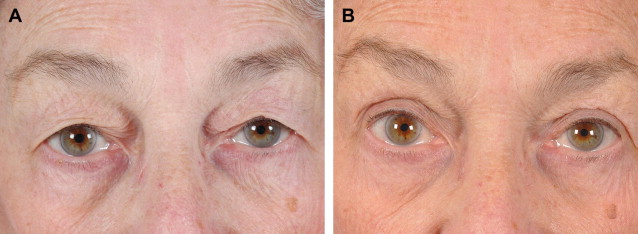
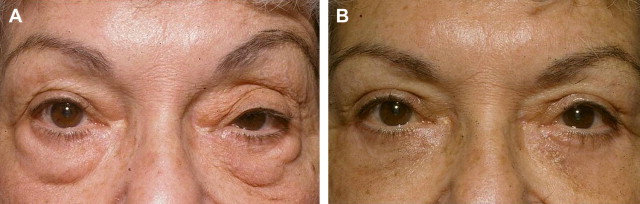
Isolated blepharoplasty in these patients unmasks this latent brow ptosis because the patient no longer needs to compensate for mechanical ptosis by contracting the frontalis ( Fig. 1 ). This procedure often leads to a poor aesthetic result. Bilateral ptosis repair also eliminates the drive for frontalis activation, and also unmasks brow ptosis and can compromise the aesthetic result when performed as an isolated procedure ( Fig. 2 ). In both of these clinical situations, it is important to discuss the need for brow lifting surgery to prevent patient disappointment with the postoperative result. Many patients either opt for simultaneous brow lift or are prepared to deal with the aesthetic consequences if eyelid surgery alone is chosen.
Hering’s Law Applied to Blepharoplasty and Ptosis Repair
In 1868, Ewald Hering described what is now known as the Hering law, stating that there is equal and simultaneous innervation to synergistic ocular yoke muscles. Afferent innervation to the brainstem from the visual system drives a bilateral symmetrically mediated motor response that aligns the eyes. This phenomenon was first described to explain how, when fixating on a moving visual target, the eyes move symmetrically while maintaining fusion. The Hering law also applies to the frontalis and levator muscles, and is the principle underlying the drop in the brows seen when blepharoplasty or ptosis repair is performed (as described previously). According to this principle, the paired levator and frontalis muscles are symmetrically innervated from a motor standpoint, and correction of upper eyelid ptosis or dermatochalasis diminishes afferent input to the frontalis muscles, causing the brows to drop.
In cases of upper eyelid position asymmetry, such as in unilateral ptosis, the Hering law is equally important. In these cases, ocular dominance (preferred eye) must be determined. The dominant eye is the preferred afferent input that drives symmetric bilateral motor innervations to the levator muscle. In cases of asymmetry, it can be assumed that alteration in the dominant eye’s eyelid position may have an effect on the contralateral eye’s lid position. This assumption can not be made when the nondominant eye is ptotic, and unilateral ptosis repair may be performed without alteration of the contralateral lid position. However, in cases in which unilateral ptosis occurs in the dominant eyelid, compensatory elevation of the contralateral (nonptotic) eyelid can occur. Once the unilateral ptosis is surgically corrected and the increased tone of the levator muscles is diminished bilaterally, latent ptosis may become evident in the contralateral (nondominant) eyelid, either at the time of surgery or afterward. Thus, in cases of asymmetric bilateral ptosis or unilateral ptosis in the dominant eye, it is best to anticipate the potential to perform bilateral ptosis surgery.
Unilateral eyelid asymmetries can also have an effect on brow position because the impetus for frontalis muscle contraction is also not always symmetric. Asymmetric brow elevation can therefore be seen in patients with unilateral ptosis, with the ptotic eyelid appearing symmetric to the contralateral side ( Fig. 3 ). An association between involuntary asymmetric eyebrow elevation and ocular dominance has been described, with ocular dominance matching the side of unilateral eyebrow elevation 77% of the time. Unilateral brow asymmetries are also commonly seen in patients with preexisting conditions such as Bell palsy, previous trauma to the VII nerve, and scar tissue in the forehead from trauma or surgery. Thus, when evaluating the patient, it is important in all these instances to elevate the ptotic brow and depress the elevated brow to rule out unilateral compensatory frontalis overaction that could be concealing an eyelid ptosis.
Neurotoxin Effect on Brow-Eyelid Continuum
Now that the use of neurotoxins has become commonplace for the treatment of glabellar and transverse forehead wrinkles, their effect on the brow-eyelid continuum must be considered. It is common to evaluate patients for brow or upper eyelid ptosis who have exacerbated a preexisting condition such as upper eyelid skin excess or brow ptosis with neurotoxin placement. Depending on the placement and quantity of the neurotoxin injections, brow and eyelid contour can be significantly altered. It is common in our practices to see patients in consultation for blepharoplasty who have undergone recent injections and have not made the connection between their sudden skin excess or brow ptosis and their neurotoxin treatment.
Brow-Eyelid Continuum Evaluation
The upper eyelids must not be considered in isolation in evaluating patients for upper eyelid aesthetic surgery. Asymmetries of the upper eyelid or brow position must be carefully assessed before surgery, and often the solution to a unilateral problem involves bilateral surgery. Because of the integration of the brow-eyelid continuum, the region must be evaluated as a whole, even when the presenting issue seems obvious.
Aesthetic anatomy of the face
Since the Renaissance, scholars and artists have developed guidelines for ideal facial proportions that continue to be studied, modified, and debated. A wide variation exists in the ideal aesthetic of the upper third of the face and is influenced by age, sex, culture, and ethnicity. Alterations in what is considered aesthetically desirable also vary based on fashion and the epoch. The widespread use of Botox (Allergan, Inc., Irvine, CA) and its congeners may have altered perceptions of what is attractive in the periorbital region, because fashion models and celebrities often are photographed with brow ptosis or peaked brows from selective paresis of muscles. Although there is no universally applicable ideal eyebrow position and contour, certain principles must be followed to maintain harmony within the periorbital region. Following is a summary of the current guidelines of ideal aesthetics in the upper third of the face based on published anatomic guidelines.
Hairline, Forehead, and Temporal Fossa
Understanding the aesthetic anatomy of the hairline, forehead, and temporal fossa is important in achieving a balanced and harmonious rejuvenation of the upper third of the face. This area is often overlooked when rejuvenating the eyebrows and upper eyelids, because certain techniques of brow lifting elevate the hairline, leading to a disproportionately long forehead with a receded hairline. The hairline is variable between individuals. The average male hairline height is 6.5 to 8 cm measured from the trichion to the supra-eyebrow line. The female hairline is lower, between 5 and 6 cm. The forehead is delineated by the hairline superiorly, the glabella inferiorly, the frontonasal groove centrally, and laterally by the lateral brow. The forehead should transition smoothly to the temple. In general, the diagonal distance between the lateral brow and the temporal tuft should be less than 3.5 cm.
Eyebrows
The brow frames the appearance of the upper eyelid. Subtle alterations in brow position convey an array of emotions, from anger to surprise. Best described by Laorwong and colleagues, the brow is shaped like a curved sword. The superior brow edge is arched and tapered laterally. The horizontal length of the brows can measure 5.0 to 5.5 cm with a width of 1.3 to 1.5 cm. Men in general have thicker brows than women. The cilia in the medial brows are finer and directed upward. As the brow tapers laterally, the superior and inferior cilia are more transversely oriented and direct toward each other at approximately a 30° angle.
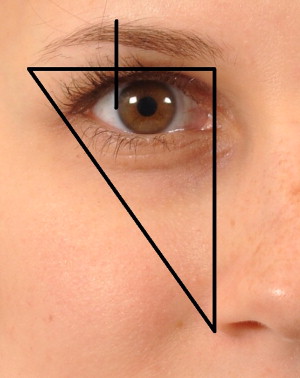
The basis of the modern ideal female brow was described by Westmore in 1974. The ideal brow is gently curved, with its apex aligned approximately above the lateral corneal limbus. The medial brow edge should begin on the same vertical line as the lateral nasal ala and the inner canthus. The lateral brow edge should end at the oblique line that is described by the lateral nasal alae and the lateral canthus ( Fig. 4 ). The male brow should have similar medial to lateral alignment; however, it is usually lower and straighter.
Additional aesthetic determinants of ideal brow position and contour have been reported since Westmore’s description; many of these are in conflict. Ellenbogen thought that the brow was most aesthetically pleasing 1 cm above the supraorbital ridge, whereas Whitaker and colleagues thought the ideal brow should be slightly below the supraorbital ridge. The greatest point of curvature of the brow has also been debated. Cook and colleagues, Ellenbogen, and Whitaker and colleagues thought that the greatest curvature of the brow is positioned more laterally. Pham and colleagues reported that the apex of the temporal curve correlates best with the temporal fusion line, and occurs more laterally. These contradictions arise because the aesthetic ideal is subjective.
The preference of brow position and contour can also depend on the age of the beholder. In one study, individuals younger than age 30 years preferred lower positioned brows, whereas those more than age 50 years preferred higher, more centrally arched brows. An explanation of this phenomenon could be that individuals conceptualize beauty during their youth. The appearance of the youthful brow shape and position has changed through the years. Early in the 1930s and until the 1970s, the high arched eyebrow with the apex in the middle was the most popular brow shape. The projected youthful brow in most fashion magazines is currently characterized by thick, full, and low-set eyebrows.
Objective guidelines for determining ideal brow position
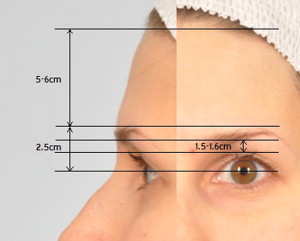
To make the subjective nature of brow position and contour more objective, investigators have proposed numeric guidelines for ideal brow position ( Fig. 5 ).
- •
Connell and colleagues estimated the distance between the upper eyelid crease to the lower eyebrow edge at 1.5 cm.
- •
Matarasso and Terino estimated the distance from the upper edge of the eyebrow to the hairline as 5 to 6 cm, the lower edge of the middle eyebrow to the eyelid crease as 1.6 cm, the lower edge of the eyebrow to the midpupil as 2.5 cm, and the lower edge of the middle eyebrow to the superior orbital rim as 1 cm.
- •
McKinney and colleagues described the distance from the midpupil to the upper edge of the eyebrow as 2.5 cm and the distance from the upper edge of the eyebrow to the hairline as 5 cm, on average.
- •
Numeric guidelines such as these provide a useful starting point, but cannot be applied universally because of variations among individuals.
Variables in determining ideal brow position
The racial composition of the patient is a variable that makes numeric determinations of ideal brow position universally challenging. Inter-racial anthropometric analyses of the eyebrows and eyelids were conducted by Kunjur and colleagues, in which 3 different racial groups, white, Indian, and Chinese, were compared. The investigators found that the eyebrow was arched and bow shaped in all subjects and that the apex of the brow was between the lateral canthus and the lateral limbus, except in Indian men, in whom it was about 1 to 2 mm lateral to the lateral canthus. Price and colleagues, in their study comparing eyelids and brows between African Americans and white people, found that African Americans had an overall higher brow position than white people. No significant racial differences were found in regard to the shape and apex of the brow.
Facial shape is an important factor in the determination of an individualized ideal brow position. Some investigators think that vertically long faces should have a flatter brow to give the appearance of a fuller face, whereas, for square faces, an accentuated lateral curvature may help soften the angles. Thus, the ideal brow is a dynamic concept that takes into consideration not only the anatomy of the upper third of the face but the face as a whole. This precept is important in achieving a balanced, natural surgical result.
Despite numerous attempts to define the ideal position and contour of the brow, the results remain subjective. The surgeon should solicit the patient’s opinion regarding individual preference on brow position and contour, then advise the patient as to whether these preferences can realistically be attained. The surgeon should also be honest about the aesthetic merits of the patient’s chosen position.
Upper Eyelids
Ideal eyelid appearance varies with gender, race, and age. In general:
- •
The upper eyelid should rest approximately 1 to 2 mm below the superior corneal limbus.
- •
The lower eyelid should rest on or 1 mm above the inferior corneal limbus.
- •
The opening between the eyelid margins, the vertical palpebral fissure, measures 9 to 10 mm, whereas the horizontal aperture measures 28 to 30 mm.
- •
Normal eyelid levator function is 14 to 16 mm and is defined as the excursion of the upper eyelid margin from downgaze to upgaze with the frontalis immobilized.
- •
The greatest curve of the upper eyelid is observed slightly medial to the pupil, whereas the lower eyelid’s greatest curve is seen lateral to the midpupillary line.
- •
The horizontal palpebral fissure is inclined with a slight upward tilt with the lateral canthus positioned about 2 mm above the medial canthus. In a comparative inter-racial study, Kunjur and colleagues found that canthal tilt varied among races. The author found that canthal tilt was greatest in Chinese subjects (5.7°), then white people (4.0°) and then Indians (1.2°).
- •
The eyelid crease, a significant component of eyelid aesthetics, is formed by the subcutaneous insertion of the levator aponeurosis onto the anterior lamella and varies in position with age, sex, and race. Eyelid crease height is generally higher in women than in men. The eyelid crease, as measured from the lid margin, is characteristically described to be 8 to 10 mm in men and 10 to 12 mm in women. In a recent study comparing white and African American eyebrow and eyelid dimensions, African Americans were found, in general, to have higher eyelid creases.
Asian eyelid crease
The aesthetic appearance and anatomy of the Asian eyelid crease are unique and variable. The average Asian eyelid crease height is approximately 5 to 7 mm. Park’s study of the anthropometry of Asian eyelids revealed the average eyelid crease height to be 6.6 mm in men and 6.5 mm in women. In the Asian eyelid there are 3 commonly described variations:
- 1.
Apparent double eyelid
- 2.
Inner eyelid fold with a low-lying crease
- 3.
Single eyelid that does not have an eyelid crease
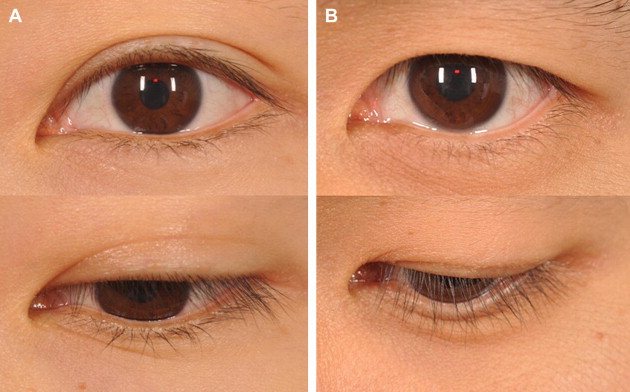
The apparent double eyelid and the inner eyelid fold with a low-lying crease make up most of the Asian eyelids observed ( Fig. 6 ). Compared with the white eyelid, the Asian eyelid has been described to have a lower insertion point of the orbital septum onto the levator aponeurosis. This anatomic difference results in an inferior extension of the preaponeurotic fat pad creating a thicker and lower eyelid crease. Kakizaki and colleagues, using cadaveric Asian eyelids, recently showed that the distal end of the levator aponeurosis insertion site was located above the superior tarsal border, similar to its insertion site in white eyelids. This study suggests that the anatomic differences observed between Asian and white people are caused by inherent differences in upper eyelid fat volume rather than the attachment site of the orbital septum to the levator.
Surgical anatomy of the face
Forehead and Brows
Bony landmarks
The frontal and nasal bones are the primary bony landmarks encountered in aesthetic brow and upper eyelid surgery.
- •
In most patients, the supraorbital nerve originates from a notch over the superior orbital rim.
- •
In approximately 20% of patients, the nerve exits through a foramen.
- •
In 10% of patients, a lateral branch of the nerve exits the frontal bone approximately 2 cm above the rim.
Surgical note: The surgeon should be familiar with the location of these nerves to avoid injury, especially during dissection.
Muscles
The main elevator of the eyebrow and forehead is the frontalis muscle. The paired frontalis muscles join the occipitalis muscles posteriorly, the galea aponeurotica anteriorly, and the temporal fascias laterally. Frontalis fibers interdigitate with the orbital portion of the orbicularis muscle near the supraorbital rim and insert into the dermis beneath the eyebrow. The activation of the frontalis produces horizontal rhytids of the forehead skin.
The procerus and corrugator supercilii muscles are the primary brow depressors, along with the orbicularis to a lesser extent. Their origins, insertions, and primary actions are described later.
Soft tissue and suspensory ligaments
The forehead is usually described in layers from the skin to the periosteum :
- •
Skin
- •
Connective tissue
- •
Aponeurosis, which fuses with the frontalis muscle
- •
Loose connective tissue
- •
Galea
- •
Periosteum
Surgical note: Adhesion zones have been described for the frontal periosteum by Moss and colleagues. They are strongest along the frontal bone in the vicinity of the superior temporal crest ligament, and extend to the origin of the corrugator muscle.
- •
The inferior border of this adhesion zone is located 6 mm above the deep attachment of the periorbital septum.
- •
The upper border extends 20 to 40 mm above the orbital rim.
The galea aponeurotica descends laterally into the temporal fossa as the superficial temporal fascia. The galea aponeurotica splits anteriorly into a superficial and deep layer to include the frontalis and the orbicularis muscle. At the level of the brow, the deep layer of the galea also splits into an anterior and posterior facial layer to enclose the retro-orbicularis oculi fat (ROOF). The posterior facial layer continues as the orbital septum of the eyelid, eventually fusing with the levator aponeurosis.
The conjoined tendon is an area of fusion between the soft tissues of the forehead and the fascias of the temple and is an important landmark in endoscopic brow surgery. The deep temporal fascia (DTF), superficial temporal fascia (STF), and frontal periosteum fuse forming the conjoint tendon. The inferior temporal septum, described by Moss and colleagues, represents another area of confluence between deep and superficial tissues.
Surgical note: At this location, the DTF splits into its superficial and deep layers to envelope the superficial temporal fat pad, and is a landmark that is important in brow surgery. This zone of adhesion exists along a line approximately 1 cm above the course of the frontal branch of the facial nerve. This area must be traversed deep to the temporal branch of the facial nerve to avoid injury.
Perforating veins and sensory nerves (the medial and lateral zygomaticotemporal nerves) are pertinent landmarks that indicate that the nerve is superficial to the plane of dissection.
Temporal region
The temporal region is complex and multilayered.
Surgical note: The frontal branch of the facial nerve is vulnerable at several locations in this dissection. It is important for the surgeon to become well acquainted with the anatomy of this region before embarking on surgery.
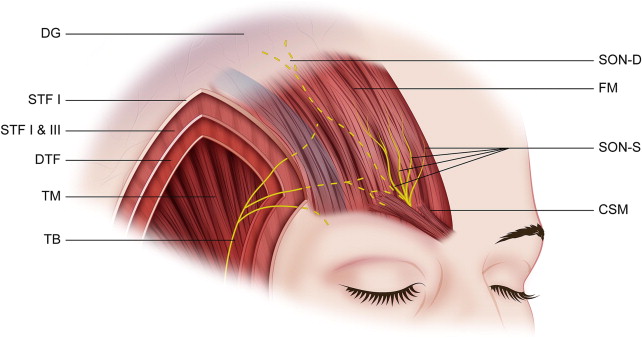
The superficial musculoaponeurotic system (SMAS) of the temple is composed of the temporoparietal fascia (TPF; also known as the STF), the most superficial fascial layer in the temple. Deep to this, the superficial portion of the DTF is observed; a white glistening fascia that is easily separated from the TPF above. This loose areolar layer between the TPF and the DTF has been referred to as the subaponeurotic plane ( Fig. 7 ).
The DTF splits into a superficial and a deep layer as it further descends toward the zygomatic arch. The superficial temporal fat pad is encased between the superficial and the deep layers of the DTF. In this location, the superficial portion of the DTF is also known as the intermediate fascia, or the innominate fascia, and the fat pad is known as the intermediate fat pad. The deep layer of the deep temporalis fascia covers the temporalis muscle and blends inferiorly with the parotidomasseteric fascia of the face.
ROOF
Beneath the ciliary portion of the brow and accompanying orbicularis is a fat pad encased in septated connective tissue. This fat compartment, the ROOF pad, continues into the upper eyelid as the postorbicularis fascia (POF).
Surgical note: Although some investigators have advocated resection of the ROOF to improve the contour of the lateral eyelid, deformities related to resection can ensue and this can add to normal involutional eyebrow/eyelid deficits. Instead, vertical elevation of the ROOF via a brow lifting procedure is often necessary to achieve the desired contour of the brow-eyelid continuum.
In Asian people, the ROOF continues into the lid proper as a fatty layer called the preseptal fat, located between the orbicularis muscle and orbital septum. This layer contributes to the apparent fullness of the Asian upper eyelid.
Eyelids
Upper eyelids
The upper eyelid skin is the thinnest skin in the body because of its lack of subcutaneous fat. It is thinnest near the ciliary margin and becomes thicker approaching the eyebrows. The eyebrow skin is significantly thicker, containing sebaceous glands, sweat glands, and hair follicles.
The eyelid margin is approximately 2 mm in width. From anterior to posterior, the eyelid margin consists of the skin, the eyelashes, the gray line (terminal orbicularis muscle), the tarsus with associated meibomian gland orifices, and the mucocutaneous junction.
Surgical note: The gray line serves as an important surgical anatomic landmark and represents the muscle of Riolan, which is the most anterior and superficial portion of the pretarsal orbicularis muscle. The gray line is useful to the surgeon in aligning the eyelid margin.
The eyelid can be divided through the gray line into 2 segments:
- 1.
Anterior lamellae
- 2.
Posterior lamellae
Throughout the eyelid, the anterior lamella is composed of skin and orbicularis muscle. Above the tarsus, the posterior lamella is composed of the eyelid retractors and palpebral conjunctiva. Below the tarsus, the posterior lamella consists of the tarsus and conjunctiva. Connective tissue attachments of the levator aponeurosis traverse anteriorly and attach to the pretarsal orbicularis muscle and skin, forming the upper eyelid crease.
Tarsus
The tarsal plates are rigid structures formed from connective tissue (collagen type I, III, VI, and multiple glycosaminoglycans) and serve as the supporting framework of the eyelids. Within the tarsus are meibomian glands that secrete mebum, the oily external component of the 3-layered tear film. The tarsal plates measure approximately 29 mm horizontally, with a thickness of 1 mm. The superior tarsus has a vertical height of 8 to 12 mm. Asian people have a smaller superior tarsal plate, with a vertical height measuring 8 mm.
Orbital septum
The orbital septum is a fibrous multilayered connective tissue that originates at the arcus marginalis, a circumferential thickening of periosteum at the orbital rim. The orbital septum defines the separation of the orbit proper from the eyelid, and can be thought of as a physical barrier that encloses the orbital fat and internal orbital structures. The septum fuses with the levator aponeurosis in the upper eyelid and the capsulopalpebral fascia in the lower eyelid.
Surgical note: It is imperative the orbital septum never be sutured when closing a blepharoplasty incision or lid motility dysfunction can result.
Eyelid/orbital fat
The eyelid fat compartments or pads lie posterior the orbital septum. The upper eyelid has 2 distinct fat compartments, nasal and central, separated by a connective tissue septum. The nasal fat is in continuity with deeper orbital fat because it is not separated from extraconal and intraconal fat by the levator aponeurosis. The central fat compartment is an important landmark in upper eyelid surgery because it lies directly anterior to the levator aponeurosis. The potential space between the orbital septum and the levator aponeurosis is greatest immediately inferior to the superior orbital rim over the central fat pad, and therefore is an ideal location for dividing the orbital septum to expose the fat without injury to the levator and other deep structures. This preaponeurotic fat pad can be differentiated from the nasal fat pad by its color. The central fat pad has a yellow appearance, whereas the nasal fat pad has a whiter appearance. This color difference has been attributed to a higher carotenoid and retinol content in the central fat pad. Korn and colleagues suggest that this difference relates to differing embryologic origins, with the central fat pad derived from mesodermal cells and the nasal fat pad from neural crest cells.
Lacrimal gland
The lacrimal gland is a bilobed structure composed of orbital and palpebral segments divided by the lateral horn of the levator aponeurosis. The orbital lobe lies in the lacrimal fossa located in the superior lateral orbit and is connected to the palpebral lobe posterior to the lateral horn of the levator. With aging, the lacrimal gland can prolapse, adding to brow/sulcus fullness. Lacrimal gland prolapse has been reported to occur in 15% of patients and may be associated with normal aging of the orbit. The dehiscence of the fibrous interlobular septae that connect the gland to the orbital rim fossa, along with thinning of septal connective tissue, contribute to prolapse of the lacrimal gland.
Eyelid Muscles
Protractors
The circular orbicularis oculi muscle, the main protractor of the eyelid, lies directly beneath the eyelid skin. The orbicularis oculi muscle, innervated by the facial nerve (cranial nerve [CN] VII), encircles the orbit and eyelids, extending beyond the orbital rim. The orbicularis is divided into 3 segments, all named for the structures they overlie:
- 1.
Pretarsal segment
- 2.
Preseptal segment
- 3.
Orbital segment
The pretarsal portion rests over the upper and lower tarsal plates, the preseptal portion over the orbital septum, and the orbital portion over the orbital rim. The orbicularis acts both voluntarily to close the eyes and involuntary with the blink mechanism. The action of the pretarsal and preseptal orbicularis contribute to lacrimal drainage via the lacrimal pump mechanism.
The pretarsal orbicularis fibers insert at the canthal tendon laterally and originate from 2 locations medially: the posterior lacrimal crest (deep head) and the anterior limb of the medial canthal tendon (superficial head). The superficial and deep heads of the upper and lower pretarsal orbicularis collectively form the Horner muscle, located posterior to the medial canthal tendon. Preseptal orbicularis fibers originate medially from the superficial and deep heads. The preseptal superficial head originates from the medial canthal tendon and the deep head originates from the fascia of the lacrimal sac and medial orbital wall above and below the Horner muscle. The orbicularis laterally inserts into the lateral palpebral raphe. The superior portion of the orbital orbicularis muscle is formed from fibers originating from the anterior limb of the orbital portion of the frontal bone. The orbicularis fibers interdigitate with the frontalis muscle superiorly, procerus and corrugators supercilii muscle medially, and anterior temporalis fascia laterally.
Three muscles (brow depressors) work in conjunction with the orbicularis to aid in upper eyelid closure:
- 1.
Procerus
- 2.
Corrugator supercilii
- 3.
Depressor supercilii
The procerus muscle originates on the nasal bone, inserting into the skin of the nasal bridge and lower forehead. Contraction results in an inferior-directed force that causes medial brow descent and the formation of horizontal glabellar rhytids.
The paired corrugator superciliaris muscles originate in the medial superciliary ridge and extend obliquely superolaterally where they blend with the frontalis and orbicularis oculi muscle, and insert onto the skin of the middle eyebrow. Activation of the muscle results in inferomedial depression of the medial brow and the development of vertical glabellar furrows.
The depressor supercilii originates from the frontal process of the maxilla about 1 cm superior to the medial canthal tendon and ascends superiorly to insert in the skin about 14 to 15 mm superior to the medical canthal tendon. Activation of the muscle also depresses the medial brow and contributes to the formation of oblique glabellar frown lines.
Retractors
There are 2 upper eyelid elevating muscles:
- 1.
Levator palpebrae superioris
- 2.
Müller muscle
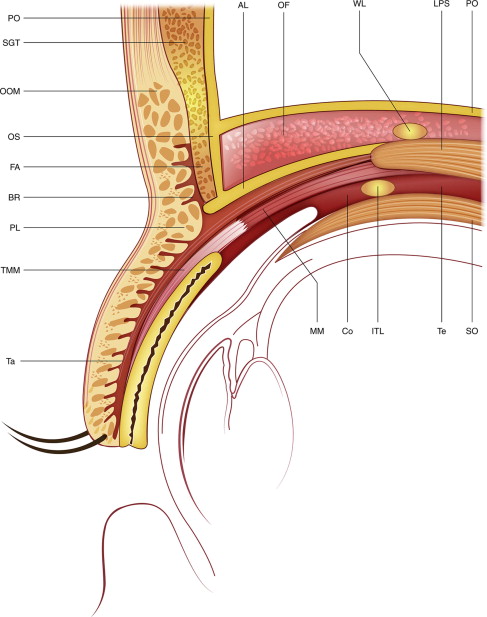
Levator muscle
The levator is the primary retractor of the upper eyelid. It is innervated by the superior division of CN III, which enters the muscle approximately 12 mm from the orbital apex. The levator muscle originates from the lesser wing of the sphenoid at the orbital apex. It extends anteriorly above the superior rectus muscle until the Whitnall ligament (the superior transverse ligament), where it transitions into the levator aponeurosis and inserts onto the anterior surface of the tarsus. The orbital (muscular) portion of the levator has a horizontal vector of action, whereas the aponeurotic portion has a vertical vector ( Fig. 8 ). The levator muscle with its aponeurosis measures 54 to 60 mm in length from origin to insertion, with the aponeurotic portion of the levator complex being 14 to 20 mm.