Key Words
premalignant, nonmelanoma, basal cell carcinoma, squamous cell carcinoma, Merkel cell carcinoma, actinic keratosis, actinic cheilitis, leukoplakia, lymphoma, T-cell lymphoma, Sézary syndrome, Bowen disease, Paget disease, in situ, biopsy, Mohs micrographic surgery
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is the most common invasive malignant cutaneous neoplasm found in humans. The most common presenting complaint is a bleeding or scabbing sore that heals and recurs. Unfortunately, there is a tendency to regard BCC as nonmalignant because the tumor rarely metastasizes. BCC advances by direct extension and destroys normal tissue. Left untreated or inadequately treated, the cancer can destroy the whole side of the face or penetrate subcutaneous tissue into the bone and brain.
Basal Cell Carcinoma versus Squamous Cell Carcinoma.
BCC and squamous cell carcinoma (SCC) are referred to as nonmelanoma skin cancers. A number of differences between these two tumors exist ( Table 21.1 ). The relationship with ultraviolet (UV) radiation is stronger for SCC. SCCs of the head and neck occur on areas receiving maximal irradiation. The distribution of BCC on the face does not correspond well with areas of maximal sun exposure. Many BCCs occur on sun-protected sites, such as the inner canthus and behind the ears. Approximately one third of all BCCs occur on areas of the skin that receive little or no UV radiation and, unlike SCCs, they are uncommon on the backs of the hands and on the forearms. Increasing grade of wrinkling is associated with a progressive reduction in risk of a BCC.
| Basal Cell Carcinoma | Squamous Cell Carcinoma | |
|---|---|---|
| Incidence in United States, 2012 | 542,782 | 186,157 to 419,843 |
| Age | 20% occur in patients younger than 50 years | Uncommon in the young |
| Fair skin, inability to tan | Low risk | High risk |
| Most important risk factor | Inability to tan | Cumulative sun exposure; increasing age more important than tanning ability |
| UV exposure patterns | Intermittent sun exposure, childhood and adolescent sun exposure, tanning beds | Cumulative exposure; childhood and adolescent sun exposure, tanning beds |
| Other environmental exposures | PUVA, arsenic (superficial multicentric BCC), photosensitizing drugs (tetracyclines, thiazide diuretics), ionizing radiation Immunosuppressed states (especially with solid organ transplantation and HIV) | Chronic ulceration and inflammation, scarring dermatosis, immunosuppressed states (especially solid organ transplantation, HIV and long term glucocorticoid use), human papillomavirus infection, chemical carcinogens (coal-tar products), psoralens and UVA, arsenic, cigarette smoking, photosensitizing drugs (tetracyclines, thiazide diuretics), ionizing radiation, voriconazole, BRAF inhibitors, radon |
| Genodermatoses | Xeroderma pigmentosum, nevoid BCC syndrome, epidermolysis bullosa (Dowling–Meara variant), nevus sebaceous | Xeroderma pigmentosum, epidermodysplasia verruciformis, epidermolysis bullosa (recessive dystrophic EB), Fanconi’s anemia, Ferguson–Smith syndrome (multiple KAs), Werner syndrome, Bloom syndrome, Rothmund–Thomson syndrome, dyskeratosis congenita, albinism |
Location.
Of all BCCs, 85% appear on the head and neck region; 25% to 30% occur on the nose alone, the most common site. BCC is rarely found on the backs of the hands, although this site receives a significant amount of solar radiation. Tumors also occur in sites protected from the sun, such as the genitals and breasts. The location of the BCC and SCC is important for risk stratifications (see Table 27.3 ).
Epidemiology.
The average lifetime risk for Caucasians to develop BCC is 30%. BCC most commonly occurs in adults, especially in the elderly population. Individuals with fair skin, blonde or red hair, light eye color, poor tanning ability (skin type I), and sun-damaged skin are at greatest risk. The male-to-female ratio is 2 : 1. Women younger than 40 years of age outnumber men in this age group. The closer Caucasians live to the equator, the greater is their risk for developing BCC.
The main risk factor for the development of BCC is UV light exposure. UVB radiation (290 to 320 nm, sumburn rays) plays a greater role in BCC development than UVA radiation (320 to 400 nm, tanning rays). UVA and UVB damage DNA. Light exposure is not the only factor; 20% of BCCs arise on non–sun-exposed skin. Individuals with fair skin, blonde or red hair, and light-colored eyes (skin type I) who are susceptible to sunburn have the highest risk. This increases with intense, intermittent amount of sun exposure when compared to an equal dose of continuous exposure. The incidence in people with dark skin is much lower. The incidence of developing BCC in transplant patients is 10 to 100 times higher than that in the general population. There is a 10-fold increased risk of developing a subsequent BCC 3 years after the first diagnosis of BCC. BCC occurs at the site of previous trauma, such as scars, thermal burns, and injury. BCC develops years later at sites treated with ionizing radiation. The tumor appears 3 months to 7 or more years later at the site of a previous injury.
Pathophysiology
BCCs arise from basal keratinocytes of the epidermis and adnexal structures (e.g., hair follicles, eccrine sweat ducts). UVB radiation damages DNA and its repair system and alters the immune system. The principle molecular pathway involved in the initiation of BCC is the sonic hedgehog signaling pathway. Medications such as vismodegib, erismodegib, itraconazole, and imiquimod alter this pathway and may be utilized to treat certain BCCs. BCC grows by direct extension and appears to require the surrounding stroma to support its growth. The course of BCC is unpredictable. BCC can remain small for years with little tendency to grow, particularly in the elderly, or it may grow rapidly or proceed by successive spurts of extension of the tumor and partial regression.
Histologic Characteristics
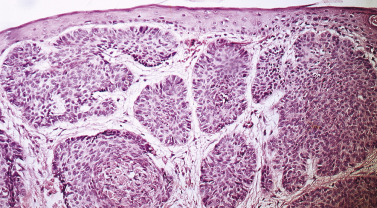
The cells of BCC resemble those of the basal layer of the epidermis. They are basophilic, have a large nucleus, and appear to form a basal layer by developing an orderly line around the periphery of tumor nests in the dermis, a feature referred to as palisading ( Fig. 21.1 ![]() ).
).
There are five major histologic patterns:
- 1.
Nodular (21%): a rounded mass of neoplastic cells with well-defined peripheral contours. Peripheral palisading is well developed (see Fig. 21.1 ).
- 2.
Superficial (17%): contains buds of atypical basal cells extending from the basal layer of the epidermis.
- 3.
Micronodular (15%): small, rounded nodules of tumor about the size of hair bulbs. Tumor islands are rounded and well demarcated, and demonstrate peripheral palisading.
- 4.
Infiltrative (7%): tumor islands vary in size and show a jagged configuration.
- 5.
Morpheaform (1%): numerous small, elongated islands containing a few cells that appear as strands or cords in a fibrous stroma.
Clinical Types
BCC occurs in many different clinical forms, which vary in appearance and malignant potential.
Nodular Basal Cell Carcinoma.
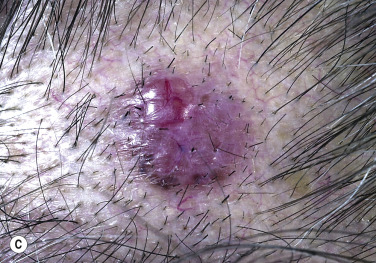
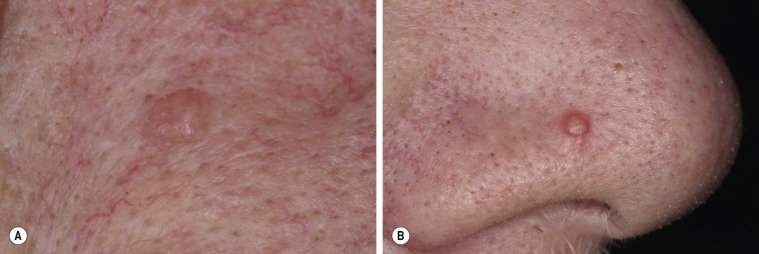
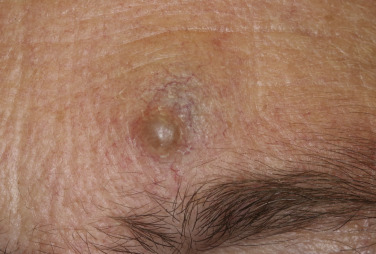
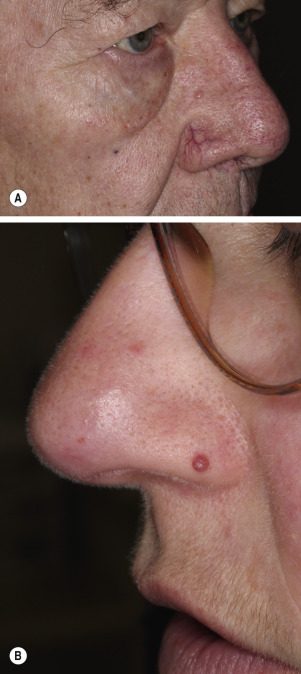
Nodular BCC is the most common form of BCC. The lesion begins as a pearly white or pink, dome-shaped papule resembling a molluscum contagiosum or dermal nevus ( Figs. 21.2 to 21.8 ![]() ). The mass extends peripherally. The lesion may remain flat. Traction on the surrounding skin accentuates the pearly border. Telangiectatic vessels become prominent and easily recognizable through the thin epidermis as the lesion enlarges. The growth pattern is irregular, forming an oval mass whereby the surface may become multilobular. The center frequently ulcerates and bleeds and subsequently accumulates crust and scale (see Fig. 21.5 ). Ulcerated BCCs were formerly termed rodent ulcers. Atypical fibroxanthomas can appear similar to BCC ( Fig. 21.9 ).
). The mass extends peripherally. The lesion may remain flat. Traction on the surrounding skin accentuates the pearly border. Telangiectatic vessels become prominent and easily recognizable through the thin epidermis as the lesion enlarges. The growth pattern is irregular, forming an oval mass whereby the surface may become multilobular. The center frequently ulcerates and bleeds and subsequently accumulates crust and scale (see Fig. 21.5 ). Ulcerated BCCs were formerly termed rodent ulcers. Atypical fibroxanthomas can appear similar to BCC ( Fig. 21.9 ).












Ulcerated areas heal with scarring, and patients often assume their conditions are improving. This cycle of growth, ulceration, and healing continues as the mass extends peripherally and deeper; masses of enormous size may be attained. BCCs may present as nonhealing leg ulcers. Biopsy specimens should be taken of leg ulcers that do not respond to treatment. The tissue mass of a nodular BCC has a distinctive consistency that can be appreciated during curettage or biopsy. It has poor cohesive forces and collapses or breaks down when manipulated with a curette. This is an important diagnostic feature that supports the clinical impression during the biopsy procedure.
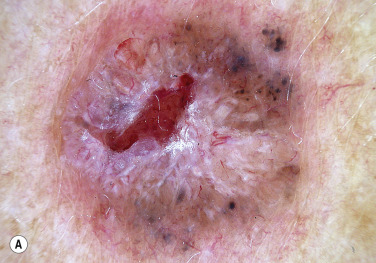
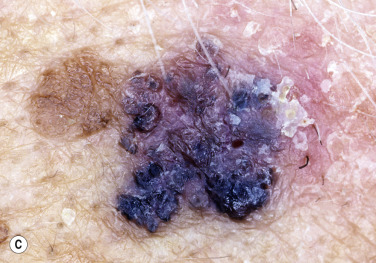
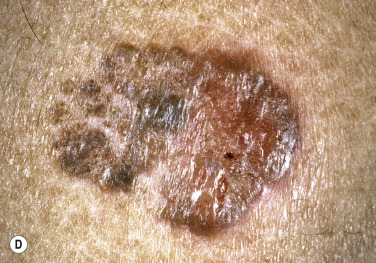
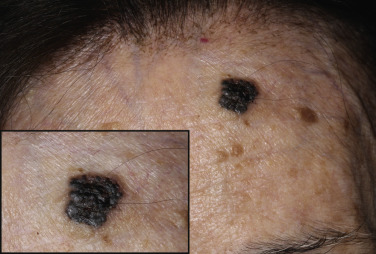
Pigmented Basal Cell Carcinoma.
BCCs may contain melanin that imparts a brown, black, or blue color through all or part of the lesion. Clinically, the lesion resembles a melanoma or pigmented seborrheic keratosis, but close inspection reveals the characteristically elevated, pearly white, translucent border ( Figs. 21.10 and 21.11 ). Surface microscopy (see Chapter 22 , Dermoscopy) may be used for more accurate diagnosis. Pigmented BCC must not have a pigment network and must have one or more of the following six positive features: large gray-blue ovoid nests, multiple gray-blue globules, maple leaf–like areas, spoke wheel areas, ulceration, and arborizing “tree-like” telangiectasia. A biopsy confirms the diagnosis. The histologic pattern most frequently associated with pigment is the nodular pattern.

Cystic Basal Cell Carcinoma.
This variant of nodular BCC appears as a smooth, round, cystic mass. Cystic BCC behaves like nodular BCC.
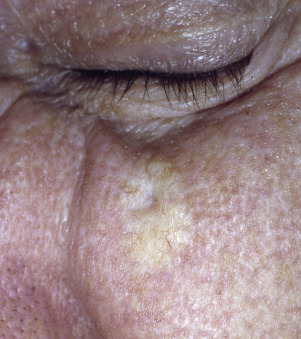
Sclerosing or Morpheaform Basal Cell Carcinoma.
Morpheaform BCC is an insidious tumor possessing innocuous surface characteristics that can mask its potential for deep, wide extension. The tumor is waxy, firm, flat-to-slightly raised, and either pale white or yellowish, and resembles localized scleroderma, thus the designation morpheaform ( Figs. 21.12 to 21.14 ![]() ). The borders are indistinct and blend with normal skin. Lesions may become depressed and firm, resembling a scar. The tissue is rigid and difficult or impossible to remove with a curette. Localization of this tumor by inspection or biopsy is impossible. The average subclinical extension beyond clinically delineated borders was 7.2 mm in one study . Treatment consists of wide excision or, preferably, Mohs micrographic surgery.
). The borders are indistinct and blend with normal skin. Lesions may become depressed and firm, resembling a scar. The tissue is rigid and difficult or impossible to remove with a curette. Localization of this tumor by inspection or biopsy is impossible. The average subclinical extension beyond clinically delineated borders was 7.2 mm in one study . Treatment consists of wide excision or, preferably, Mohs micrographic surgery.


Superficial Basal Cell Carcinoma
The least aggressive BCC is the superficial BCC. This tumor occurs most frequently on the trunk and extremities but may occur on the face. There may be one or more lesions. The tumor spreads peripherally, sometimes for several centimeters, and invades after considerable time. Slowly growing lesions may be present for years before patients seek help. The circumscribed, round-to-oval, red, scaling plaque resembles a plaque of eczema, psoriasis, extramammary Paget disease (EMPD), or Bowen disease ( Fig. 21.15 ). However, careful inspection of the border shows its thin, raised, pearly white nature. The characteristic features can also be appreciated by eliminating the redness with lateral finger pressure. Basal cell carcinoma is associated with inherited syndrome, most commonly basal cell nevus syndrome (BCNS).



Basal Cell Nevus Syndrome ((BCNS), Nevoid Basal Cell Carcinoma Syndrome, Gorlin Syndrome, Gorlin–Goltz Syndrome)
This rare dominantly inherited disorder with high penetrance (97%) and variable expressivity has a prevalence of 1 per 40,000 to 57,000 individuals. The disorder is diagnosed on the basis of clinical features with molecular confirmation if necessary ( Table 21.2 ). Patients with BCNS present to dermatologists with multiple BCCs (median number is 8; Figs. 21.16 and 21.17 ); usually BCCs arise at an early age (median age 20 years) and are histologically identical to sporadic BCC. Children may develop vascular-appearing BCCs (some are pedunculated around the neck) that look like melanocytic nevi. Patients, especially those with darker skin, may only develop a few BCCs over a lifetime. Sun-exposed and non–sun-exposed skin develops BCC. BCNS is caused by germline alterations in the PTCH ( PTCH1 , PTCH2 ) or SUFU genes involved in the sonic hedgehog pathway. Mutations in these genes allow for up-regulation of sonic hedgehog signaling and increase in cell growth and proliferation. Gene mutations do not correlate with the phenotypic expression, and genetic testing should be done in consultation with a geneticist or a genetic counselor. Mutations in SUFU are associated with an increased risk of medulloblastoma. BCNS patients should be followed closely by specialists familiar with this condition. BCNS patients should use meticulous ultraviolet radiation (UVR) precautions and avoid ionizing radiation (e.g., radiation for BCC, computerized tomography [CT] scans). Treatment of BCC is the same as for sporadic BCC, with the exception of avoiding radiation as a treatment option. Newer sonic hedgehog pathway inhibitors vismodegib and sonidegib may be administered systemically and topically for BCNS patients.
| MAJOR CRITERIA |
|
| MINOR CRITERIA |
|
| DIAGNOSIS |
|


Management and Risk of Recurrence
There are several factors to consider before choosing the best treatment modality. The most important are clinical presentation, cell type, tumor size, and location. Current guidelines follow the National Comprehensive Cancer Network guidelines ( Table 21.3 , Boxes 21.1 to 21.3 ).
| Parameters | Low Risk | High Risk |
|---|---|---|
| CLINICAL | ||
| Location * /size † | Area L <20 mm Area M ‡ <10 mm | Area L ≥20 mm Area M ≥10 mm Area H § |
| Borders | Well defined | Poorly defined |
| Primary vs recurrent | Primary | Recurrent |
| Immunosuppression | No | Yes |
| Site of prior radiation therapy | No | Yes |
| PATHOLOGIC | ||
| Growth pattern | Nodular, superficial ‖ | Aggressive ¶ |
| Perineural involvement | No | Yes |
* Area L consists of trunk and extremities (excluding hands, feet, nail units, pretibia, and ankles); area M consists of cheeks, forehead, scalp, neck, and pretibia; and area H consists of central face, eyelids, eyebrows, periorbital skin, nose, lips, chin, mandible, preauricular and postauricular skin/sulci, temple, ear, genitalia, hands, and feet.
‡ Location independent of size may constitute high risk.
§ Area H constitutes a high-risk area on the basis of location, independent of size.
‖ Other low-risk growth patterns include keratotic, infundibulocystic, and fibroepithelioma of Pinkus.
¶ Having morpheaform, basosquamous (metatypical), sclerosing, mixed infiltrative, or micronodular features in any portion of the tumor.
A treatment plan that considers recurrence rate, preservation of function, patient expectations, and potential adverse effects is recommended.
C&E may be considered for low-risk tumors in non-terminal hair-bearing locations.
For low-risk primary BCC, surgical excision with 4-mm clinical margins and histologic margin assessment is recommended.
Standard excision may be considered for select high-risk tumors. However, strong caution is advised when selecting a treatment modality without complete margin assessment for high-risk tumors.
Mohs micrographic surgery is recommended for high-risk BCC.
BCC, basal cell carcinoma; C&E, curettage and electrodesiccation.
Cryosurgery may be considered for low-risk BCC when more effective therapies are contraindicated or impractical.
If surgical therapy is not feasible or preferred, topical therapy (e.g., imiquimod or 5-FU), MAL- or ALA-PDT, and radiation therapy (e.g., superficial radiation therapy, brachytherapy, external electron beam, and other traditional radiotherapy forms for BCC) can be considered when tumors are low risk, with the understanding that the cure rate may be lower.
Adjustment of topical therapy dosing regimen on the basis of side-effect tolerance is recommended.
There is insufficient evidence to recommend the routine use of laser or electronic surface brachytherapy in the treatment of BCC.
ALA, aminolevulinic acid; BCC, basal cell carcinoma; 5-FU, 5-fluorouracil; MAL, methylaminolevulinate; PDT, photodynamic therapy.
Multidisciplinary consultation and smoothened inhibitors are recommended for patients with metastatic BCC.
If treatment of metastatic BCC with smoothened inhibitors is not feasible, platinum-based chemotherapy or best supportive care is recommended.
If surgery and radiation therapy are contraindicated or inappropriate for the treatment of locally advanced BCC, or if residual tumor persists following surgery and/or radiation therapy and further surgery and radiation therapy are contraindicated or inappropriate, systemic therapy with a smoothened inhibitor should be considered.
Patients with advanced disease should be provided with or referred for best supportive and palliative care, to optimize symptom management and maximize quality of life.
BCC, basal cell carcinoma.
Clinical Type.
Nodular and superficial BCCs are the least aggressive and many times can be treated by electrodesiccation and curettage or by simple surgical excision, if they are considered low risk for recurrence (see Table 21.3 ).
Histologic Type.
The micronodular, infiltrative, and morpheaform BCCs have a higher incidence of positive tumor margins (18.6%, 26.5%, and 33.3%, respectively) after excision and have the greatest recurrence rate. Clinically, BCCs with these patterns have poorly defined borders and are not apparent during physical examination. They subtly extend into surrounding tissue and are easily missed by blind treatment techniques such as surgical excision. An average of 7.2 mm of subclinical tumor extension was found in morpheaform BCCs in one study, compared with 2.1 mm of extension in well-circumscribed nodular lesions. Routine pathologic examination of surgically excised BCCs may not detect a small nodule or strand of BCC on the other side of the excision margin. These tumors are classified as high risk by National Comprehensive Cancer Network (NCCN) guidelines and need more aggressive treatment with wide excision or Mohs microscopically controlled surgery.
Tumor Size.
In general, electrodesiccation and curettage afford excellent results for smaller low-risk BCCs (see Table 21.3 ).
Location.
Tumors in the H regions (see Tables 21.3 and 27.3 ) are considered high risk and require Mohs micrographic surgery ( Box 21.4 ).
- 1.
Extensive, recurrent skin cancers that have not responded to aggressive conventional surgical techniques or radiation
- 2.
Unusually large primary skin cancers of long duration
- 3.
Poorly differentiated squamous cell carcinoma
- 4.
Morpheaform or fibrotic basal cell carcinoma
- 5.
Tumors with poorly demarcated clinical borders
- 6.
Tumors on the face in locations where deeper invasion of the skin along natural skin planes is possible or the extent of the tumor is difficult to define, such as eyelids, nasal alae, nasolabial folds, and circumauricular areas
- 7.
Areas where maximum conservation of tumor-free tissue is important for preservation of function, such as the penis or finger
Follow–up.
Box 21.5 summarizes the recommendations for follow-up of BCC.
After diagnosis of a first BCC, skin cancer screening for new keratinocyte cancers (BCC or cSCC) and for melanoma should be performed on at least an annual basis.
Patients with a history of BCC should be counseled on skin self-examination and sun protection.
The use of topical and oral retinoids (e.g., tretinoin, retinol, acitretin, and isotretinoin) is not recommended to reduce the incidence of future keratinocyte cancers in those with a history of BCC.
Dietary supplementation of selenium and beta-carotene is not recommended to reduce the incidence of future keratinocyte cancers in those with a history of BCC.
There is insufficient evidence to make a recommendation on the use of oral nicotinamide, DFMO, or celecoxib in the chemoprevention of BCC.
BCC, basal cell carcinoma; DFMO, α-difluoromethylornithine; cSCC, cutaneous squamous cell carcinoma.
Bichakjian C, Alam M. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol 2018;78(3):540–59. Table XIII.
Recurrent Basal Cell Carcinoma
Clinical Presentation
Inadequately treated BCC may recur. The tumor may be superficial in the scar tissue, on the border, or deep in the dermis or subcutaneous fat ( Fig. 21.18 ). The clinical presentation of recurrent BCC sometimes differs from that of the original tumor. A tumor that infiltrates scar tissue produces a subtle change in color and consistency that is easily missed. Erosions that appear spontaneously at the border or in the scar are suspicious. The characteristic pearly white border is often absent, but biopsy of the erosion with the curette can reveal the soft, amorphous, gelatinous tissue of BCC extending deep and laterally well beyond the border of the erosion. Deep recurrences show a normal or a brownish erythematous surface and can be confused with epidermal cysts.


Histologic picture, anatomic location, and size are factors in predicting recurrence.
Histologic Type.
Tumors of the morpheaform and basosquamous varieties have the greatest recurrence rate. BCCs that histologically show poor palisading or have a micronodular (islands of tumor) and/or infiltrating strand pattern without sclerotic stroma clinically have poorly defined borders and are not apparent during physical examination. They subtly extend into surrounding tissue and are easily missed by blind treatment techniques such as surgical excision. An average of 7.2 mm of subclinical tumor extension was found in morpheaform BCCs in one study, compared with 2.1 mm of extension in well-circumscribed nodular lesions. As mentioned previously, routine pathologic examination of surgically excised BCCs may not detect a small nodule or strand of BCC on the other side of the excision margin. These tumors need more aggressive treatment with wide excision or microscopically controlled surgery.
Location.
Increasing diameter of the lesion and location of the lesion on various sites of the head, especially the nose and ear, are associated with an increased risk of recurrence, whereas location on the neck, trunk, limbs, or genitalia is associated with a decreased risk of recurrence with electrodesiccation and curettage, radiation therapy, and surgical excision. BCCs on the nose or perinasal area may infiltrate along the perichondrium or penetrate into the embryonic fusion plane of the nasolabial fold, resulting in subclinical extension.
Size.
The larger the tumor, the greater the chance of recurrence; increased subclinical extension is seen with larger tumors.
Treatment of Basal Cell Carcinoma
The following section outlines various treatment modalities. Specific surgical techniques are described in Chapter 27 .
Biopsy.
Biopsy alone of a small BCC often appears curative with no clinical evidence of residual tumor. Two thirds of clinically disease-free biopsy sites were shown to contain microscopic foci of BCC.
Electrodesiccation and Curettage.
Curettage and destruction is indicated for low-risk BCC (see Table 21.3 ).
Curettage requires firm dermis on all sides and below the tumor to enable the curette to distinguish between dermis and soft tumor ( Fig. 21.19 ![]() ). If the tumor encroaches on the fat, the curette cannot distinguish between fat and soft tumor, and an alternate procedure must be used. Curettage should be avoided for lesions on the back and shoulders, where the dermis is thick, unless the BCCs are superficial and small. Proper technique requires vigorous curettage, usually two to three times; therefore lesions on the eyelid or lip area are treated by other methods. It is especially useful for lower extremity tumors, where tissue mobilization for excision may be difficult. Wounds created by electrosurgery ooze serum and accumulate crust during a 2- to 6-week healing period. The recurrence rate using electrodesiccation and curettage performed by a fully trained dermatologist is 5.7%. The overall recurrence rate using surgical excision is 5.3%. The technique is explained in Chapter 27 .
). If the tumor encroaches on the fat, the curette cannot distinguish between fat and soft tumor, and an alternate procedure must be used. Curettage should be avoided for lesions on the back and shoulders, where the dermis is thick, unless the BCCs are superficial and small. Proper technique requires vigorous curettage, usually two to three times; therefore lesions on the eyelid or lip area are treated by other methods. It is especially useful for lower extremity tumors, where tissue mobilization for excision may be difficult. Wounds created by electrosurgery ooze serum and accumulate crust during a 2- to 6-week healing period. The recurrence rate using electrodesiccation and curettage performed by a fully trained dermatologist is 5.7%. The overall recurrence rate using surgical excision is 5.3%. The technique is explained in Chapter 27 .

Cryosurgery.
Cryosurgery utilizing liquid nitrogen may be considered for low-risk BCC in which other therapies are not indicated or are not practical. For example, cryotherapy is an excellent option for a frail elderly patient with multiple superficial BCCs on the back.
Excision Surgery.
For low-risk BCC, standard surgical excision with 4-mm margins to the depth of the mid-subcutis results in a 96% 5-year cure rate.
Incompletely Resected Basal Cell Carcinoma.
Adequate excision, peripherally and in depth, is the key to surgical control, and the demonstration of tumor cells at the margins of excision is associated with recurrence rates of 26.8%. Data support the policy of immediate reexcision or Mohs micrographic surgery for all patients with incompletely excised BCCs rather than a “wait-and-see” policy after incomplete excision. Reexcision may not be necessary if the patient’s life span is limited or if treatment of a possible recurrence would not be difficult.
Mohs Micrographic Surgery.
Mohs surgery is a microscopically controlled technique that should be utilized for high-risk BCC (see Table 21.3 ). This technique is reviewed in Chapter 27 .
Radiation.
Radiation, such as external beam radiation, may be utilized for patients who are not able to undergo surgical excision.
Imiquimod 5% Cream.
Imiquimod is an immune response modifier that induces cytokines related to cell-mediated immune responses including interferon-alfa, interferon-gamma, and interleukin-12. Patient-administered imiquimod 5% cream used five to seven times per week for a period of 6 weeks effectively treated superficial BCCs ( Fig. 21.20 ![]() ). Local skin reactions are common but well tolerated. The initial clearance rate at 12 weeks’ posttreatment is about 95%. The recurrence rate after 2 years is as high as 20%.
). Local skin reactions are common but well tolerated. The initial clearance rate at 12 weeks’ posttreatment is about 95%. The recurrence rate after 2 years is as high as 20%.

5-Fluorouracil.
Five percent 5-fluorouracil (5-FU) cream is approved by the Food and Drug Administration (FDA) for the treatment of superficial BCCs. Treat with 5% 5-FU cream twice daily for up to 12 weeks. Treatment is stopped sooner if the lesion is clinically resolved.
Metastatic Basal Cell Carcinoma.
Basal cell carcinoma rarely metastasizes and has an extremely poor prognosis. Treatments are summarized in Box 21.3 and should involve multiple specialties. Newer medications targeting the sonic hedgehog pathway have been developed.
Vismodegib and Sonidegib.
Vismodegib and Sonidegib are orally administered sonic hedgehog–pathway inhibitors that are effective for treating locally advanced and metastatic BCCs. Advanced BCCs are defined as inoperable because of multiple postsurgical recurrences, incurable with surgery without significant deformity or loss of function, or metastatic. Many patients stop the drugs because of adverse events, which include loss of taste, muscle cramps, hair loss, and weight loss.
Recommended Follow-Up Evaluation.
Box 21.5 summarizes follow-up recommendations and risk reduction for future BCC.
Actinic Keratosis
Actinic keratosis (AK) is a scaly papule due to epidermal keratinocyte dysplasia, resulting from UVR. Actinic keratosis may spontaneously resolve, remain stable for years, or progress to SCC and possibly BCC.
The potential for change cannot be predicted by clinical signs or histologic characteristics. Thick lesions are worrisome. Patients with AKs need periodic evaluation and usually repetitive treatments to prevent the development of aggressive cancers. Individuals with light complexions are more susceptible than those with dark complexions. Years of sun exposure are required to induce sufficient damage to cause lesions. Actinic keratoses may undergo spontaneous remission if sunlight exposure is reduced, but new lesions may appear. Patients often present with lesions that were first noticed during the summer, suggesting that the lesions may become more active after sunlight exposure. Immunosuppression is a risk factor. SCC is up to 65 times as likely to develop in transplant patients as controls. Lesions appear 2 to 4 years after transplantation and increase in frequency.
Clinical Presentation.
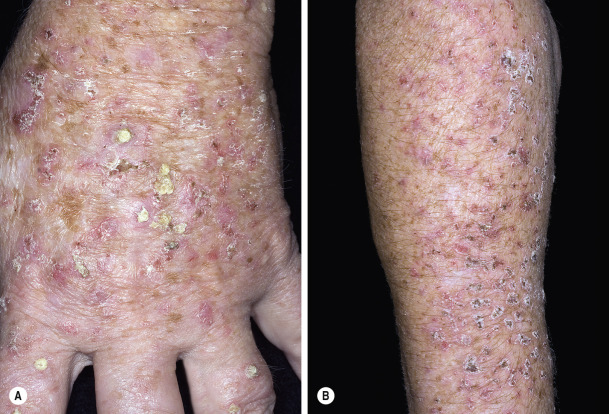
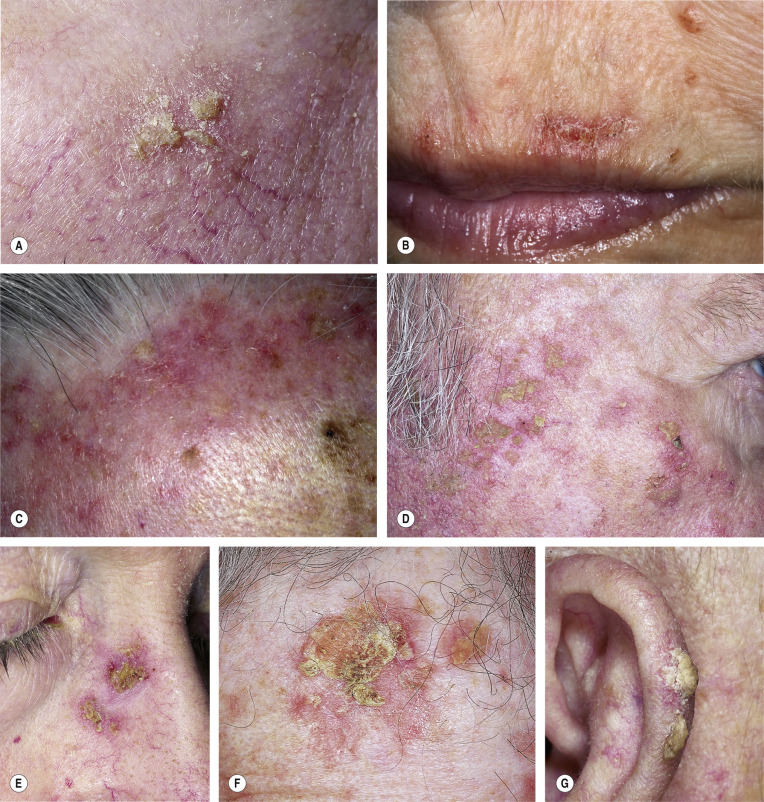
Actinic keratoses begin as an area of increased vascularity, with the skin surface becoming slightly rough. Texture is the key to diagnosing early lesions. They are better recognized by palpation than by inspection. Very gradually an adherent, yellow, sharp scale forms. Removal of the scale may cause bleeding ( Figs. 21.21 and 21.22 ). Most lesions vary in size from 3 to 6 mm. The extent of disease varies from a single lesion to involvement of the entire forehead, balding scalp, or temples. AK can progress into thickened or hypertrophic lesions. Thickened lesions can progress to SCC and be clinically indistinguishable. Induration, inflammation, and oozing suggest degeneration into malignancy.
Clinical and Histologic Variants.
Variants include spreading pigmented AK, cutaneous horn, actinic cheilitis, and others ( Table 21.4 ![]() ). Pigmented AKs resemble a scaling lentigo, seborrheic keratosis, or melanoma ( Fig. 21.23 ). They are the result of a collision between a nonpigmented solar keratosis and a separate coexistent pigmented lesion, primarily a solar lentigo. Pigmented AKs can be associated with adjacent melanoma in situ; therefore, its diagnosis merits increased suspicion for coexisting melanoma. Cutaneous horn is a hypertrophic AK that accumulates keratin to become a conical hyperkeratotic protuberance ( Fig. 21.24 ).
). Pigmented AKs resemble a scaling lentigo, seborrheic keratosis, or melanoma ( Fig. 21.23 ). They are the result of a collision between a nonpigmented solar keratosis and a separate coexistent pigmented lesion, primarily a solar lentigo. Pigmented AKs can be associated with adjacent melanoma in situ; therefore, its diagnosis merits increased suspicion for coexisting melanoma. Cutaneous horn is a hypertrophic AK that accumulates keratin to become a conical hyperkeratotic protuberance ( Fig. 21.24 ).

| Variant | Characteristics | |
|---|---|---|
| 1 | Hypertrophic |
|
| 2 | Atrophic |
|
| 3 | Bowenoid |
|
| 4 | Acantholytic |
|
| 5 | Epidermolytic |
|
| 6 | Lichenoid |
|
| 7 | Pigmented |
|
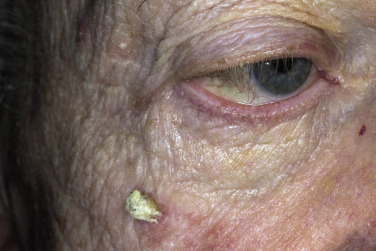
AKs are very common and tend to be thick on the scalp ( Fig. 21.25 ). Actinic cheilitis is AK occurring on the lower lips. The lips are rough, scaly, and red, and may show fissuring, scaliness, and ulcerations. These findings can be seen in SCCs of the lip ( Figs. 21.26 and 21.27 ). SCCs of the lip have approximately an 11% metastatic rate, which is higher than other cutaneous SCCs.



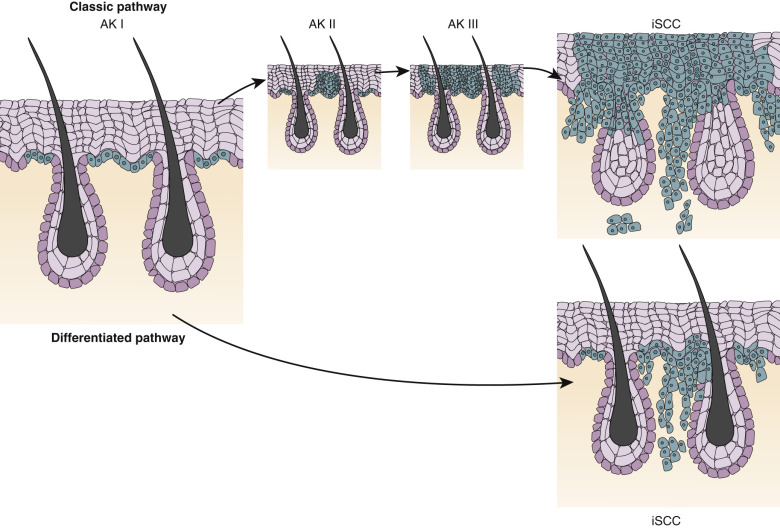
Transformation Into Squamous Cell Carcinoma.
After several years, a small percentage of lesions may increase in size and thickness, extend into the dermis, and become a risk for metastatic disease. A very low yearly transformation rate for single lesions can translate into a substantial lifetime risk of transformation for patients with several actinic keratoses. Squamous cell carcinomas that evolve from AK, may eventually metastasize. Malignant transformation may occur as a progression from atypical keratinocytes in the lower third of the epidermis to full thickness involvement (similar to the progression of cervical cancer) or a cancerous cell may arise directly from an atypical epidermal cell and invade along hair follicles and sweat ducts ( Fig. 21.28 ). Risk factors associated with malignant progression included induration/inflammation, diameter greater than 1 cm, history of rapid enlargement, bleeding, erythema, and ulceration. Retrospective analysis of 91 invasive SCCs at the site of a previously confirmed AK determined that the length of time to progression was 24.6 months. Lesions located on the lips and ears are at elevated risk for disease progression. AKs of the trunk and lower extremities also have a high risk of progression and poor healing. Factors associated with increased risk of invasive SCC arising from AK are listed in Box 21.6 ![]() .
.
Lesion Characteristics
Hyperkeratotic, proliferative
Inflamed, bleeding
Large surface area and depth
Ulceration, induration
Pigmentation
Any rapid changes in presentation
Presence of multiple lesions
Evidence of greater ultraviolet-induced skin damage
Lesion Location
Lip, ear, extremities
Concomitant Medications, Illness
Immunosuppressive agents
Agents that increase sun sensitivity
Lymphoma, leukemia
Actinic Keratosis versus Squamous Cell Carcinoma.
There is no definite way to distinguish between an AK and an SCC without a biopsy. There is a continuum of clinical signs that makes distinction difficult. An increase in the thickness, redness, pain, ulceration, and size only suggests progression to SCC, but it is impossible to predict the point at which an individual AK will evolve into an invasive SCC. Lesions thought to be actinic keratoses or those not responding to treatment may actually be SCCs. Therefore treatment should be aggressive and patients monitored closely to prevent progression.
Pathophysiology and Histology.
Ultraviolet radiation initiates the process by inducing mutations in DNA. Additional exposure to radiation may convert the AK into an SCC. Histologically, an AK consists of abnormal epithelial cells confined to the epidermis. The features of the cells are identical to those found in invasive SCC, including those that have metastasized. The cells have large pleomorphic nuclei and acidophilic cytoplasm. Some are in mitosis. They show signs of faulty cornification with dyskeratotic cells and parakeratosis. The follicles are not involved, so there is no follicular plugging. Penetration through the dermoepidermal junction and into the dermis indicates the development of an invasive SCC.
Management
Because actinic keratoses sometimes undergo spontaneous remission, definitive treatment may be delayed for patients with a few superficial lesions. Small lesions should be reexamined at a later date for spontaneous remission. Patients should make every effort to prevent further sun damage. This does not mean that patients must hibernate for a lifetime, but they should understand techniques to reduce sunlight exposure. There is a continuum and a progression from AK to SCC; therefore there is no way to reliably distinguish clinically between the two diagnoses. Because it can be impossible to distinguish between an AK and an SCC, treatment of AK should be aggressive to stop the progression to SCC. All patients with AK should be examined carefully for BCCs.
Treatment Approaches
There are two approaches: lesion-directed therapy and field-directed therapy ( Table 21.5 ).
| Treatment Type | Treatment | Local Adverse Effects | Systemic Adverse Effects | Notes |
|---|---|---|---|---|
| Lesion-directed therapy | Liquid nitrogen cryotherapy | Short term: pain, edema, blistering, infection, pyogenic granuloma (rare) Long term: nerve damage, pigment changes | NA | NA |
| CO 2 laser resurfacing | Persistent erythema, dyspigmentation, infections, scarring | NA | NA | |
| Curettage | Scar, infection, vital structure damage (rare) | Reactivation and local spread of HSV | Works well for hyperkeratotic lesions | |
| Dermabrasion | Intense pain | NA | Used for large areas such as scalp or forehead; usually requires procedural sedation and analgesia | |
| Topical field treatment | 5-FU | Erythema, inflammation, erosions, pain, pruritus, photosensitivity, burning | Headache, insomnia, irritability, stomatitis, leukocytosis, thrombocytopenia, birth defects, herpes simplex reactivation, miscarriage, neutropenia, neurotoxicity, gastrointestinal toxicity | Systemic toxicity mostly seen in patients with dihydropyrimidine dehydrogenase deficiency; not recommended in patients with melasma or acne rosacea |
| Imiquimod | Erythema | Upper respiratory tract infection, influenza-like symptoms, HSV | NA | |
| Ingenol mebutate | Pain, itching, irritation, infection, dose-related erythema, flaking/scaling/dryness, scabbing/crusting | Headache, periorbital edema, nasopharyngitis, conjunctivitis, eye pain, herpes zoster, severe hypersensitivity (rare) | FDA warning about systemic adverse effects was issued in August 2015 | |
| Diclofenac | Dry skin, pruritus, erythema | Hepatotoxicity (rare) | NA | |
| Lesion-directed or field therapy | Photodynamic therapy | Burning or stinging during light exposure, pigmentary changes | NA | FDA approved for lesion-directed treatment but is used off label as field therapy |
Lesion-Directed Therapy
These techniques are indicated for isolated lesions that are few in number.
Cryotherapy.
Cryotherapy is the treatment of choice for most isolated, superficial, AK. AK resides in the epithelium. Cryotherapy with liquid nitrogen causes the separation of the epidermis and dermis, resulting in a highly specific, nonscarring method of therapy for superficial lesions. It is tempting to freeze thicker lesions but malignant cells that reside at an increased depth may be missed by this technique. Patients with darker complexions may develop hypopigmented areas after freezing, and treating multiple lesions on the faces of such patients may result in white-spotted faces. Topical 5-FU is the best alternative.
Curettage With Electrodesiccation.
Curettage with electrodesiccation is indicated and highly effective for thick hypertrophic lesions. Lesions heal with a hypopigmented scar. Clinicians are often surprised at how deep these seemingly thin isolated hyperkeratotic lesions can be and are gratified that they chose this technique instead of cryotherapy.
Surgical Removal.
Individual indurated lesions or those with thick crusts should be removed with minor surgical procedures such as curettage shave excisions. It is unnecessary to biopsy lesions less than 0.5 cm. Larger lesions or those occurring near or on the vermilion border of the lips should be examined. Electrodesiccation and curettage easily remove small, thicker lesions. The CO 2 laser may be superior to vermilionectomy for actinic cheilitis that is too extensive to be treated with topical 5-FU.
Field-Directed Therapy
Field-directed therapy is indicated for multiple visible lesions on contiguous areas of sun damage that are likely to contain many subclinical lesions. These forms of therapy treat both active and preclinical lesions. This approach includes resurfacing techniques (dermabrasion, chemical peels, and laser therapy), topically applied medications, and photodynamic therapy. These techniques cause erythema, dryness, pruritus, and burning. Treatment duration varies. It is shortest for ingenol mebutate gel, 2 to 4 weeks for 5-FU, and variable for imiquimod, depending on medication concentration (two 2-week cycles or up to 16 weeks). Skin reactions may persist for up to 4 weeks after treatment is stopped. An initial increase in lesion counts occurs as the inflammatory process reveals and treats subclinical lesions.
Topical Chemotherapy With 5-Fluorouracil.
5-FU is an effective topical treatment for superficial AK. Thicker lesions, especially those on the scalp, may evolve into SCC and should be treated with more aggressive techniques. The agent is incorporated into rapidly dividing cells, resulting in cell death. Normal cells are less affected and clinically appear to be unaffected. Inflammation is induced during this process. Thick, indurated lesions become most inflamed and may best be managed by surgically removing them before instituting topical chemotherapy. The available preparations of 5-FU are listed in Table 21.6 ![]() and in the Formulary.
and in the Formulary.
| Product | Active Ingredient | Packaging |
|---|---|---|
| Carac | 0.5% fluorouracil | 30-g cream |
| Efudex | 2% fluorouracil | 10-mL liquid |
| 5% fluorouracil | 10-mL liquid | |
| 5% fluorouracil | 25-g cream | |
| Fluoroplex | 1% fluorouracil | 30-mL solution |
| 1% fluorouracil | 30-g cream | |
| Aldara | 5% imiquimod | Cream – box of 12 or 24 packets |
| Zyclara | 2.5%, 3.75% imiquimod | Cream – box of 28 packets, 7.5- and 15-g pump bottle |
Patients should be cautioned about the various stages of inflammation encountered during treatment. Considerable discomfort may be experienced for 1 week or more during periods of intense inflammation. Pain can be minimized if only small areas are treated at one time; however, many patients wish to treat the full face instead of prolonging the unsightly erythema and crusting for weeks. Lesions on the back of the hands, arms, and lower legs require longer periods of treatment than those on the face ( Table 21.7 ). Patients with a small number of lesions may be treated during the summer or winter. Patients with a large number of lesions who work outdoors are best treated in the winter. Pharmaceutical companies that manufacture 5-FU supply patient information sheets and videos with color photographs of the various stages of inflammation.
| Site | Early Signs of Inflammation (Days) | Duration of Treatment (Weeks) |
|---|---|---|
| Face, lips | 3–5 | 2–4 |
| Scalp | 4–7 | 3–5 |
| Neck | 4–7 | 2–4 |
| Arms, hands, legs | 10–14 | 4–8 |
| Back | 10–14 | 4–6 |
| Chest | 10–14 | 4–6 |
Treatment Technique (5-FU) and Expected Results
5-FU is available as a 0.5%, 1%, and 5% cream and a 1% and 2% solution. The 1% solution is helpful for the scalp with hair, and the 2% solution is used for individual lesions. 5-FU 0.5% cream is applied once daily for up to 4 weeks as tolerated. Irritation resolves within 2 weeks of cessation of treatment. 5-FU 5% cream is applied twice a day for 2 to 4 weeks. Applying 5-FU preparations two or three times a week is less effective. Significant irritation and discomfort are frequently encountered. Petrolatum may be applied between 5-FU applications to soothe raw, dry, and cracked areas. Oral pain medication (e.g., acetaminophen with codeine) controls pain at the peak of inflammation. Instruction handouts supplied by 5-FU manufacturers are very helpful.
Topical Chemotherapy With Imiquimod.
Imiquimod cream (5%, 3.75%, 2.5%) is an immune response modifier. Imiquimod 5% applied three times a week for 16 weeks resulted in an 86.6% reduction in AK. An alternate treatment regimen for the 5% preparation is to apply the medication three times a week for 4 weeks followed by a 4-week no-treatment interval, and then by a second 4-week treatment cycle. In the event of a local skin reaction, treatment may be reduced to two times per week. Imiquimod 2.5% and 3.75% creams are administered daily as a 2-week on/off/on regimen (see Table 21.6 ![]() ). Lesion reduction is greater with imiquimod 3.75% than with imiquimod 2.5%.
). Lesion reduction is greater with imiquimod 3.75% than with imiquimod 2.5%.
Inflammatory Response and Physician Supervision.
In the early inflammatory phase, erythema first appears in treated areas at predictable intervals (see Table 21.7 ). In the severe inflammatory phase ( Fig. 21.29 ), erythema, edema, burning, stinging, and oozing reach maximum intensity at different intervals, depending on the site treated and the thickness of the lesions. In the lesion disintegration phase, erosion or ulceration, intense inflammation, discomfort, pain, crusting, eschar formation, and evidence of reepithelialization occur. When this phase is reached, treatment stops. Table 21.7 lists the approximate duration of treatment. Patients should be evaluated every 1 or 2 weeks during the treatment period. This irritating treatment is a major event for the patient. They are physically and mentally traumatized, and they will have many questions. Patients need close supervision, encouragement, and reassurance. They frequently call the office during treatment. The clinician must determine the endpoint of treatment and be prepared to manage excessive inflammation with wet compresses and group V to VI topical steroids. Infection responds to mupirocin ointment or oral antibiotics. Sunscreens can be irritating and should not be used during treatment. Sun exposure is avoided by using hats and clothing. Women may tolerate bland liquid makeup.



Ingenol Mebutate.
Ingenol mebutate is extracted from the sap of the plant Euphorbia peplus . The sap of this plant has been used as a naturopathic remedy for actinic lesions by Australians with AK. It causes rapid cell death of tumor cells, which are more sensitive to ingenol mebutate than are differentiated keratinocytes. Ingenol mebutate gel is FDA-approved for topical treatment of AK. In human studies, ingenol mebutate achieved high clearance rates of AK on the trunk or extremities and face or scalp after once-daily application for 2 or 3 consecutive daily treatments. The localized inflammatory skin responses were generally mild to moderate and resolved in approximately 2 weeks on the face or scalp and in 4 weeks on the trunk or extremities. Gel containing ingenol mebutate is available in two formulations – 0.015% or 0.05%. Ingenol mebutate gel may be applied to the affected area, up to one contiguous skin area of approximately 25 cm 2 (e.g., 5 cm × 5 cm), using one unit-dose tube. After the gel is spread evenly over the treatment area, it should be allowed to dry for 15 minutes. Wash hands after application and avoid transfer to other areas including the eye.
Avoid washing and touching the treated area for 6 hours after application. Actinic keratoses on the face and scalp are treated by applying ingenol mebutate gel 0.015% to the affected area once daily for 3 consecutive days. Actinic keratoses on the trunk and extremities are treated by applying ingenol mebutate gel 0.05% to the affected area once daily for 2 consecutive days. Prescribe a treatment kit. The face and scalp kit (0.015%) contains three tubes. The trunk and extremity kit (0.05%) contains two to three tubes. One tube is used each day. The most common adverse reactions (≥2%) are application site pain, pruritus, irritation, infection, periorbital edema, nasopharyngitis, and headache. There have been reports of severe allergic reactions (e.g., swelling of tongue and throat, and difficulty breathing), herpes zoster, and severe eye injury (from transfer of gel to eye) after use of ingenol mebutate.
Other Treatments.
Diclofenac, dermabrasion, and CO 2 laser resurfacing are other treatments that have been utilized to treat AK (see Table 21.5 ).
Photodynamic Therapy.
Photodynamic therapy is a two-step procedure. A precursor photosensitizing agent is applied and absorbed by damaged cells. It undergoes enzymatic conversion to a photosensitizer. Several hours later the area is illuminated with blue or red visible light. This leads to production of singlet oxygen that initiates a tissue-toxic photochemical reaction. Acute pain during illumination is a major side effect. Crusts and erosions form in a few days. Imiquimod provides a better clinical response and a significantly better histologic response than photodynamic therapy.
Topical Steroids.
Some authors suggest using topical steroids during the entire treatment period to suppress inflammation and decrease patient discomfort. This technique, however, may make it difficult to determine when therapy should be discontinued.
Actinic Keratosis of the Face.
Patients with mild damage consisting of erythema and scaling can be treated with tretinoin cream 0.05% alone for several months. Small, superficial lesions that do not respond can then be treated with 5-FU or cryosurgery. Patients with many lesions can be pretreated with tretinoin cream applied once each day for 1 to 3 months. Pretreatment with tretinoin may improve the quality of the dermis and reduce subsequent treatment time with 5-FU. Tretinoin 0.025% cream should be prescribed for patients with sensitive skin. 5-FU may then be applied alone or in combination with tretinoin to complete the treatment program. Combination therapy may shorten the treatment period, but it produces more intense inflammation. Most clinicians prescribe 5-FU alone without the use of tretinoin.
Actinic Keratoses of the Upper and Lower Extremities.
These lesions are frequently multiple, hyperkeratotic, and distributed over a large area. Hyperkeratosis tends to limit penetration of topical 5-FU. Lesions on the extremities require longer treatment than those on the face. Lesions may be pretreated for 1 or 2 weeks or longer with twice daily applications of tretinoin 0.025% gel or 12% ammonium lactate to reduce hyperkeratosis, which interferes with 5-FU penetration. Plastic wrap occlusion is sometimes used to facilitate 5-FU penetration of thicker lesions.
Actinic Cheilitis.
Actinic cheilitis is treated effectively with 5-FU cream ( Fig. 21.30 ![]() ); however, pain and excessive crusting can make this a very unpleasant experience. Some authors suggest using 5% 5-FU cream three times a day for 14 to 18 days to obtain the optimal reaction in the shortest time. The objective is to reduce the morbidity to 2 weeks. Application of 5% lidocaine ointment relieves pain.
); however, pain and excessive crusting can make this a very unpleasant experience. Some authors suggest using 5% 5-FU cream three times a day for 14 to 18 days to obtain the optimal reaction in the shortest time. The objective is to reduce the morbidity to 2 weeks. Application of 5% lidocaine ointment relieves pain.

Cool compresses are applied several times each day if inflammation is intense. Group V topical steroids may be applied to red areas to suppress inflammation and pruritus. The appearance of a purulent exudate suggests infection; when this occurs, oral antistaphylococcal antibiotics or mupirocin ointment should be prescribed. In the healing phase, residual erythema and hyperpigmentation persist for several weeks.
Contact Allergy to 5-FU.
Contact allergy to 5-FU should be suspected if intense erythema and vesiculation occur. Patch testing is not reliable because many patients who are allergic to 5-FU do not show a positive patch test reaction.
Prognosis.
Patients should remain free of lesions for months and possibly years, but recurrences can be anticipated. Frequently, unsupervised patients inadequately treat their own newly evolving lesions, resulting in surface healing but untreated deeper abnormal cells. For this reason, no refills should be indicated on the initial prescription, and patients should be instructed to discard medication when treatment is finished.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


