Abstract
Mastering the fundamental techniques of periocular surgery is essential for the Mohs and reconstructive surgeon. The eye holds immeasurable value, visual and aesthetic, that demand understanding and expertise to ensure successful surgical outcomes. The mobile nature of the eyelids and their bipolar suspension creates tensional forces that must be appreciated and actively managed during surgical repairs. Numerous surgical techniques have been described throughout the decades. In this chapter, fundamental principles and select reconstructive techniques that reliably produce optimal results and minimize complications are presented.
Keywords
eye, ocular, periocular, surgery, reconstruction
Introduction
Mastering the fundamental techniques of periocular surgery is essential for the Mohs and reconstructive surgeon. The eye holds immeasurable value, visual and aesthetic, that demand understanding and expertise to ensure successful surgical outcomes. The mobile nature of the eyelids and their bipolar suspension creates tensional forces that must be appreciated and actively managed during surgical repairs. Numerous surgical techniques have been described throughout the decades. In this chapter, fundamental principles and select reconstructive techniques that reliably produce optimal results and minimize complications are presented.
Preoperative Assessment
For most patients, a preoperative examination assessing visual acuity, intraocular pressure, and tear film/dryness is generally recommended within a year before surgery. Consultation with an oculoplastic surgeon is prudent for patients with preexisting eye disease and defects close to involving the lid margin. Imaging with computed tomography or magnetic resonance imaging may be indicated for tumors in the medial canthus and complex tumors that may extend into the orbit. Management or cessation of blood-thinning medications is indicated for tumor extirpations or repairs that extend into the orbital septum to minimize risks of retrobulbar hemorrhage. Meticulous intraoperative control of bleeding and postoperative observation and counseling are essential. Assessment and control of blood pressure in hypertensive patients is also important to minimize risks of bleeding. In addition, anxiolytic medications with adequate monitoring can be useful during periocular surgery.
Specialized Instrumentation
Although many periocular repairs can be performed with standard facial repair trays, specialized instrumentation can be useful, particularly for defects involving the lid margins.
Specialized instrumentation for periocular surgical trays:
Corneal shields protect the globe and shield the light
Bishop-Harmon forceps for handling delicate tissue
Spring scissors for accurate cutting of fine tissues
Tenotomy scissors for cutting tarsus
Castroviejo needle drivers for grasping and placing fine sutures
Fine tissue hooks
Beaver blade and blade holders
Bipolar unit for hemostasis in a wet field
5-0 and 6-0 polyglactin sutures spatulated needles
6-0 polypropylene sutures
Proparacaine ophthalmic drops
Erythromycin ophthalmic ointment
Nonstick eye pads
Anatomy
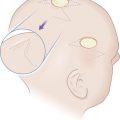
The unique anatomy of the eyelids and supporting structures present unique challenges to the periocular surgeon. The eyelids are conceptually divided into anterior and posterior lamella for purposes of reconstruction. The posterior lamella, composed of mucosa and tarsus, also houses numerous glands vital for producing the tear film, which is essential for clear vision. The anterior lamella is composed of the orbicularis oculi muscle and skin, with minimal retinaculum in between. The orbicularis oculi is contiguous with the lateral canthal tendon, a fibrous tissue that tethers the tarsal plates to the bony orbit. The lateral canthal tendon attaches to the inside of the orbital rim at Whitnall tubercle, a bony prominence where additional suspensory ligaments, essential for opening and closing the lids, also converge. Whitnall tubercle can be palpated manually and is an important point of fixation for suspension and fixation of the of the lateral canthal tendon fundamental to many periocular repairs ( Fig. 12.1 ). The medial canthal tendon bifurcates into anterior and posterior limbs, which diverge around the lacrimal sac to facilitate the lacrimal pump before attaching to the anterior and posterior aspects of the bony lacrimal crest. Familiarity with the complex anatomy of the medial canthal region is essential to preserve lacrimal drainage.

The vascular supply of the periorbital region is ample and facilitates a low infection rate and rapid healing of repairs in this area. The internal and external carotid arteries and veins provide vascular supply to the eyelids and surrounding tissue via numerous branches, including the dorsal nasal artery medially and the temporal and transverse facial arteries laterally that anastomose to form the marginal arcades of the eyelids. The sensory nerves of the eye emanate from ophthalmic and maxillary branches of the trigeminal nerve. Motor innervation required for both movement and constitutive tone of the periocular muscles is supplied by branches of the facial, oculomotor, and sympathetic nerves.
Tension
Preoperative, intraoperative, and postoperative assessments of the tensional forces around the eye are essential to prevent complications that may impact vision and cosmetic outcomes. Indeed, even the smallest tensional forces on the lid margin, created primarily or secondary to adjacent wound contraction, can lead to ectropion and webbing. The limits of tension can be assessed preoperatively by performing a “snap test,” in which the lid is pulled away from the globe and watching the rate of return, which correlates with the degree of laxity. Assessing maximal tension intraoperatively is also prudent, so that adjustments can be made and suspension sutures used to ensure tensional limitations are not exceeded. Forceps can be used to approximate wound edges prior to closure and tension assessed again after key sutures are placed. Maximal tension can be assessed by asking the patient to look up while opening the mouth widely (see Fig. 12.3 ). If the lid pulls away from the globe, then adjustments can be made before the surgery is completed. Additional support can be achieved intraoperatively by placing deep sutures in the cutaneous retinaculum and fascia to reinforce horizontal support and minimize downward pull on the eyelid. However, most importantly, the power of suspension sutures placed in the fascia, periosteum, and canthal support tissues to minimize tension around the eye cannot be overstated. Examples of periocular suspension sutures will be highlighted throughout this chapter.
Periocular Repairs
There are many ways to approach the repair of defects located around the eye. Keeping incisions perpendicular to the lid margin and designing flaps that push tissue towards the lid margin and limit downward pull is the cornerstone of avoiding ectropion in periocular surgery ( Figs. 12.2 and 12.3 ). It is also important to oversize flaps and grafts adequately to accommodate for convexities, eye movement, and facial expression. The choice of closure often depends on a number of factors, including the size, depth, location of the defect and tissue reservoirs, skin laxity, and stability of the canthal tissues. Despite these variables, fundamental principles and techniques of reconstruction in the periocular area can be followed to optimize outcomes and avoid complications of webbing and ectropion (see Fig. 12.3 ).


Linear Repairs
Repairing wounds in a linear fashion around the eye often requires a balance of obscuring incisions in relaxed skin tension lines (RSTLs) and directing tension parallel to the lid margin. Below the lid, vertical incisions can be designed increasingly oblique to the lid margin from medial to the lateral where incisions become more horizontal (see Fig. 12.2 ), excepting the medial canthus, where horizontal incisions are strictly avoided to prevent webbing. M-plasty repairs can also help to manage redundant cones near the lid margin when needed. Below the eye, removing less of the redundant tissue at the apex of the ellipse can also help to protect against ectropion. Small defects located on the upper lid crease can often be repaired with a crescent-shaped incision along the natural crease similar to a traditional blepharoplasty (keeping incisions medial to the caruncle to avoid webbing and extending beyond the lateral canthus when hooding is present).
Skin Grafts
Full-thickness skin grafts can be useful when primary closures are not possible but must be well designed and supported in the perioperative period. In general, skin grafts must be oversized by 30% to allow for wound contracture and avoid ectropion. More precise sizing can be achieved by putting the eyelid on stretch and using a sterile nonstick gauze pad as a blotter to create a graft template. The ideal donor site is the ipsilateral or contralateral upper lid and can be harvested with a typical blepharoplasty incision. Larger grafts can be harvested from the prearuicular, supraclavicular, and inner arm area. Grafts can be thinned, fenestrated, and tacked to the base to optimize inosculation. Canthopexy sutures can be useful to prevent ectropion. Frost sutures can be helpful to support the low lid immediately postoperatively. Dental wax or petroleum gauze bolsters can be useful to provide gentle pressure. Split thickness skin grafts are generally not recommended due to skin contraction.
Flap Repairs
Defects Below the Lid Margin
Rhomboid transposition flaps that “push” tissue towards the lid margin are a staple for repairing small and medium defects located below the eyelid ( Fig. 12.4 ). Rhomboid flaps must be adequately sized to accommodate for upgaze, maximal tension, and wound contraction to reliably avoid complications of ectropion. Tension-free incisions heal well and are often obscured, despite crossing cosmetic unit boundaries and rhytids, owing to ample vascular supply and rapid healing. Transposition flaps based on skin within the orbit are useful for central defects that are very close to the lid margin, where they soundly direct tension superiorly ( Fig. 12.5 ). More lateral defects can be repaired with transposition flaps based on the redundant skin of the upper lid crease ( Fig. 12.6 ). Canthal suspension sutures can be used to provide additional support when indicated. Laterally based rotation flaps can be useful for defects exceeding the limits of the upper lid reservoir ( Fig. 12.7 ).