PATIENT HISTORY AND PHYSICAL FINDINGS
■ A thorough history should be elicited prior to treatment, including a detailed past medical and surgical history, present medications and allergies, and a personal and family history of cancer. A complete head-to-toe skin examination should be performed. All lymph node basins (cervical, supraclavicular, axillary, epitrochlear, inguinal, popliteal) should be evaluated for clinically positive lymph nodes.
■ Clinically positive lymph nodes typically present as a palpable mass. However, enlarged lymph nodes in the popliteal fossa may not be easily palpable because of the thick overlying fascia. Therefore, a careful examination of the popliteal fossa is essential.
■ Most patients undergo popliteal dissection because of a positive sentinel lymph node biopsy. Sentinel lymph node biopsy has now become the standard of care for evaluating regional lymph node basins in patients with cutaneous melanoma greater than 1 mm in Breslow thickness who have no evidence of distant metastatic disease (see Chapter 27). Current standard of care for patients with positive sentinel lymph nodes includes completion lymphadenectomy of the involved lymph node basin; observation alone should be performed in the context of a clinical trial. Approximately 50% of patients with a positive popliteal sentinel lymph node biopsy will also have documented inguinal disease; therefore, popliteal and inguinal dissections are often performed concomitantly.1,2
IMAGING AND OTHER DIAGNOSTIC STUDIES
■ A clinically positive lymph node should be evaluated using fine needle aspiration biopsy. Popliteal dissection is performed for a positive biopsy.
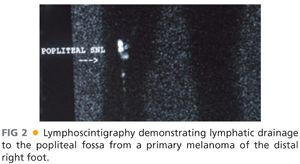
■ For patients with clinically negative lymph nodes, preoperative lymphoscintigraphy should be performed at the time of the initial sentinel lymph node biopsy even if the primary melanoma is located on an extremity. Lymphoscintigraphy will demonstrate drainage to popliteal lymph nodes in 1% to 9% of patients with distal lower extremity melanoma (i.e., below the knee; FIG 2).1–5 By far, the most common locations for primary melanomas that drain to the popliteal fossa are the posterolateral foot and posterior lower leg; however, primary melanomas of the anterior lower leg or anteromedial aspect of the foot will also occasionally drain to the popliteal fossa.1–4 The overall incidence of a positive popliteal lymph node is 0.3% to 2.8%.1–3,5
SURGICAL MANAGEMENT
Preoperative Planning
■ In the preoperative area, a focused history and physical examination should be repeated, and the patient’s prior pathology and imaging studies should be reviewed.
■ The patient should be marked to confirm laterality.
■ Although there are no data that specifically address the wound infection rate in popliteal dissection, we favor the administration of a dose of preoperative antibiotics, particularly if concomitant inguinal dissection is planned.
Positioning
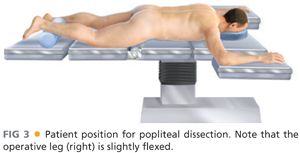
■ The patient is placed prone, with pressure points padded, and the operative knee slightly flexed (FIG 3). The operative leg should be prepped circumferentially from above the midthigh to below the midcalf.
■ If a concomitant inguinal dissection is planned, the popliteal dissection is usually performed first.
TECHNIQUES
PLACEMENT OF INCISION
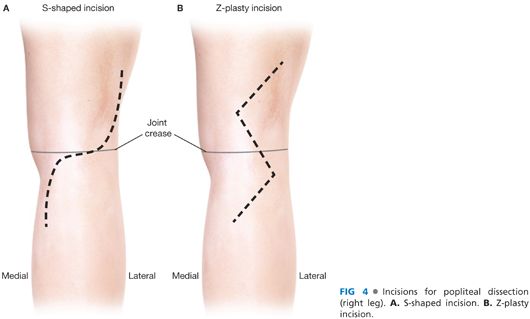
■ There are two options for the incision for popliteal dissection (FIG 4). The incision should be planned such that a prior incision for sentinel lymph node biopsy can be excised.
■ The S-shaped incision was described by Karakousis6 in his initial report of the technique of popliteal dissection. This incision typically extends from approximately 10 cm proximal to the joint crease along the lateral thigh overlying the biceps femoris muscle, crosses the joint transversely, and extends approximately 10 cm distal to the joint crease along the medial calf overlying the medial aspect of the gastrocnemius muscle (FIG 4A). A mirror image of this incision, extending from the medial thigh to the lateral calf, is also acceptable and may be preferable depending on the orientation of the incision used to perform the sentinel lymph node biopsy.
■ We prefer a Z-plasty incision that allows for optimal exposure and heals without joint contracture.7 Again, the orientation is typically superolateral to inferomedial. The width and length of the Z is relative to the size of the lower thigh, usually with an interior angle ranging from 100 to 120 degrees (FIG 4B).
SKIN INCISION AND RAISING OF FLAPS
■
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


