Pemphigoid gestationis is a rare, autoimmune bullous disease of pregnancy that involves autoantibodies directed against type XVII collagen in the basement membrane zone. This article discusses the immunopathogenesis, diagnostic methods, and clinical features of this fascinating disease.
Pemphigoid gestationis (PG), formerly known as herpes gestationis, is a rare autoimmune blistering disease (AIBD) of pregnancy. It was first described in 1872 by Dr John Laws Milton, founder of the St John’s Hospital for Diseases of the Skin in London, stemming a team of subsequent experts in the condition from this institution, in particular Dr Martin Black. Recent advances have shown this disease to be similar to the pemphigoid group of diseases in terms of clinical and immunologic features. The specific dermatoses of pregnancy have since been reclassified and pemphigoid gestationis is the current terminology used. Since then, there have been a number of case reports and large case series on this disease.
Epidemiology
The incidence of PG is very low, estimated at approximately 1 case per 50,000 pregnancies. Reports are variable, but the disease commonly presents in the second or third trimester of pregnancy. In a review of 505 women with specific dermatoses of pregnancy, 21 were diagnosed with PG, with 48% of cases occurring in primigravid women. Disease onset was typically during the third trimester (71%), and less commonly during the second trimester (29%). In another case series of 117 patients with PG, the mean age of patients was 28 years, with 17.9% presenting in the first trimester, 34.2% in the second trimester, 34.2% in the third trimester, and 13.7% during the postpartum period. There are also reports of this disease occurring in women with trophoblastic tumors, hydatidiform mole, or choriocarcinoma.
Immunopathogenesis
In normal pregnancies, there is a state of homeostasis between the mother and the fetus, whereby the mother tolerates the genetically and immunologically different fetal tissue growing inside her. Changes to this tightly regulated immune state of the mother during pregnancy may lead to the development of various autoimmune diseases, one of which is PG. Fetal trophoblastic cells are typically devoid of major histocompatibility complex (MHC) class 1 and 2 molecules, and this is to ensure that the maternal immune system does not mount an immune response against the growing fetus. The major target antigen in PG is collagen XVII (BP180), a transmembrane hemidesmosomal glycoprotein, which is found in the basement membranes of the skin and the amniotic epithelium of placental tissues. In a recent immunohistochemical study of the basement membrane zone and dermal extracellular matrix of normal amnion, BP180 was found to be greatly reduced in comparison with nonreproductive epithelium. This self-antigen is presented to the maternal immune system by abnormally expressed HLA class 2 molecules in the placenta. Antibodies, mainly immunoglobulin-G (IgG) and complement C3, are formed against the extracellular noncollagenous 16A (NC16A) domain of the 180-kd target antigen. This is the same immunodominant region of BP180 that is involved in bullous pemphigoid. Earlier reports state that the main IgG subclasses involved are IgG1 and IgG3, but more recently, with the use of sandwich double antibody immunofluorescence (SDAI), the predominant subclass identified is IgG4. IgG4 is the subclass that can cross the placenta, so if the infant had gradually developed an immune response to the mother’s different BP180 sequence, this might explain why it only develops several months into pregnancy and why it would disappear after delivery. A more recent paper has identified IgE antibodies reactive against the NC16A domain of BP180. The epitope profile of PG includes other target sites on the BP180 molecule outside of the NC16A domain. In a paper by Zambruno and colleagues, PG sera bound to a total of 8 epitopes in the intracellular domain (ICD) and extracellular domain (ECD) by immunologic screening analyses and enzyme-linked immunosorbent assay (ELISA). There have also been reports of IgA autoantibodies directed against the C-terminal portion of the BP180 ectodomain in a PG patient with extensive oral involvement. In addition, sera of PG patients may recognize the BP230 antigen.
Epitope spreading upon exposure of the BP180 molecule to the maternal immune system may account for these additional autoantigens, as is described in other AIBD. None of these studies had sequenced the infant’s BP180 gene to see if there was a polymorphism from a paternal allele that may have allowed the infant to recognize the mother’s BP180 as foreign. The latter would fit with the history of 50% of pregnancies being affected in large families, as there would be a 50% chance of the fetus inheriting a polymorphism from the father. Such polymorphisms have been found in patients with other AIBD, such as pemphigus foliaceus. Upon binding to the target antigen, IgG activates the classical complement pathway, resulting in tissue injury and blister formation. This is evidenced by deposition of C3 along the basement membrane zone during direct immunofluorescence.
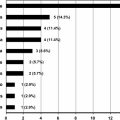
PG is associated with the presence of maternal MHC class 2 antigens DR3 and DR4. A study done in the United States on 23 patients with PG showed that 61% of patients express HLA-DR3; 52% express HLA-DR4, and 43% express a combination of HLA-DR3/DR4. This observation seems to be similar across ethnic groups, and has been reported in 8 Mexican patients with PG. In a review of 22 cases of PG in Kuwait, predominance of HLA-DR3 and DQ2 antigens were observed, with no predominance of HLA-DR4. They have also found anti-HLA antibodies to paternal HLA molecules in all cases studied.
Related posts:
 A Globally Available Internet-Based Patient Survey of Pemphigus Vulgaris: Epidemiology and Disease Characteristics
A Globally Available Internet-Based Patient Survey of Pemphigus Vulgaris: Epidemiology and Disease Characteristics
 Diagnosis and Clinical Features of Pemphigus Foliaceus
Linear IgA Disease: Clinical Presentation, Diagnosis, and Pathogenesis
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
Diagnosis and Clinical Features of Pemphigus Foliaceus
Linear IgA Disease: Clinical Presentation, Diagnosis, and Pathogenesis
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
 Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


