Perioperative pain management in surgery of the hand and upper extremity relies on a multimodal approach involving systemic, local, and presurgical considerations. A pain management plan should be tailored to each patient. Management of pain of patients undergoing upper extremity surgery begins before surgical intervention and continues postoperatively. Patient education, setting expectations, psychological interventions, and addressing risk factors associated with postoperative pain are critical to successful pain management. Intraoperative anesthesia is accomplished via a variety of means. Cryotherapy, transcutaneous electrical nerve stimulation, acupuncture, massage, and localized heat are used in concert with pharmacologic therapies postoperatively to continue pain management.
Key points
- •
A multimodal analgesia approach including oral and intravenous therapies is the most effective means of managing perioperative pain of patients undergoing surgery of the hand and upper extremity.
- •
Regional anesthesia for upper extremity surgery is effective for procedures involving distinct anatomic regions and is augmented with continuous infusions to reduce postoperative pain and opioid requirements.
- •
Preoperative pain science education and pain management education can decrease postoperative opioid use and increase patient satisfaction.
Introduction
Outpatient surgeries have become increasingly popular over the past few decades, in line with the significant advances in surgical techniques, improving technology, availability of more efficient anesthetic medications, and evolving pain management strategies. In 2010, there were an estimated 48.3 million ambulatory surgery procedures performed in the United States, which is estimated to keep rising with the current shift away from inpatient surgery to improve efficiency and reduce cost.
Hand and upper extremity surgeries are among the most common procedures performed in an outpatient setting, and patients are commonly prescribed opioid medications for postoperative pain management. Approximately one-third of patients complain of moderate to severe pain after surgery and adequate pain management allows patients to progress more comfortably and efficiently through rehabilitation and to improve patient satisfaction and surgical outcomes. Additionally, postoperative pain complaints are the most common causes for unanticipated inpatient admissions, and severe acute postoperative pain is associated with the development of chronic pain and frequent visits to the outpatient clinic and emergency department. Persistent pain in elderly patients has been associated with cognitive decline, increased risk for dementia, memory loss, and loss of executive function. Given these known associations stemming from postoperative pain and the potential effect on patients’ quality of life, surgeons should be thoughtful in their perioperative pain management practices.
There are several strategies implemented to offer patients proper pain control, which is most efficiently achieved by a multimodal approach. Pain management starts in the preoperative setting with patient education, establishing proper expectations, psychosocial therapies, and addressing opioid medication habits especially in opioid-tolerant patients. Intraoperative analgesia and anesthesia usually set the tone for the postoperative pain management phase and includes peripheral regional blocks, intravenous (IV) regional anesthesia (RA), continuous infusion pumps, periarticular infiltration, local infiltration, and wide-awake surgery. Postoperative analgesia starts in the postanesthesia care unit including cryotherapy, injectable and oral medications, transdermal patches, and selective regional blocks. Home analgesia involves multiple different medications with different efficiencies and modes of action, such as acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxers, gabapentinoids, ketorolac, and opioids.
Opioid pharmacotherapy has long been the mainstay for postoperative pain control following surgeries of the hand and upper extremity, but in the face of the opioid epidemic there has been a great deal of attention directed at ways to reduce opioid prescriptions and reduce the rates of substance-related deaths in the United States. The annual opioid-related economic burden is $78.5 billion, and this is mostly because of health care cost, treatment of substance abuse and dependence, and lost productivity and incarceration.
The Centers for Disease Control and Prevention has reported more than 400,000 opioid-related deaths from 1999 to 2017, and the numbers keep rising. There were around 48,000 deaths in 2017 alone related to opioid overdose including prescription and illegal drugs, a staggering 130 mortalities per day, six times higher than in 1999. There are increasing efforts to finding alternative ways to provide proper pain management for all patients, especially orthopedic surgery patients, the third highest recipients of opioid prescriptions in all medical and surgical specialties.
This review discusses the different pain management modalities used in surgeries of the hand and upper extremity, describing the mode of action of each modality, the effectiveness of each pain management option, and the risks and potential complications.
Pain pathways and modulation
The pain pathway is broken down into two different categories: the central and peripheral nervous systems (CNS and PNS). Each system has several modulators, which are the targets of perioperative pain control. Therefore, a basic understanding of the pain pathway is helpful in understanding and providing effective perioperative pain management.
Surgery is a trauma that stimulates nociceptors in the PNS. The resulting inflammatory reaction at the site of injury initiates a cascade of locally released inflammatory mediators, among which are cyclooxygenase (COX) and prostaglandins, the targets of acetaminophen, NSAIDs, and other common perioperative medications. Inflammatory mediators sensitize nociceptors, decreasing their excitability threshold.
Nociceptors carry signals to the dorsal horn of the spinal cord, part of the CNS, where inhibitory neuronal pathways can modulate pain. Psychological factors can play a role in these inhibitory neuronal pathways, with the signal ultimately carried to the brain where sensations are perceived. Neurons in the CNS, in the brain and spinal cord, have excitatory and inhibitory receptors, including the N -methyl- d -aspartate (NMDA) receptors and α 2 -adrenergic receptors, respectively, which can be targeted by pharmacotherapy. In response to inflammation and nociceptor stimulation, expression of receptors and channels on neurons in the CNS undergo modulation (reversible changes) and modification (long-lasting changes) of these neurons. , These changes result in short-lived or long-lasting changes in excitability, changes that are the basis of hyperalgesia, chronic pain, and pathologic pain. , ,
Pharmacotherapy and multimodal analgesia
Inhibition of Inflammation and Prostaglandins
Prostaglandins are found in the pain pathway in the PNS and CNS, inflammatory mediators that sensitize nociceptors in the setting of injury. Therefore, modulation of the inflammatory pathway is an important target for postoperative pain control. Acetaminophen and ibuprofen reduce inflammation and prostaglandin production.
Acetaminophen (Tylenol) is the most widely used medication in multimodal therapy with its low side-effect profile and minimal contraindications compared with other medications. Acetaminophen given 24 hours before surgery has been shown to reduce morphine intake by up to 20%. Hepatotoxicity is a side effect of acetaminophen that should be considered, especially in patients with cirrhosis of the liver or liver injury.
NSAIDs exert their effects either through nonselective inhibition of the COX-1 and -2 enzymes (ketorolac, ibuprofen, meloxicam), or selective COX-2 inhibition (celecoxib). Preoperative and postoperative NSAIDs including ketorolac (Toradol), ibuprofen, and celecoxib, have all been shown to significantly reduce postoperative pain. , , These have increased anti-inflammatory properties when compared with acetaminophen alone. The side effects of NSAIDs (gastric irritation, cardiovascular events, and renal toxicity) must be considered in each patient individually to ensure safety. Selective COX-2 inhibitors are considered for their reduced gastrointestinal and renal risk profile. A theoretic risk of bone healing problems is associated with NSAID use, but evidence to this effect has not been strong enough to preclude its use in this setting.
Gabapentinoids
Gabapentinoids, such as gabapentin and pregabalin, are associated with reduced opioid requirements, reduced postoperative pain, , and decreased risk of progression to chronic pain by mitigating central and peripheral sensitization. Both medications are effective when dosed preoperatively and exert their effects by blocking voltage-dependent calcium channels and modulating excitatory neurotransmitter release , thereby reducing hypersensitivity in spinal cord dorsal horn neurons. There has been no consensus on recommended perioperative dosing; studies have recommended anywhere from a 2-week preoperative course to a high-dose bolus 1 to 2 hours before surgery, to simply starting a course of gabapentinoids postoperatively. Caution should be used in patients with contraindications, such as renal dysfunction, or those with higher risk of sedation and dizziness because these are side effects of gabapentinoids.
N -Methyl- d -Aspartate Receptor Antagonists
Ketamine is well-known for its action as an NDMA receptor antagonist, with a complex mechanism of action, acting peripherally and centrally on multiple other binding sites including nicotinic, muscarinic, monoaminergic, and opioid receptors. Ketamine also decreases proinflammatory cytokine formation. Intraoperative ketamine has been shown to decrease central pain sensitization, opioid requirements postoperatively, and persistent postoperative pain , at subanesthetic doses. Risks of administration including hallucinations and nightmares have become less frequent with modern reduced doses of ketamine used perioperatively. Still, the American Pain Society recommends that ketamine be used for major surgeries given its known side effects.
IV and intra-articular magnesium and nitric oxide have NMDA receptor antagonistic effects and have been considered for use to control postoperative pain, although none of these have received a significant amount of attention in the literature.
Other Nonopioid Pain Medications
α 2 -Adrenergic receptor agonists, such as dexmedetomidine and clonidine, have shown promising effects on decreasing perioperative pain and hyperalgesia , , by acting centrally and increasing the effects of inhibitory γ-aminobutyric acid neurons. Intraoperative corticosteroids have also demonstrated decreased postoperative pain and opioid consumption, with prolonged RA.
Lidocaine, typically known for its action on sodium channels providing local anesthesia, also demonstrates action on other familiar receptors within the pain pathway. IV lidocaine has been shown to have anti-inflammatory properties and central NMDA receptor antagonism. IV lidocaine has demonstrated decreased postoperative pain scores and opioid consumption. ,
Opioids
Opioids mimic endogenous opioid proteins and bind to mu, delta, and kappa receptors thereby reducing neuronal excitability and decreasing the release of the nociceptive neurotransmitter, substance P. Oral opioids have been shown to be equally effective for postoperative pain control as IV. The cautions of opioid medication include addiction potential; nausea; vomiting; ileus; constipation; urinary retention; sleep disturbance; delirium; and, most significantly, sedation, respiratory depression; and tolerance. , Opioids have been shown to cause opioid-induced hypersensitivity, a paradox in which opioids lead to increased pain perception. Some opioids activate NMDA receptors, activating central excitatory neurons, leading to increased perceptions of pain. Short-acting opioids, such as fentanyl, used intraoperatively have been shown to be clinically associated with higher opioid requirements postoperatively after the infusion had been stopped.
Multimodal Analgesia
Multimodal pain therapy takes advantage of the science behind pain perception by targeting different receptors involved in modulation of pain perception. Studies have demonstrated that, compared with narcotic-only management, multimodal therapy provides as effective or superior pain management, in addition to reducing the amount of opioids used. , , Additionally, enhanced recovery protocols have been developed on the idea that reducing metabolic stress with multimodal therapy leads not only to improved pain management but also to decreased catabolism and perioperative insulin resistance, thereby reducing poor surgical outcomes. Multimodal therapy is an especially important concept to use when operating on patients with risk factors associated with increased postoperative pain. These risk factors include preoperative opioid use/substance abuse, morbid obesity, anxiety and depression, younger patients, female patients, preexisting pain syndromes, and lower education. , ,
Preventative and preemptive pain management are other important considerations in perioperative pain management in terms of medication timing. The role of preventative analgesia is reducing CNS sensitization, and improving postoperative pain control. Preemptive analgesia (eg, local/regional anesthetic before the incision) aims to mitigate the afferent nociceptive pathway, the first step in pain perception. Although preemptive analgesia helps with immediate postoperative pain control, it has not consistently been shown to be as effective as preventative analgesia in reducing surgery-related opioid use. ,
There is a paucity of publications regarding multimodal therapy in upper extremity surgery specifically, but there is evidence that upper extremity surgeons have room to improve routine multimodal analgesia practices. In a study evaluating 170 shoulder surgeons, more than 90% reported that they had a pain management regimen, but less than 50% regularly gave acetaminophen or ibuprofen, less than 15% regularly gave gabapentin, and more than 75% gave short-acting narcotics. There is also evidence of overprescribing opioids up to five times what patients consume, in orthopedic literature. In one study of 1199 procedures including shoulder arthroscopy, endoscopic carpal tunnel release, hip, and total knee surgeries, patients reported unused opioids in 61% of procedures. Even after one institution used an early recovery protocol, the rate of opioid prescriptions was still 72% for patients with low opioid consumption before discharge and low pain scores. Increased mindfulness regarding opioid requirements can mitigate this discrepancy. Kim and colleagues documented the number of opioid pills patients consumed among several upper extremity surgeries, and created a helpful template ( Table 1 ).
| Operation | Typical Volume of 1% Lidocaine with 1:100,000 Epinephrine and 8.4% Bicarbonate (Mixed 10 mL:1 mL) | Location of Injection |
|---|---|---|
| Carpal tunnel | 20 mL | 10 mL between ulnar and median nerves (5 mm proximal to wrist crease and 5 mm ulnar to median nerve); another 10 mL under incision |
| Trigger finger | 4 mL | Subcutaneously beneath the center of the incision |
| Finger sensory block (SIMPLE) | 2 mL | Volar middle of proximal phalanx just past palmar-finger crease |
| Finger soft tissue lesions or other surgery when finger base tourniquet is not desirable and finger epinephrine is used for hemostasis | 5 mL volar distributed among 3 phalanges, 4 mL dorsal split between 2 phalanges | 2 mL volar and 2 mL dorsal subcutaneous midline fat, in proximal and middle phalanges The distal phalanx gets only 1 mL midline volar, just past the DIP crease |
| PIP arthrodesis | 8 mL total, 4 mL volar (2 in each phalanx), and 4 mL dorsal (2 in each phalanx) | 2 mL midvolar and another 2 mL middorsal of proximal and middle phalanges |
| Thumb MCP arthrodesis and collateral ligament tears of the MCP joint | 15 mL | 2 mL on each of volar and dorsal aspects of proximal phalanx and the rest all around the metacarpal head |
| Dupuytren contracture or zone II flexor tendon repair | 15 mL/ray | 10 mL (or more) in the palm, then 2 mL in the proximal and middle phalanges and 1 mL in the distal phalanx (if required) |
| Trapeziectomy or Bennet fracture | 40 mL | Radial side of the hand under the skin and all around the joint, including the median nerve If LRTI is performed, decrease concentration to 0.5% lidocaine with 1:200,000 epinephrine, and also inject all around where FCR or APL will be dissected |
| Metacarpal fractures | 40 mL | All around the metacarpal where dissection or K-wires will occur |
Regional anesthesia
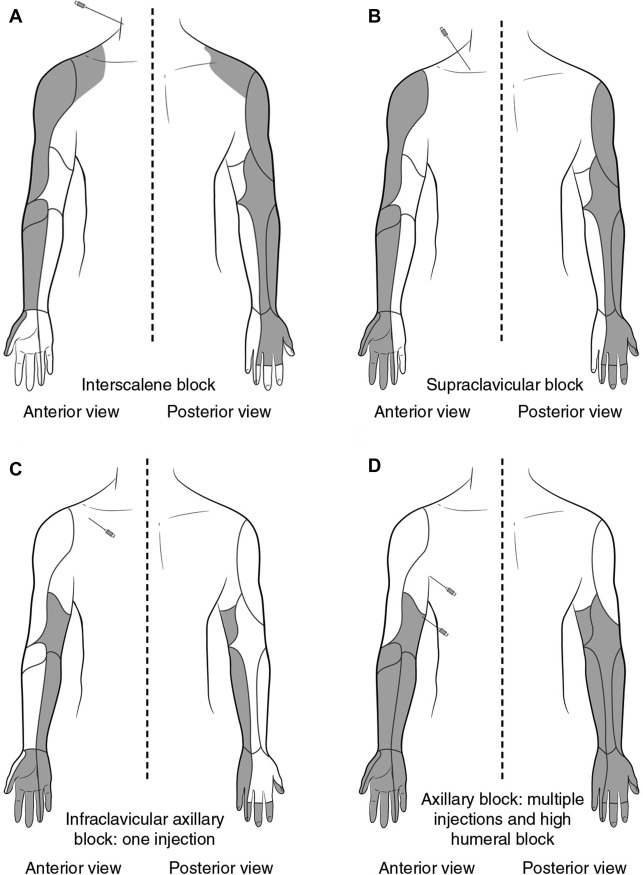
RA is a means of achieving a combination of motor and sensory blockade via targeted administration of anesthetic agents and adjuvants into a specific anatomic region. In upper extremity surgery, RA is often a peripheral block of the brachial plexus, which can be anesthetized in various anatomic regions to achieve the desired anesthetic effect. Commonly, RA of the brachial plexus is aimed at the interscalene, supraclavicular, infraclavicular, or axillary regions ( Fig. 1 ). The advent of ultrasound and neurostimulation as a means of localizing these regions has increased the adoption, safety, and efficacy of RA as an alternative to general anesthesia. Long- and short-acting local agents for RA are available and the dose required is dependent on agent used, technique (eg, ultrasound guided), and physician preference. Bupivacaine is a long-acting agent that has been shown effective for interscalene brachial plexus blocks (ISB). Its association with cardiotoxicity and neurotoxicity led to the development of levobupivacaine and ropivacaine, which have been shown to have improved side effect profiles. Adjuvants to RA including epinephrine, clonidine, and dexamethasone are used to improve local absorption and prolong duration of analgesia; however, those benefits must be weighed against their known associations with intraoperative bradycardia, hypotension, and sedation.