Pedicled Perforator Flaps in Breast Reconstruction
Moustapha Hamdi
Introduction
Since the mid-1990s, the advent of perforator flaps has expanded the horizons of reconstructive microsurgery. Harvesting a flap without sacrificing the underlying muscle or the functional motor nerves characterizes this technique, which aims to reduce donor-site morbidity to an absolute minimum. Although the thoracodorsal (TD) and intercostal (IC) arteries provide many perforators to the region of the back, only the latissimus dorsi (LD) muscle or musculocutaneous flap is in common use in breast surgery, despite resulting in loss of the largest muscle in the body. Pedicled perforator flaps are no longer a new concept. These flaps have been widely used for breast reconstruction in our department. This chapter reviews the concept of pedicled perforator flaps and their use in breast reconstruction.
Anatomy
The TD vessels are the main pedicle of the LD muscle. After giving off the serratus anterior (SA) branch, the TD vessel divides into two branches: the descending or vertical branch and the horizontal branch (Fig. 63.1A). These branches give off several perforators to the skin of the back. Anatomic studies on cadavers have shown that the vertical intramuscular branch provides two or three musculocutaneous perforators. The proximal perforator pierces the muscle, enters the subcutaneous tissue approximately 8 cm distal to the posterior axillary fold and 2 to 3 cm posterior to the anterior border of the muscle, and is oriented obliquely as it passes from deep to superficial. The second perforator originates 2 to 4 cm distal to the first perforator and, along with the first, is found consistently in most people. Our clinical experience with the thoracodorsal artery perforator (TDAP) free flap has demonstrated the occasional occurrence of a direct perforator (septal or paramuscular perforator) arising from the thoracodorsal vessel, which passes around the anterior border of the LD muscle into the skin. Because the perforator does not pierce the LD muscle, there is no need for intramuscular dissection, making flap harvest rapid and simple.
Intercostal perforators are found anterior to the border of the LD, permitting harvest of a perforator flap without disturbing or sacrificing the thoracodorsal vessels. Until recently, there have been no additional anatomic studies of the IC perforators in the upper trunk. Our cadaver dissection showed a variable number of IC perforators that can be clinically used in the area between the LD and PM muscles. A “dominant perforator” was identified in most cadavers (92%). These dominant perforators were located in the fourth to the eighth ICSs, with a higher concentration in the sixth and seventh ICSs. The dominant perforators are located an average of 3.5 cm from the anterior border of the latissimus dorsi muscle. Retrograde dissection of the dominant perforator revealed that it travels obliquely under a slip of the origin of the SA muscle into the intercostal space deep to the internal and external intercostal muscles. Once deep to the intercostal muscles, it emerges from the subcostal groove. The dominant perforator typically had a smaller posterior branch, which bifurcated above the SA muscle. This branch was found to communicate with the TD perforators or SA vessels. When it bifurcated under the SA muscle (in 10% of cases), it had a similar diameter to the anterior branch.
The branch to SA gives few perforators to the skin, some of which may communicate with intercostal perforators. This vascular connection was found between the SA branch and the intercostal perforators in 21% of the cases. This connection was noted more frequently in the seventh ICS and the sixth ICS in 38% and 30% of cases, respectively. The perforator blood supply to the skin of the back and lateral chest is schematically represented in Figure 63.1A.
Classification of Flaps
Perforator flaps (Figs. 63.1 and 63.2) were classified according to the nutrient artery as recommended by the Gent consensus in 2002:
Thoracodorsal artery perforator (TDAP) flap
Lateral intercostal artery perforator (LICAP) flap
Serratus anterior artery perforator (SAAP) flap
Variable segments of LD muscle may need to be included in the flap due to anatomic variation that only becomes apparent preoperatively. Muscle-sparing latissimus dorsi (MS-LD) flaps were classified as follows:
MS-LD-TDAP I, where a small piece of LD muscle (4 cm × 2 cm) is incorporated within the flap
MS-LD-TDAP II, where a larger segment of up to 5 cm width is designed along the anterior border of the LD muscle
MS-LD-TDAP III, where a larger area of LD muscle is harvested
Figures 63.2E to 63.2G demonstrate the various muscle-sparing flaps.
Indications
Many patients with breast or thoracic defects traditionally treated with an LD musculocutaneous flap are suitable candidates for pedicled perforator flaps. The indications can be summarized as follows:
Partial breast reconstruction, whether immediate or following wider excision in cases of histologically involved margins
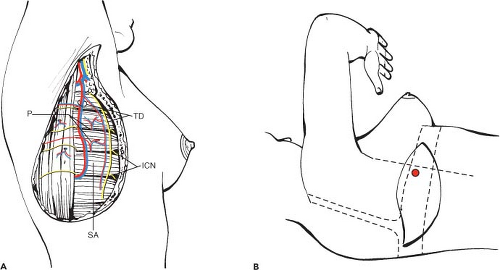
Figure 63.1. A: Vascular anatomy. ICN, intercostal nerve; P, perforator; SA, serratus anterior; TD, thoracodorsal. B: Flap design. The perforator is located using unidirectional Doppler and is usually found 6 to 8 cm from the posterior axillary fold. The flap is designed within the bra region (dotted line) and crosses the anterior border of the latissimus dorsi muscle (dashed line).
Correction of breast deformity after breast-conserving surgery (tumorectomy and radiotherapy)
Thoracic coverage after radical excision
Salvage procedure after significant partial necrosis of free flap for breast reconstruction
Postmastectomy breast reconstruction with or without an implant
Autogenous breast augmentation
Contraindications
There are few contraindications to perforator flap surgery in breast reconstruction. An adequate expertise in perforator flap harvest is requisite, and surgeons may choose to familiarize themselves by first harvesting other perforator flaps, such as the deep inferior epigastric artery perforator or superior gluteal artery perforator flaps, which have relatively larger and more numerous perforators that allow some margin for error.
Defects located at the inferomedial quadrant of the breast are difficult to reach using a pedicled perforator flap and may be better treated by other techniques. Furthermore, thin patients with large breast defects may not be suited to perforator flaps due to a lack of sufficient flap volume.
Damage to the TD pedicle due to previous axillary or thoracic surgery is an absolute contraindication to raising a TDAP flap, as it is for a traditional LD flap; however, an LICAP flap may still be harvested for lateral defects on the breast. Previous surgery to the axilla or lung (lateral thoracotomy) or radiotherapy to the region may also result in damage to the perforator complexes.
Surgical Approach
Preoperative Assessment
The patient is marked on the day before surgery. Breast size, tumor size, tumor location, and the estimated defect size are all taken into account. The thickness of the skin and fat of the back is determined by the pinch test. Doppler examination is performed with the patient lying in a lateral position, similar to that during surgery (Fig. 63.1B), with the arm abducted to 90 degrees. A 5- to 8-mHz handheld Doppler probe allows accurate location of perforators with a strongly audible signal. The perforators are usually found based on the vertical branch of the thoracodorsal vessel, in all cases within 5 cm of the anterior border of the LD muscle and between 7 and 10 cm from the posterior axillary line. The flap is designed to include the audible perforators and lies in the direction of the lines of relaxed skin tension, or it can be oriented more horizontally according to the desires of the patient. The perforator flap should always extend over the anterior border of the LD muscle to include any paramuscular perforators that may be present. The width of the flap is determined by the size of the defect and the preference for primary donor-site closure.
Operative Technique
The patient is placed in a lateral decubitus position with the arm free-draped and abducted to 90 degrees, as though harvesting a traditional LD myocutaneous flap. Simultaneous tumor resection and flap harvest is possible if the required flap size can be accurately predicted before resection. Skin and
subcutaneous tissue are incised down to the level of the muscle fascia, and the initial dissection is beveled outward to maximize flap volume. Flap elevation proceeds from distal to proximal and from medial to lateral at the level just above the LD muscle fascia until the preoperatively identified perforator or another good size perforator is located (Fig. 63.3A).
subcutaneous tissue are incised down to the level of the muscle fascia, and the initial dissection is beveled outward to maximize flap volume. Flap elevation proceeds from distal to proximal and from medial to lateral at the level just above the LD muscle fascia until the preoperatively identified perforator or another good size perforator is located (Fig. 63.3A).
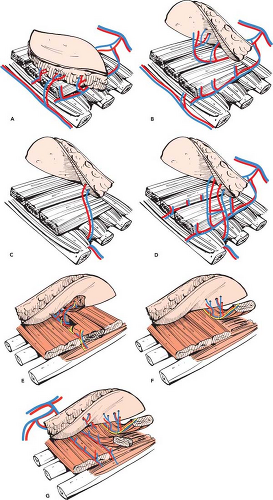 Figure 63.2. Classification of flaps. A: The various nutrient artery sources and perforator branches are marked. Thoracodorsal, serratus anterior, and intercostal vessels are represented diagrammatically. B: Thoracodorsal artery perforator flap. C: Lateral intercostal artery perforator flap. D: Serratus anterior artery perforator flap. E: Muscle-sparing latissimus dorsi Muscle-sparing latissimus dorsi thoracodorsal artery perforator (MS-LD-TDAP) I flap. F: MS-LD-TDAP II flap. G: MS-LD-TDAP III flap. |
Thoracodorsal Artery Perforator Flap
A perforator originating from the vertical branch is preferred because dissection is easier due to fewer connections with branches of the thoracodorsal nerve, and also the intramuscular vessel course is usually shorter. If two perforators lie along the same line, both can be incorporated within the flap without cutting any additional muscle fibers. A perforator should be visibly pulsatile and have an adequate diameter (>0.5 mm). If the surgeon is satisfied with the caliber and the quality of the perforator complex and committed to harvesting the perforator flap, the perforator vessel is fully dissected. The anterosuperior skin paddle is left attached to the patient’s skin to avoid undue tension on the perforator complex. The muscle is split along the line of its fibers and the perforator dissected cranially (Fig. 63.3B). Side branches are ligated or coagulated with microbipolar diathermy, whereas nerve branches are dissected away from the vessels and preserved. The perforator usually runs in a loose areolar-fatty tissue and is traced back to the
thoracodorsal pedicle (Fig. 63.3C). The TD vessels can be dissected proximally to the origin from the subscapular vessel if a long pedicle is required, sufficient to reach even the most distal breast defects. The serratus anterior branch may require ligation if it hinders adequate mobility of the flap. Once dissection of the vessels is complete, the skin paddle is carefully passed through the split LD muscle (Fig. 63.3D), then subcutaneously through the axillary region into the breast defect (Fig. 63.3E). Extreme care should be taken to avoid damage to the perforator complex during subcutaneous passage of the flap. If a perforator originating from the TD vessels and passing around the anterior border of the LD muscle into the skin is identified, dissection is made easier, and the entire flap can be raised without disturbing the LD muscle.
thoracodorsal pedicle (Fig. 63.3C). The TD vessels can be dissected proximally to the origin from the subscapular vessel if a long pedicle is required, sufficient to reach even the most distal breast defects. The serratus anterior branch may require ligation if it hinders adequate mobility of the flap. Once dissection of the vessels is complete, the skin paddle is carefully passed through the split LD muscle (Fig. 63.3D), then subcutaneously through the axillary region into the breast defect (Fig. 63.3E). Extreme care should be taken to avoid damage to the perforator complex during subcutaneous passage of the flap. If a perforator originating from the TD vessels and passing around the anterior border of the LD muscle into the skin is identified, dissection is made easier, and the entire flap can be raised without disturbing the LD muscle.
Related posts:
 Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
 Breast Implants: Materials and Manufacturing Past, Present, and Future
Breast Implants: Materials and Manufacturing Past, Present, and Future
 Reconstruction of the Irradiated Breast
Reconstruction of the Irradiated Breast
 Perforator Flaps in Breast Reconstruction
Perforator Flaps in Breast Reconstruction
 Management of Chronic Postoperative Breast Pain
Management of Chronic Postoperative Breast Pain
 The Periareolar Approach to Augmentation Mammaplasty
The Periareolar Approach to Augmentation Mammaplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


