Posterior Thigh and Hamstring Flaps for Ischial Ulcers
John Hulsen
Jeffrey E. Janis
DEFINITION
A pressure injury is localized damage to the skin and soft tissue typically over a bony prominence.
They occur as a result of prolonged pressure or pressure in combination with shear.
The ischial area is the most frequent site of development and recurrence of pressure ulcers.2
Soft tissue overlying the bony prominence of the ischial tuberosity is particularly vulnerable to pressure injury especially in the wheelchair-bound/spinal cord injury patient.
ANATOMY
The posterior thigh is a region bordered by the inferior gluteal fold superiorly, the iliotibial tract laterally, the thigh adductors medially, and the popliteal fossa inferiorly.
The hamstring muscle group functions to flex, stabilize, and rotate the knee and are not expendable as a group in the ambulatory patient (FIG 1).3
Biceps femoris
Semimembranosus
Semitendinosus
Blood supply of the posterior thigh skin:
The profunda femoris artery principally supplies the largest cutaneous area on the posterior thigh.3
It originates laterally from the femoral artery, gives off both medial and lateral circumflex femoral arteries, and then continues distally and traveling behind the adductor longus.
Medial branches enter into the adductor compartment.
Lateral branches (four profunda femoris artery perforating vessels) pierce the adductor magnus insertion and enter the posterior compartment of the thigh.
The fourth profunda femoris perforating artery is the termination of the profunda femoris artery.
Each profunda femoris perforating vessel perfuses musculocutaneous and/or septocutaneous perforators that contribute to the well-developed fascial plexus of the posterior thigh.
The inferior gluteal artery principally supplies the cutaneous vascular territory of the lower gluteal region.
It originates off the internal iliac artery and exits the pelvis to enter the gluteal region inferior to the piriformis with the sciatic and posterior cutaneous nerves. In 91% of patients, the inferior gluteal artery sends off a descending fasciocutaneous branch.4
The descending branch of the inferior gluteal artery travels in a common sheath with the posterior cutaneous nerve in 72% of patients.
Rather than singularly coursing down the thigh, the descending branch acts as a “relay artery,” being reinforced along its length by myocutaneous and fasciocutaneous branches from the profunda femoris perforating vessels.3
Anastomotic branches from the descending branch of the inferior gluteal artery join branches from the medial femoral circumflex artery, lateral femoral circumflex artery, and the first profunda perforating artery to form the cruciate anastomosis (FIG 2).5
Each vessel that unites to form the cruciate anastomosis can provide collateral circulation to the longitudinally directed fascial plexus of the posterior thigh in the absence (or surgical ligation) of one of its constituents.3,5
This accounts for the clinical reliability of the multitude of fasciocutaneous flap designs available from the posterior thigh.
PATHOGENESIS
Pressure ulcers are the result of numerous factors, both extrinsic and intrinsic to the patient, that contribute to the development of a wound.
Pressure: Greatest areas found over bony prominences
Can produce tissue ischemia if applied in excess of 32 mm Hg (skin end capillary bed pressure)
The ischial tuberosities are particularly vulnerable to ulceration and recurrence as pressures over this region in the sitting position exceed 80 to 100 mm Hg.
Shearing: Sliding deformation of tissue caused by oppositely directed parallel forces
Friction: Contributes to abrasions and breakdown of the superficial skin barrier
Moisture: Contributes to maceration of the skin
Limited mobility: Inability to adequately off-load pressure points, potentially increasing friction and shearing forces
Altered sensation: Lack of protective sensory input
Spasticity: Interruption of supraspinal inhibitory pathways that may result in contractures that create new or altered pressure points
Altered level of consciousness: Unrecognized prolonged pressure with skin maceration/contamination from urine/fecal soilage
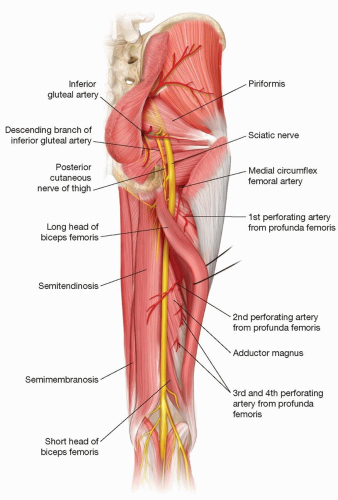
FIG 1 • Key posterior thigh anatomy.
Tissue tolerance for pressure and shear forces is affected by microclimate, nutrition, perfusion, comorbidities, and condition of the soft tissue.1
It is important to recognize, especially in the spinal cord injury patient, that all phases of wound healing are impaired in denervated tissue.
NATURAL HISTORY
Skin hyperemia is seen within 30 minutes and is characterized by nonblanching erythema that resolves within 1 hour after pressure is alleviated.
Tissue ischemia develops with sufficient continuous pressure for 2 to 6 hours, causing erythema that requires at least 36 hours to resolve after pressure cessation.
Deep tissue injury/tissue necrosis can develop after 6 hours of unrelieved pressure and manifests as deep red, maroon, or purple skin discoloration with induration.
Soft tissue ulceration over bony prominences occurs within 2 weeks after tissue necrosis occurs.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient age, general health/functional status, medical comorbidities, nutritional intake, as well as the circumstances, etiology, chronology, and prior ulcer management should be documented.
Note any medications or therapy that impairs wound healing such as radiation and steroids.
Obtain reports from any previous surgical interventions that may influence ulcer reconstructive options.
Social history including tobacco use and a clear picture of the patient’s support system should be obtained.
It is critical to identify the etiology that led to reconstructive failure when treating a recurrent ulcer.
Lack of compliance with postoperative care, lack of patient motivation, and inadequate resources for home care will doom even the best executed reconstruction and are critical to account for in determining whether a patient is a reconstructive candidate.
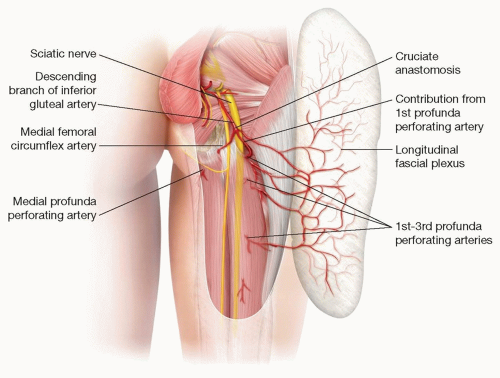
FIG 2 • The cruciate anastomosis.
Physical examination
General appearance, BMI, assessment of nutrition status: Does the patient appear well or fragile and emaciated?
Accurately assess location, dimensions (including tunneling), wound condition/odor, and stage/depth of ulcer.
Presence of diverting ostomy or suprapubic catheter
Presence of lower extremity fixed posturing or uncontrolled spasticity
Evaluate the posterior trunk and lower extremities for surgical scars from previous reconstructions while also assessing potential donor-site muscle bulk (diminished in spinal cord injury).
IMAGING AND OTHER DIAGNOSTIC STUDIES
Preoperative laboratory studies
White blood cell count/differential and hemoglobin/hematocrit
Inflammatory markers: Erythrocyte sedimentation rate and C-reactive protein (especially if suspect osteomyelitis)
Glucose and HgbA1c: Ideally, good long-term glucose control in diabetics with a HgbA1c less than 6%6
Nutrition studies
Accurate assessment of the nutritional status of the pressure ulcer patient is often compromised by proinflammatory factors that may preclude the use of typical serum protein values.
Ideal, and potentially unattainable, preoperative serum protein levels7:
Albumin: At least 3.5 g/dL with upward trend
Prealbumin: At least 20 g/dL with upward trend
Unfortunately, there is little evidence that enteral or parenteral nutrition supplementation has any effect on healing existing pressure sores or the prevention of new ulcers.
Data suggest that anemia, serum protein alterations, and markers of inflammation will actually normalize after surgical treatment of the ulcer.8
These deficient values are viewed as the result of the ulcer rather than modifiable risk factors to optimize prior to surgery.
Imaging studies
Used to assess for any undrained fluid collection and as noninvasive modality to detect osteomyelitis
MRI: 97% sensitive, 89% specific for diagnosis of osteomyelitis in the pelvis9
Pathology/microbiology
Diagnostic standard for osteomyelitis is the pathology report of an aseptically obtained bone biopsy.
DIFFERENTIAL DIAGNOSIS
Stage I to IV pressure ulcer, unstageable wound, or deep tissue injury
Wound infection
Acute or chronic osteomyelitis
Malnutrition
Muscle spasms
Fecal and/or urinary incontinence
Failed previous reconstruction
NONOPERATIVE MANAGEMENT
Indications for nonoperative management include patients with stage I and II pressure ulcers as well as some patients with stage III and IV ulcers who are not candidates for reconstruction7:
Unmotivated patient
Inadequate home support or outpatient care
Comorbidities that place the patient at an unacceptable surgical or anesthesia risk
Unreconstructable defect
In all pressure ulcer cases particular emphasis is placed on the prevention of wound complications and infections, halting ulcer progression, and reducing the risk of additional ulcers.
If possible, the highest goal is a closed stable wound.
A closed wound is not an attainable goal for all patients.
The patient’s social situation is just as important, if not more so, than any medical or surgical therapy.7
General treatment strategies for nonoperative management mirror those used in preoperative optimization of the pressure ulcer surgical candidate.
Offloading pressure points with specialty beds, seat mapping, and turning protocols every 2 hours.
Local skin and wound care to promote moist wound healing without maceration is essential.
Many passive and sophisticated active dressings are available; however, evidence is mixed regarding head-to-head superiority.
Fever/sepsis usually has a urinary or pulmonary source, not the open wound.
Negative-pressure wound therapy may be more comfortable to patients and effective in ulcers that fail to progress or as a bridge to surgery.
NPWT functions to increase wound perfusion and formation of granulation tissue while reducing bacterial load
A well-balanced diet is best to provide adequate nutrition for wound healing.
Supplements are beneficial only if there is a nutritional deficiency.10
Goal is 30 to 35 kcal/kg and 1.25 to 1.5 g protein/kg/d for adults with a pressure ulcer who are at risk for malnutrition.
Additional fluid should be provided to patients with heavily exudative wounds to prevent dehydration.
Management of muscular spasms helps to prevent new pressure points and reduces wound-shearing forces.
SURGICAL MANAGEMENT
The presence of stage III and IV pressure ulcers alone is not an indication for surgical management.7
Optimization of medical comorbidities, modification of risk factors, assuring adequate home support, availability of medical equipment, access to outpatient care, assessment of patient compliance, and motivation to take an active role in self-care are essential for consideration of surgical candidacy.
The technical intraoperative aspects of pressure ulcer surgery are often the easiest facet of the patient’s care.
Goals of surgical management7:Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree