Partial Breast Reconstruction With Local Tissue Rearrangement
Moustapha Hamdi
DEFINITION
The treatment of breast cancer is an evolving field. Different modalities are continuously being developed to maximize patient survival while minimizing the treatment’s morbidity.1,2,3,4,5
Currently, the two main options for the management of primary breast cancer are total mastectomy and lumpectomy/quadrantectomy with radiation.1,2,3,4,5
Studies have shown that women diagnosed at early stages of invasive breast cancer have equivalent outcomes when they are treated with lumpectomy and radiation therapy or modified radical mastectomy.2,3,4,5
Oncoplastic surgery is a combination of breast conservative surgery and an immediate partial breast reconstruction.6
This chapter reviews partial breast reconstruction after partial mastectomy.
ANATOMY7
The Blood Supply
The blood supply of the breast is a rich anastomotic network derived from the axillary, internal thoracic (internal mammary), and two intercostal arteries.
Multiple factors can influence how robust each of these sources of inflow may be (age, endocrine activity, overall health, systemic diseases, eg, diabetes/atherosclerosis, smoking, radiotherapy).
The major inflow sources, from medial to lateral, are the internal mammary segmental perforators, the intercostal perforators, the thoracoacromial perforators, and the external mammary artery.
The anteromedial and anterolateral intercostal perforators are major contributors to the vascularization of the nippleareola complex (NAC).
The venous drainage is a dual system: a superficial subdermal plexus, which eventually meets up in the deep system, and a deep system, which accompanies the mentioned arterial system.
The Nerve Supply
The medial and central breast sensations come from the second through the sixth anteromedial intercostal nerves.
The nipple-areola sensation is contributed by the third, fourth, and fifth anteromedial and anterolateral intercostal nerves.
Careful consideration of the nerve supply helps to maximize nipple sensation. When pedicled flaps (see Chapter 22) are passed into partial mastectomy defects, the tunnel should be created high enough to avoid lateral denervation to the breast.
PATIENT HISTORY AND PHYSICAL FINDINGS
Breast and plastic surgeons must have a thorough understanding of breast anatomy, physiology, and the qualities of an aesthetically pleasing breast shape.
Surgeons performing the oncoplastic approach should consider the aesthetic subunits when planning cosmetic quadrectomies, resections, and reconstructions.
Also, knowledge of the anatomical landmarks, breast proportions, and shape is essential to achieve a pleasing outcome.
Preoperative evaluation of the patient and her breasts must be standard and detailed.
The examination must include the following:
Evaluation of breast skin, elasticity, thickness, scars, and any defining marks such as tattoos, stretch marks, contour irregularities, and previous breast surgery should be taken into account when planning breast-conserving therapy (BCT).
Palpation for masses or abnormalities in the breast parenchyma, nipple inspection, and detailed documentation of breast sensation are integral.
Breast shape, grade of ptosis, and size are determinants of success in surgical treatment.
The base and width of the breast, the width of the NAC, the height of the nipple, and the distance from the sternal notch, midline and inframammary crease, must be recorded in detail.
Any natural breast asymmetry should be pointed out to the patient before surgery.
Different body types, skin laxity, and fat distribution are important factors in the decision-making process.
SURGICAL MANAGEMENT
Oncological Approach
Indications: Most early-stage cancers (T1 and T2 cancers with or without nodal involvement) are indicated for BCT.6,8
Contraindications: Patients with a high probability for recurrence, especially those with multicentric disease, those who are pregnant or have collagen vascular disease, or those who have a history of prior radiation therapy.6,8
Relative contraindications include the following:
Patients with a high probability of subsequent cancers (BRCA mutations)
Patients who are likely to have a poor cosmetic result, which includes patients with a high tumor/breast ratio
Medially and inferiorly based tumors
Tumors that require removal of the NAC
Clinical Approach
The success of this procedure depends on the size of the cancer, the anatomical position, and the volume of resection needed to achieve clear margins in relation to the volume of the breast.
The choice of the technique used depends on many factors, including the extent of resection, the time of surgery, the breast size and tumor location, and patient preferences.
Preoperatively, incision lines and preservation of the NAC should be discussed with the oncologic surgeon and patient.
The estimation of the defect size after tumor resection and breast size/tumor ratio is a guideline to the choice of the reconstructive method (FIG 1).
Immediate correction of asymmetry by a contralateral mastopexy or reduction should also be discussed (Table 1).
There are two basic types of surgery techniques in partial breast reconstruction: volume displacement and volume replacement.
Volume displacement techniques refer to advancement, rotation, or transposition of large local breast flaps into the smaller created defect, redistributing the volume loss. The dissection involves the advancement of a full-thickness segment of breast fibroglandular tissue to fill the dead space. Volume displacement procedures and surgical scars are optimal when combined with mastopexy-reduction techniques. The tumor is excised within the planned markings of the reduction specimen in medium, large, or ptotic breasts, and the remaining parenchyma is sufficient enough to reshape the breast mound.
Volume replacement techniques are technically more difficult and are used in small to moderate-size breasts or when the tumor/breast ratio is large and the remaining breast tissue is insufficient for the rearrangement and the replacement of the defect. Volume replacement with the use of nonbreast local or distant flaps provides both tissue for the filling of the glandular defect and the skin deficiency of the reconstructed breast (see Chapter 22).
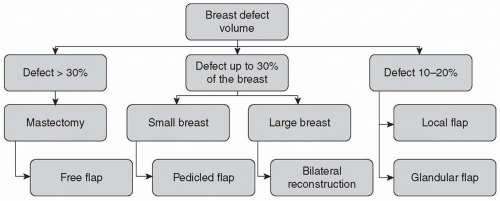 FIG 1 • An algorithm to partial breast reconstruction. |
Table 1 Important Considerations in Partial Breast Reconstruction | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


