patterns support the association with somatic mosaicism, which was described by Happle and Assim in 2001.8 PWBs do not follow the lines of Blaschko but rather are mostly localized or segmental in distribution. Multifocal and widespread PWBs do occur but are less common.
TABLE 3.2.1 Vascular Anomalies per the 2014 ISSVA Classification | ||
|---|---|---|
|
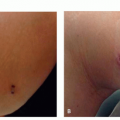
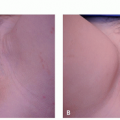
 FIGURE 3.2.1 Hypertrophic and nodular port-wine birthmark. |
as demonstrated by the lack of mitoses and of tritiated thymidine uptake. A mean vessel depth of 0.46 mm has been reported for CMs, suggesting that most of the vessels are superficial. Immunohistochemical studies reveal a significantly decreased density of perivascular nervous tissue in lesional skin associated with progressive vascular dilatation.14 On confocal microscopy, nerve density and blood vessel diameter are inversely correlated with the lowest nerve density exhibiting the highest blood vessel density and the poorest response to laser intervention.15 The expression of endothelial cell mitogen vascular endothelial growth factor (VEGF)-A and of its receptor VEGF-R2 are significantly increased in CM tissue as compared with control skin.16
TABLE 3.2.2 Syndromic Associations and Characteristics | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
small CMs on the face and limbs, with about 30% of individuals with concomitant arteriovenous malformations (AVMs) and/or AVFs,20 which are generally symptomatic early in life.
Vascular tumors
Other vascular malformations
Telangiectasia
Cutis marmorata telangiectatica congenita (CMTC)
Nevus simplex/salmon patch/“stork bite”/“angel kiss”
Lymphatic malformations (LMs)
Venous malformations (VMs)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


