Pectoralis Major Flap for Pharyngeal Reconstruction
Michael A. Howard
Babak J. Mehrara
DEFINITION
The pectoralis major muscle flap was first reported by Pickrell in 19471 and popularized for head and neck reconstruction by Ariyanas a myocutaneous flap in 1979.2,3
While free tissue transfer remains the standard for many head and neck defects, this pedicled flap is useful for reconstruction of partial pharyngeal defects due to the proximity of the donor site to the recipient area as well as the fact that this flap is usually not in the radiation field in patients with recurrent tumors.
The pectoralis flap is also useful in cases in which microsurgery is not feasible or if coverage of the neck is required in complex reconstructions.
The flap has the advantages of a healthy robust muscle with reliable vascular anatomy, simple harvest technique, and a wide arc of rotation.
Goals of pharyngeal reconstruction:
Achieve primary wound healing
Maintain oral continence and facilitate swallowing while avoiding redundant pouches along food path
Prevent aspiration
Protect vital neck structures
ANATOMY
The pectoralis major is a fan-shaped muscle of the anterior chest which functions to adduct and medially rotate the arm (FIG 1).
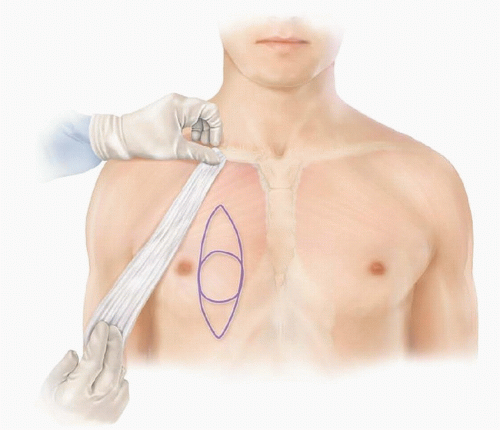
FIG 1 • Anatomy of the pectoralis major myocutaneous flap.
The pectoralis muscle inserts into the medial one-third of the clavicle as well as the sternum and cartilaginous portions of ribs 1 to 6.
The muscle originates as a tendinous insertion into greater tubercle of the humerus. The muscle in this area runs deep to the deltoid muscle, and the cleft that is formed between these two structures is referred to as the deltopectoral groove.
The pectoralis muscle has a Mathes and Nahai type 5 blood supply, composed of a dominant pedicle (the thoracoacromial artery and vein) as well as secondary minor pedicles arising from parasternal perforators arising from the internal mammary artery and vein.
The motor nerve supply of the pectoralis muscle is derived from the medial and lateral pectoral nerves.
PATIENT HISTORY AND PHYSICAL FINDINGS
A number of factors should be considered during flap selection and design.
Defect location. The arc of rotation of the pectoralis flap can be estimated by locating the pedicle of the flap and using a lap pad or suture that is held to the tip of the designed flap. The location of the pedicle can be marked by drawing a line from the acromioclavicular joint to the xiphoid. In most patients, a vertically drawn pectoralis myocutaneous flap can easily the upper portion of the hypopharynx.
Size of defect. The pectoralis flap is not easily tubularized due to the thickness of the skin flap and muscle, as well as donor site complications arising from harvesting very wide skin flaps, and as a result, is not in most cases useful for circumferential defects.
Prior chest surgery is also an important consideration since this may have resulted in scars that may decrease the utility of the flap or, less commonly, have injured the blood supply.
The use of this flap in women for pharyngeal reconstruction is also complicated by the presence of breast tissue, and a history of breast cancer (and screening) should be elicited in these patients.
This is not a good option in patients with large breasts as the thickness of the flap complicates wound closure and may result in an unsightly donor defect.
Smoking history does increase the risk of complications, and if possible, smoking should be stopped as long as possible prior to surgery (however, this may not always be feasible in patients with active tumors).
IMAGING
Imaging is rarely necessary for the planning or design of a pectoralis major flap.
SURGICAL MANAGEMENT
Preoperative Planning
Patients who are referred for pharyngeal reconstruction have primary tumors of the hypopharynx/pharynx or suffer from aggressive or recurrent tumors of the surrounding structures (eg thyroid or larynx).
In many cases, the planned procedure involves laryngectomy and end tracheostomy and repair of the pharyngeal defect.
Because the posterior wall of the larynx is closely adhered to the anterior wall of the pharynx, a strip of the pharyngeal wall is commonly resected with the laryngeal specimen.
These patients are good candidates for pectoralis myocutaneous flap reconstruction.
Similarly, the pectoralis flap is a good option in patients with small tumors of the pharynx in which a partial pharyngeal resection is performed.
Patients with more extensive defects of the pharynx that require tubularization of a flap or reconstruction of nearly the entire circumference of the pharynx are better served with a free flap (tubularized anterolateral thigh or jejunum).
Defects of the pharynx extending below the clavicle are most commonly reconstructed with a gastric pull-up or colon interposition flap.
Once a suitable surgical candidate for a pectoralis flap is identified (usually after preoperative consultation with the head and neck oncologist), the patient is examined to assess the quality of the neck skin and subcutaneous tissues.
Many patients who present for reconstruction of pharyngeal defects have previously undergone chemoradiation for laryngeal organ preservation and, as a result, have radiation damage to the skin. In these cases, plans should be discussed not just for reconstruction of the pharyngeal defect but also the overlying skin.
Positioning
The patient is positioned supine, and the bed may be rotated 90 degrees to allow easy access to the head and neck area.
Surgery is performed under general anesthesia often after end tracheostomy has been placed.
TECHNIQUES
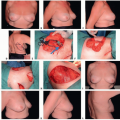
▪ Flap Design
The defect is assessed for viability of the mucosal edges (TECH FIG 1A).
The size of the defect is carefully measured, and the arch of rotation of the flap is assessed as discussed above to ensure tension-free closure.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree